Show top 10 ECG CHANGES AND EXPLAIN WITH PICTURES
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
top 10 ECG changes clinical examples with pictures ST elevation LBBB atrial fibrillation
Reading File
Reading File
Searching the Web
ECG changes site:ecgwaves.com OR site:litfl.com atrial fibrillation ventricular tachycardia heart block WPW diagrams images
Loading Image
Loading Image
Searching the Web
STEMI ECG ST elevation inferior anterior lateral leads diagram litfl ecgwaves site:litfl.com OR site:ecgwaves.com
Loading Image
Loading Image
Searching the Web
ECG LBBB left bundle branch block WPW ventricular tachycardia hyperkalemia peaked T wave LVH images site:litfl.com
Loading Image
Loading Image
Searching the Web
ECG ventricular tachycardia complete heart block QT prolongation torsades de pointes pulmonary embolism S1Q3T3 images litfl
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive guide to the Top 10 Most Important ECG Changes, each explained with real ECG examples.
Top 10 ECG Changes: Clinical Guide with Pictures
1. ST-Segment Elevation (STEMI)
What it is: Elevation of the ST segment above the isoelectric line by ≥1 mm in limb leads or ≥2 mm in precordial leads, indicating acute transmural myocardial ischemia/infarction.
Key leads by territory:
- Inferior STEMI - II, III, aVF (RCA or LCx occlusion) - with reciprocal ST depression in aVL
- Anterior STEMI - V1-V4 (LAD occlusion)
- Lateral STEMI - I, aVL, V5-V6
Clinical significance: STEMI is a time-critical emergency. Each minute of delay worsens outcome. Door-to-balloon time <90 min is the target.
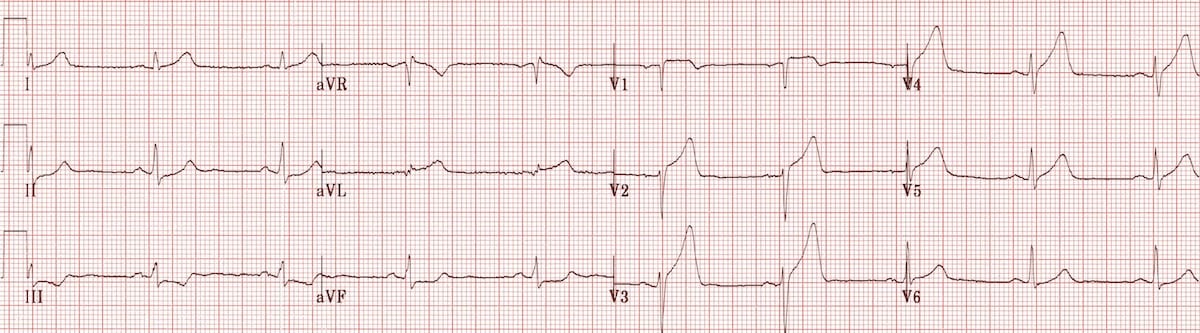
Inferior STEMI - hyperacute phase:
 Note: Hyperacute ST elevation in leads II, III, aVF with reciprocal changes (ST depression) in aVL - classic inferior STEMI pattern
Note: Hyperacute ST elevation in leads II, III, aVF with reciprocal changes (ST depression) in aVL - classic inferior STEMI pattern
Anterolateral STEMI - hyperacute phase:
 Note: Massive ST elevation across V2-V6 indicating large anterior wall involvement (proximal LAD occlusion)
Note: Massive ST elevation across V2-V6 indicating large anterior wall involvement (proximal LAD occlusion)
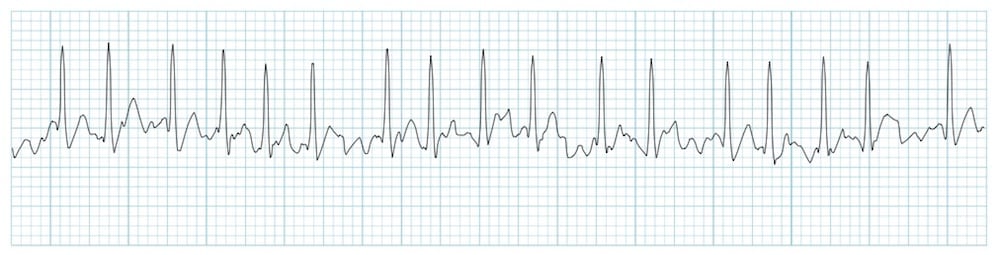
2. Atrial Fibrillation (AF)
What it is: The most common sustained cardiac arrhythmia, characterized by chaotic atrial electrical activity.
ECG features:
- No distinct P waves - replaced by irregular fibrillatory baseline (f-waves)
- Irregularly irregular RR intervals - the hallmark
- Ventricular rate typically 100-170 bpm (if uncontrolled)
- Narrow QRS (unless aberrant conduction or accessory pathway)
Clinical significance: AF increases stroke risk 5-fold. Requires anticoagulation assessment (CHA₂DS₂-VASc score) and rate or rhythm control.
