he patient is a 58-year-old male with a 10-year history of Type 2 diabetes (on Metformin 1000mg twice daily), hypertension (on Amlodipine 5mg), and recently tarted experiencing chest tightness, mild shortness of breath on exertion, occasion dizziness, and swelling in both ankles over the past 3 weeks. His last HbAlc was 8.2 BP today is 148/92 mmHg, and my fasting blood sugar this morning was 210 mg/dL He also smoke half a pack a day and have a family history of heart disease. What could be going on, and what should I do?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Searching PubMed
type 2 diabetes heart failure cardiovascular outcomes SGLT2
I now have comprehensive, authoritative information to give a thorough clinical answer. Let me synthesize everything.
⚠️ Important Disclaimer
This response is for educational purposes only and does not substitute for professional medical evaluation. This patient must be seen urgently by a physician - his symptom complex warrants prompt clinical assessment and likely urgent cardiac workup.
Clinical Assessment: What Is Likely Going On
This 58-year-old male presents with a high-risk cardiovascular profile. His constellation of symptoms - chest tightness, exertional dyspnea, bilateral ankle edema, and occasional dizziness over 3 weeks - combined with uncontrolled Type 2 diabetes (HbA1c 8.2%, FBS 210 mg/dL), hypertension (148/92 mmHg), active smoking, and a family history of heart disease, points to a serious, potentially multi-faceted cardiac problem. Three overlapping diagnoses must be considered simultaneously:
1. Ischemic Heart Disease / Angina (Most Urgent Priority)
Chest tightness + exertional dyspnea + dizziness in a diabetic male with hypertension, smoking, and family history = high pretest probability for coronary artery disease (CAD).
Key facts from Harrison's (22E, 2025):
"ASCVD, including PAD, CHD, heart failure, and cerebrovascular disease, occurs more frequently in individuals with type 1 or type 2 DM and is the major cause of mortality for individuals with diabetes... CHD is more likely to involve multiple vessels in individuals with DM."
Critically, silent ischemia is common in diabetics due to autonomic neuropathy. His chest tightness may actually be an atypical anginal equivalent or even an evolving acute coronary syndrome (ACS). As Harrison's states:
"The absence of chest pain ('silent ischemia') is common in individuals with diabetes, and a thorough cardiac evaluation should be considered."
2. Heart Failure (Possibly Developing)
Bilateral ankle edema + exertional dyspnea are classic signs of early heart failure. With 10 years of diabetes and longstanding hypertension, he is at significant risk for:
- HFpEF (preserved ejection fraction) - most common in diabetic/hypertensive patients
- HFrEF (reduced ejection fraction) - if there has been silent ischemic myocardial injury
- Diabetic cardiomyopathy - occurs without CHD or hypertension; Harrison's notes: "Some individuals with DM have reduced left ventricular function without CHD or hypertension"
Goldman-Cecil Medicine confirms: "Heart failure is related to diabetes duration and hypertension and can present as HFpEF, HFmEF, or HFrEF."
