What is meant by subclinical/ inapparent infection
Reading File
Searching the Web
subclinical inapparent infection definition microbiology
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Here is a thorough explanation of subclinical/inapparent infection, drawn from authoritative medical textbook sources.
Subclinical / Inapparent Infection
Definition
A subclinical (inapparent) infection is the entry and multiplication of an infectious agent in a host that produces no recognizable signs or symptoms of disease. The pathogen is present and replicating, the host mounts an immune response, yet the clinical manifestations remain below the threshold of detection by ordinary examination.
"Infection in which the symptoms are sufficiently mild or inapparent to escape diagnosis other than by positive confirmation of the ability to transmit the infection." - Park's Textbook of Preventive and Social Medicine
Levels of Infection (Context)
Infection exists along a continuum of host-pathogen interaction. Park's classifies the levels as:
| Level | Description |
|---|---|
| Colonization | Organism present on surface, no tissue invasion (e.g., S. aureus in the nasopharynx) |
| Subclinical / Inapparent | Pathogen multiplies, immune response occurs, no symptoms (e.g., polio) |
| Latent infection | Organism persists in host in a dormant state (e.g., herpes simplex) |
| Clinical / Manifest infection | Full-blown symptomatic disease |
Key Features
- Pathogen actively replicates - This is not merely colonization. The organism invades tissue and the body responds.
- Immune response does occur - Antibodies are produced, and the individual acquires immunity just as they would from clinical disease.
- Not detectable clinically - Requires laboratory methods (serology, PCR, culture) to confirm.
- Can still transmit - The infected individual may shed the pathogen and transmit it to others, making subclinical cases an important reservoir in the community.
Subclinical Infection and the Spectrum of Disease
The "spectrum of disease" concept places subclinical infections at one end and fatal illness at the other:
"At one end of the disease spectrum are subclinical infections which are not ordinarily identified, and at the other end are fatal illnesses. In the middle of the spectrum lie illnesses ranging in severity from mild to severe. These different manifestations are simply reflections of individuals' different states of immunity and receptivity." - Park's Textbook, p. 50
In infectious diseases, this spectrum is also called the "gradient of infection."
