Management of 1st degree heart block
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of first-degree heart block management:
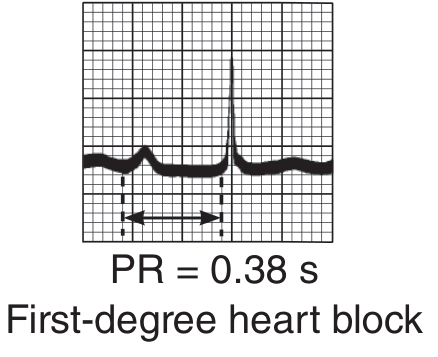
First-Degree Heart Block (First-Degree AV Block)
Definition & ECG Features
PR interval > 0.20 seconds (200 ms) in adults, with all atrial impulses conducted to the ventricles (no dropped beats). PR intervals as long as 1.0 second have been documented.
Pathophysiology
The conduction delay can reside in:
- AV node (most common) — especially when QRS is narrow and normal in contour
- His-Purkinje system — suspected when QRS shows a bundle branch block pattern; requires His bundle electrogram to confirm
- Both sites simultaneously, or rarely within the atria
Causes / Associated Conditions
| Category | Examples |
|---|---|
| Physiological | Well-trained athletes (increased vagal tone) — can be normal |
| Drugs | Beta-blockers, digoxin, calcium channel blockers, amiodarone |
| Structural heart disease | Inferior MI, myocarditis, rheumatic fever |
| Electrolyte disturbances | Hypercalcemia (acute/severe) |
| Infiltrative/genetic | Arrhythmogenic RV cardiomyopathy, Ebstein anomaly |
| Congenital |
Management
1. No treatment is required in the vast majority of cases.
First-degree AV block is generally a benign finding and does not cause hemodynamic compromise on its own. All impulses are conducted; ventricular rate is normal.
2. Identify and address the underlying cause:
- Drug-induced: Review medications. Offending agents include beta-blockers (e.g., betaxolol, esmolol, propranolol), digoxin, amiodarone, and non-dihydropyridine calcium channel blockers. Withhold or dose-reduce if clinically appropriate.
- Inferior MI or ischaemia: Monitor closely; AV nodal block in this context is often transient and resolves with reperfusion.
- Electrolyte abnormality: Correct hypercalcemia or other metabolic disturbances.
- Myocarditis / rheumatic fever: Treat underlying infection/inflammation.
3. Monitor for progression:
Acceleration of the atrial rate or enhanced vagal tone can cause first-degree AV nodal block to progress to type I second-degree AV block (Wenckebach). Conversely, it can revert to first-degree block with slowing of the sinus rate. Serial ECG monitoring is warranted in symptomatic patients or those with structural heart disease.
4. No pacemaker is indicated for isolated first-degree AV block.
- Pacemaker implantation is reserved for symptomatic higher-degree AV block (second-degree Mobitz II, third-degree).
- First-degree block alone is not an indication for pacing.
5. Contraindications to note:
First-degree AV block is commonly listed as a contraindication to drugs that further slow AV conduction (e.g., greater than first-degree block is required before some of these are absolutely contraindicated, but caution applies):
- Betaxolol, esmolol, propranolol — contraindicated in greater than first-degree block, but caution with first-degree if symptomatic
- Digoxin — use with caution; may worsen AV conduction
Prognosis
- In healthy individuals and athletes: benign, often vagally mediated.
- In structural heart disease: prognosis is determined by the underlying disease, not the block itself.
- In chronic isolated second-degree AV nodal block (proximal to His bundle) without structural disease: generally benign course, though worsens with age.
Sources: Braunwald's Heart Disease (15e), Ganong's Review of Medical Physiology (26e), Barash Clinical Anesthesia (9e), Harriet Lane Handbook (23e)
This is a shared conversation. Sign in to Orris to start your own chat.