3. Complete (Third-Degree) AV Block
What it is: Complete dissociation between atrial and ventricular activity - no supraventricular impulse conducts to the ventricles.
ECG features:
- P waves present at a regular rate (e.g., 80 bpm)
- QRS complexes present at a slower, independent rate (20-40 bpm if junctional/ventricular escape)
- P waves and QRS have no relationship to each other (AV dissociation)
- Wide QRS if ventricular escape; narrow QRS if junctional escape (block at AV node)
Clinical significance: Hemodynamically unstable. Requires urgent pacing. Common causes: inferior STEMI, Lyme disease, drugs (beta-blockers, digoxin), idiopathic fibrosis.
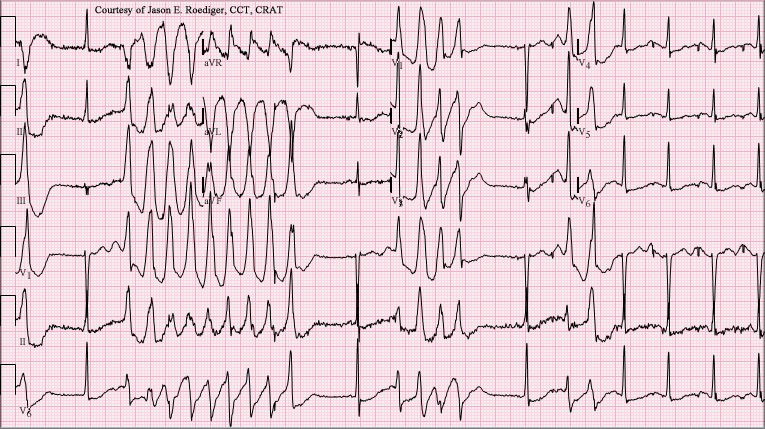
The image above shows a 12-lead with complete heart block (note the dissociated P waves and wide escape complexes) transitioning into Torsades de Pointes - illustrating how bradycardia from complete block can trigger dangerous arrhythmias.
4. Ventricular Tachycardia (VT)
What it is: Wide complex tachycardia originating below the bundle of His at a rate >100 bpm.
ECG features:
- Rate: 100-250 bpm
- Wide QRS (>120 ms) - bizarre morphology
- Regular rhythm (usually)
- AV dissociation (P waves seen independent of QRS - pathognomonic)
- Fusion beats and capture beats (Dressler beats) confirm VT
- Extreme axis deviation
Key distinction from SVT with aberrancy: Use Brugada criteria or Verecki criteria. AV dissociation on 12-lead = VT until proven otherwise.
Clinical significance: Life-threatening. Pulseless VT = defibrillation. Stable VT = amiodarone or cardioversion. Sustained VT with structural heart disease = high SCD risk.
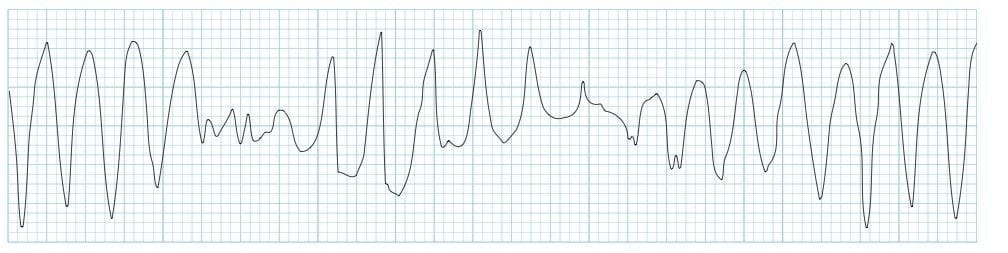
5. Torsades de Pointes (TdP)
What it is: A specific polymorphic VT occurring in the context of prolonged QT interval, where QRS complexes "twist" around the isoelectric baseline.
ECG features:
- Polymorphic, wide QRS complexes
- Amplitude cyclically waxes and wanes ("twisting" appearance)
- Rate 200-250 bpm
- Typically initiated by a short-long-short R-R sequence
- Preceded by a prolonged QT interval
Common causes of long QT: Drugs (antiarrhythmics, antipsychotics, antibiotics), hypokalemia, hypomagnesemia, congenital LQTS, complete heart block.
6. Prolonged QT Interval
What it is: Lengthening of ventricular repolarization, predisposing to TdP and sudden cardiac death.
Normal QTc values:
- Males: QTc < 450 ms
- Females: QTc < 460 ms
- Dangerous: QTc > 500 ms (high TdP risk)
Bazett's formula: QTc = QT / √RR interval
ECG features:
- Long interval from start of QRS to end of T wave
- May show T-wave abnormalities (bifid T, notched T, prominent U wave)
- The T-wave may be flat or inverted

7. Left Bundle Branch Block (LBBB)
What it is: Failure of conduction through the left bundle branch, causing abnormal left ventricular depolarization.