The Iceberg Phenomenon
Subclinical infections are the hidden bulk of the "iceberg of disease":
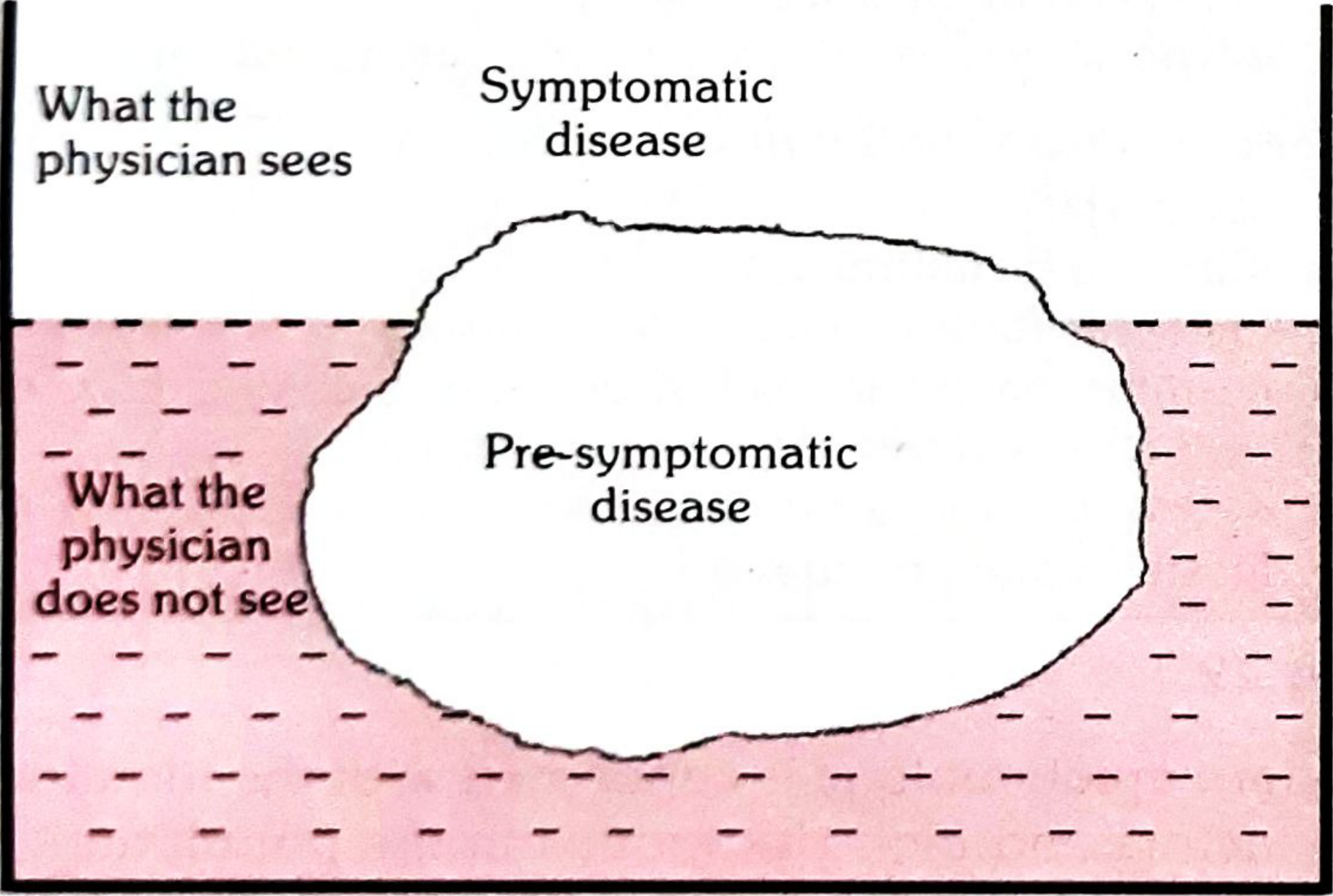
Fig. 10 - The Iceberg of Disease (Park's Textbook)
- The tip above water = symptomatic (clinical) cases the physician sees
- The submerged portion = latent, inapparent, presymptomatic, and undiagnosed cases + carriers
- The waterline = the boundary between apparent and inapparent disease
This hidden mass constitutes an important undiagnosed reservoir of infection in any community.
Classic Examples
- Poliomyelitis: The most cited example. Only ~1% of poliovirus infections result in paralysis. The vast majority are subclinical. For every clinical paralytic case, there may be 1,000 subclinical cases in children and 75 in adults (Park's, p. 243). During inapparent infection, the virus is shed in faeces and can be transmitted to others.
- Mumps: During subclinical infection, the patient can still transmit the virus to others, and individuals with subclinical mumps acquire full immunity (Jawetz Melnick & Adelberg's Medical Microbiology, 28e).
- Diphtheria, Rubella, Hepatitis A, COVID-19 - all have high rates of inapparent infection.
Epidemiological Importance
- Source of spread: Subclinical cases often outnumber clinical cases and, because they go undetected, they are a major driver of community transmission.
- Natural immunity: Subclinical infection confers immunity, contributing to herd immunity without clinical illness.
- Active immunity acquisition: Active immunity can be acquired following subclinical infection (e.g., polio, diphtheria), without the person ever knowing they were infected.
- Challenge to control: Because these cases are invisible to surveillance, they make disease control and eradication more difficult.
Summary
| Feature | Subclinical Infection |
|---|---|
| Pathogen present | Yes |
| Replication in host | Yes |
| Symptoms | None / below detection threshold |
| Immune response | Yes (antibodies formed) |
| Immunity acquired | Yes |
| Can transmit to others | Yes |
| Detectable by | Lab tests (serology, PCR, culture) |
| Epidemiological role | Major hidden reservoir; drives spread |
- Park's Textbook of Preventive and Social Medicine, pp. 105, 50, 243
- Jawetz Melnick & Adelberg's Medical Microbiology, 28e
How colonization is different from carrier state
Finding Sources
Searching the Web
colonization vs carrier state microbiology difference epidemiology
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Excellent - I now have rich textbook content to compile a comprehensive answer.