Using the AHA/ACC Heart Failure Staging Framework below, this patient has likely progressed from Stage A to Stage C:
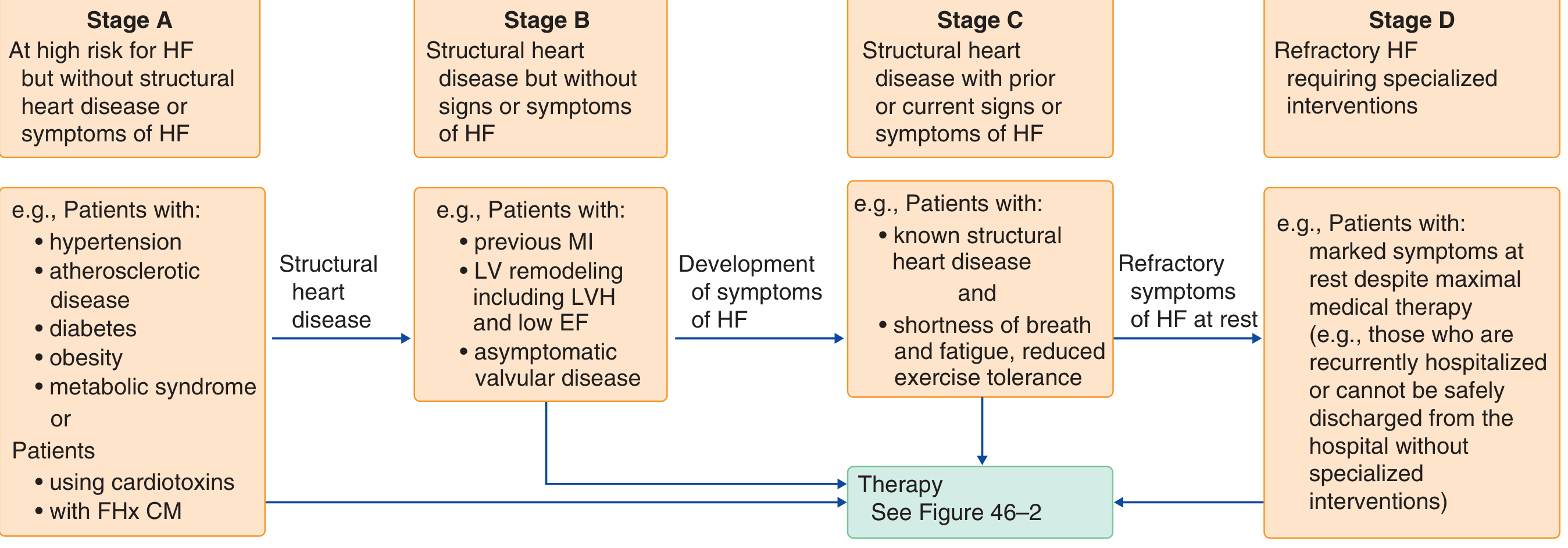
He has Stage A risk factors (diabetes, hypertension, family history) and is now developing Stage C symptoms (structural disease with current exertional dyspnea and edema).
3. Poorly Controlled Cardiovascular Risk Factors
| Risk Factor | Status | Target |
|---|---|---|
| HbA1c | 8.2% (uncontrolled) | <7.0% (ADA), or individualized |
| BP | 148/92 mmHg (elevated) | <130/80 mmHg in diabetics |
| FBS | 210 mg/dL (high) | 80-130 mg/dL (fasting) |
| Smoking | 0.5 ppd (active) | Complete cessation |
| LDL/lipids | Unknown - likely dyslipidemic | LDL <70 mg/dL (high risk) |
What Should Be Done: Step-by-Step Action Plan
IMMEDIATE (Within Hours - Same Day)
1. Emergency evaluation is needed NOW.
- The combination of chest tightness + dyspnea + dizziness must rule out ACS (unstable angina / NSTEMI / STEMI) first.
- Go to an Emergency Department or call emergency services if the chest tightness worsens, occurs at rest, radiates to the arm/jaw, or is accompanied by sweating or nausea.
2. Urgent baseline investigations:
- 12-lead ECG - look for ST changes, LVH, ischemia, arrhythmia
- Troponin I/T (serial) - rule out myocardial injury/ACS
- BNP or NT-proBNP - elevated in heart failure
- CBC, BMP/CMP - electrolytes, renal function (eGFR), glucose
- Lipid panel (likely never optimized)
- Chest X-ray - cardiomegaly, pulmonary edema
- Urinalysis + spot urine albumin:creatinine - diabetic nephropathy?