ECG features (all required for "complete LBBB"):
- QRS duration ≥ 120 ms (wide)
- Broad monophasic R wave in lateral leads (I, aVL, V5-V6)
- rS or QS pattern in V1 (no R wave, or very small r)
- No septal Q waves in lateral leads
- Discordant ST-T changes (ST/T goes opposite to main QRS deflection)
Clinical significance: New LBBB in acute chest pain warrants urgent evaluation (Sgarbossa criteria used to identify AMI within LBBB). Associated with cardiomyopathy, CAD, hypertension.
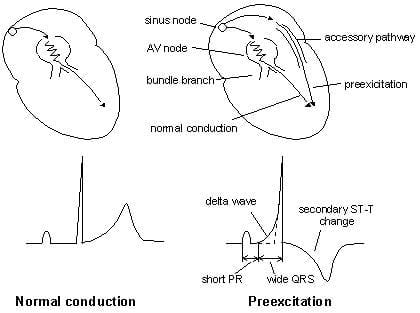
8. Wolff-Parkinson-White (WPW) Syndrome
What it is: Pre-excitation due to an accessory pathway (Bundle of Kent) bypassing the AV node.
ECG features (in sinus rhythm):
- Short PR interval (< 120 ms) - due to bypassing AV node delay
- Delta wave - slurred upstroke at beginning of QRS
- Wide QRS (> 120 ms) - due to early ventricular depolarization
- Secondary ST-T changes (discordant to QRS)
Clinical significance: Can cause AVRT (orthodromic or antidromic) or AF with rapid ventricular response (potentially fatal). Avoid AV nodal blocking agents (adenosine, verapamil, digoxin) in WPW with AF - may precipitate VF. Definitive treatment = radiofrequency ablation.
9. Hyperkalemia
What it is: Elevated serum potassium (>5.5 mmol/L) causing progressive ECG changes that can lead to cardiac arrest.
ECG changes in progressive order:
| Potassium (mmol/L) | ECG Change |
|---|---|
| 5.5 - 6.5 | Peaked (tent-shaped) T waves - narrow base, symmetric |
| 6.5 - 7.5 | PR prolongation, QRS widening, P wave flattening |
| 7.5 - 8.5 | P waves disappear, sine-wave QRS pattern |
| > 9.0 | Ventricular fibrillation, asystole |
Clinical significance: Life-threatening above ~7.0 mmol/L. ECG changes may precede lab results. Emergency treatment: IV calcium gluconate (membrane stabilization), insulin + dextrose, sodium bicarbonate, salbutamol, dialysis.
Mnemonic - Follow the ECG trace: T peaks → PR lengthens → P flattens → QRS widens → sine wave → VF
10. Pulmonary Embolism - S1Q3T3 Pattern
What it is: Right heart strain pattern seen in large/massive PE, reflecting acute right ventricular pressure overload.
Classic S1Q3T3 pattern:
- S wave in lead I (new or deepening)
- Q wave in lead III
- T-wave inversion in lead III
Additional PE changes (more sensitive):
- Sinus tachycardia (most common ECG finding)
- Right heart strain: T-wave inversions in V1-V4, right axis deviation
- RBBB (complete or incomplete) - due to RV dilation
- P pulmonale (peaked P waves in II)
- S1Q3T3 (specific but only in ~20% of PEs)
Clinical significance: ECG alone cannot diagnose or exclude PE. It helps risk-stratify. Massive PE with RV strain on ECG indicates higher mortality. Confirmation requires CT pulmonary angiography (CTPA).
Quick Reference Summary Table
| # | ECG Change | Key Feature | Main Cause | Emergency Action |
|---|---|---|---|---|
| 1 | STEMI | ST elevation + reciprocal changes | Coronary occlusion | PCI/thrombolysis |
| 2 | Atrial Fibrillation | Irregularly irregular, no P waves | HTN, valve disease | Rate control + anticoagulation |
| 3 | Complete AV Block | P-QRS dissociation, bradycardia | Ischemia, drugs, fibrosis | Emergency pacing |
| 4 | Ventricular Tachycardia | Wide complex tachycardia, AV dissociation | Structural heart disease | Cardioversion/amiodarone |
| 5 | Torsades de Pointes | Twisting polymorphic VT | Long QT, drugs | Magnesium IV, overdrive pacing |
| 6 | Prolonged QT | Long QT interval (>500 ms dangerous) | Drugs, electrolytes, congenital | Remove cause, Mg, monitor |
| 7 | LBBB | Wide QRS, no Q in lateral, rS in V1 | CAD, cardiomyopathy | Sgarbossa if acute chest pain |
| 8 | WPW | Short PR, delta wave, wide QRS | Accessory pathway | Ablation; avoid AV nodal drugs |
| 9 | Hyperkalemia | Peaked T waves → sine wave | Renal failure, drugs | Ca gluconate + K removal |
| 10 | Pulmonary Embolism | S1Q3T3, RV strain, sinus tach | DVT, immobility | CTPA, anticoagulation, thrombolysis |
Sources: Harrison's Principles of Internal Medicine 22E; Braunwald's Heart Disease; LITFL ECG Library; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.