SHORT-TERM (Days to Weeks)
3. Cardiac workup:
- Echocardiogram - assess ejection fraction, wall motion, valves, LV hypertrophy
- Cardiac stress test (exercise treadmill or pharmacological if unable to exercise) - evaluate for inducible ischemia
- Cardiology referral - mandatory given his risk profile and active symptoms
4. Medication review and optimization:
Per Harrison's (22E), for a type 2 diabetic with ASCVD or high ASCVD risk, the treatment approach should address four concurrent targets - glycemia, blood pressure, lipids, and cardioprotective agents:
Glycemia:
- Metformin 1000mg BID can continue if eGFR > 30 mL/min/1.73m²
- Add an SGLT-2 inhibitor (e.g., empagliflozin, dapagliflozin) - Harrison's explicitly recommends this: "If diabetic CKD or heart failure is present or likely, an SGLT-2 inhibitor is preferred." These drugs reduce heart failure hospitalizations and cardiovascular mortality. Recent 2024 meta-analyses in Circulation (PMID: 39210781) and Lancet Diabetes Endocrinol (PMID: 38991584) confirm additive benefit of SGLT-2 inhibitors ± GLP-1 agonists for cardiovascular and kidney outcomes in T2DM.
- Consider adding a GLP-1 receptor agonist (e.g., semaglutide, liraglutide) for additional cardiovascular risk reduction
Blood Pressure:
- Current 148/92 mmHg is well above the <130/80 mmHg target in diabetics
- Amlodipine alone is insufficient - add an ACE inhibitor or ARB (e.g., lisinopril, ramipril, or losartan). These have additional renoprotective and cardioprotective effects in diabetics.
- If heart failure confirmed: ACE inhibitor/ARB + beta-blocker is the backbone of therapy (Harrison's: "treatment... should involve a cardiovascular specialist and include treatment with an ACE inhibitor or ARB and a beta blocker")
Lipids:
- Likely needs a high-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) - per ADA guidelines in Harrison's, with a goal LDL <70 mg/dL (or <55 mg/dL if ASCVD confirmed)
Antiplatelet:
- At age 58 with multiple risk factors: aspirin 75-100 mg/day is reasonable for primary prevention; becomes mandatory secondary prevention if ASCVD confirmed (Harrison's ADA recommendation)
ONGOING MANAGEMENT
5. Lifestyle modifications (non-negotiable):
- Smoking cessation - this is the single most impactful change he can make. Smoking doubles cardiovascular risk on top of his already high burden.
- Cardiac-protective diet (Mediterranean or DASH)
- Regular moderate-intensity aerobic exercise (after cardiac clearance)
- Weight management
6. Monitoring schedule:
- HbA1c every 3 months until target achieved, then every 6 months
- BP at every visit
- Annual lipid panel, urine albumin, eGFR, eye exam, foot exam
- Repeat echo in 6-12 months after therapy optimization
Summary of Differential Diagnoses
| Diagnosis | Key Supporting Features | Urgency |
|---|---|---|
| Acute Coronary Syndrome | Chest tightness, dyspnea, DM (silent ischemia risk), family hx | Emergent - rule out first |
| Stable angina / CAD | Exertional symptoms, multiple risk factors | Urgent workup |
| Heart failure (HFpEF/HFrEF) | Bilateral ankle edema, dyspnea, DM + HTN duration | Urgent - echo needed |
| Diabetic cardiomyopathy | 10 yr DM, poor glycemic control | Evaluate with echo |
| Hypertensive heart disease | LVH from chronic HTN | Evaluate with ECG/echo |
| Peripheral edema (other causes) | Less likely given cardiopulmonary symptoms | Lower priority |
Bottom Line
This patient should not wait for a routine appointment. His chest symptoms combined with diabetes, uncontrolled blood pressure, active smoking, and family history of heart disease make ACS a real possibility that must be excluded urgently. Once ACS is ruled out, a thorough cardiac workup (echo + stress test) will clarify whether he has established CAD, heart failure, or both - and will guide the significant medication optimization that is clearly needed. A cardiology referral is strongly warranted.
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill), p. 3271; Goldman-Cecil Medicine International Edition, pp. 461-462; Neuen et al., Circulation 2024 [PMID: 39210781]; Apperloo et al., Lancet Diabetes Endocrinol 2024 [PMID: 38991584].
This is a shared conversation. Sign in to Orris to start your own chat.