Colonization vs. Carrier State
These two terms are closely related but represent distinct host-microbe relationships. The confusion arises because a carrier is often colonized, but not every colonized person is a carrier.
1. Colonization
Definition: The presence and multiplication of a microorganism on or in the body (skin, mucous membranes, gut) without causing disease or an immune response, and without implying the organism is pathogenic.
Key features:
- The organism occupies a niche on body surfaces (external or internal)
- No tissue invasion, no harm, no symptoms
- No immune response is necessarily triggered
- The organism may be part of the normal microbiota (commensal/symbiotic)
- Can be transient (brief, easily displaced) or resident (stable, long-term occupancy)
- Does NOT imply a carrier state - colonization on a body surface does not automatically mean the person can transmit disease (Park's, p. 105)
Examples:
- S. aureus in the skin and normal nasopharynx
- Streptococcus pneumoniae or Neisseria meningitidis in the throat of 5-40% of healthy people - these may represent transient flora, resident flora, OR carrier state; "whether these bacteria represent transient flora, resident flora, or carrier state is largely semantic" (Sherris & Ryan's Medical Microbiology, 8e)
- C. difficile colonization in healthy infants (25-80% colonization rates with no disease)
2. Carrier State
Definition: A person who harbors a pathogen (an organism known to cause disease), sheds it, and can transmit it to others - all without showing clinical signs of disease themselves.
Key features:
- The organism involved is known to be pathogenic
- The carrier actively sheds (excretes) the infectious agent via faeces, urine, respiratory secretions, blood, etc.
- Transmission to susceptible contacts is possible and a real epidemiological risk
- The carrier themselves may have no symptoms
As defined by Sherris & Ryan's Medical Microbiology:
"The term carrier state is used when organisms known to be potentially pathogenic are involved, although its implication of risk is not always justified."
Core Distinction at a Glance
| Feature | Colonization | Carrier State |
|---|---|---|
| Organism type | Commensal or opportunist | Known pathogen |
| Tissue invasion | No | No (but organism present at a site) |
| Symptoms in host | None | None |
| Immune response | Minimal/none | May be present (antibodies) |
| Shedding / transmission | Not necessarily | Yes - sheds organism to others |
| Disease risk to others | Low / uncertain | Real and defined |
| Epidemiological importance | Moderate | High |
| Always implies carrier state? | No | - |
Types of Carriers (Park's Textbook Classification)
A. By Type:
-
Incubatory carrier - Sheds the pathogen during the incubation period (before symptoms appear). Examples: measles, mumps, polio, hepatitis B, influenza.
-
Convalescent carrier - Continues to shed after clinical recovery (bacteriological recovery lags behind clinical recovery). Example: typhoid fever patient may shed bacilli for 6-8 weeks after recovery.
-
Healthy carrier - Emerges from subclinical infection; never had overt disease but sheds the pathogen. Examples: poliomyelitis, cholera, meningococcal meningitis, diphtheria.
- Important note: A person with subclinical infection may or may not become a carrier. In polio, a subclinical case may act as a temporary carrier. In tuberculosis, most persons with a positive tuberculin test do NOT actively disseminate bacilli and are therefore NOT labelled carriers.
B. By Duration:
| Type | Description | Examples |
|---|---|---|
| Temporary carrier | Sheds for short periods (includes incubatory, convalescent, healthy) | Polio, cholera, pertussis |
| Chronic carrier | Sheds for indefinite/prolonged periods - more epidemiologically dangerous | Typhoid (gallbladder), Hepatitis B, dysentery, malaria |
"Chronic carriers are far more important sources of infection than cases. The longer the carrier state, the greater the risk to the community." - Park's Textbook, p. 105
C. By Portal of Exit:
- Urinary carriers (e.g., typhoid urinary carrier - more dangerous than intestinal)
- Intestinal carriers
- Respiratory/nasal carriers
- Blood-borne carriers
Pseudo-carriers: Carriers of avirulent strains - not epidemiologically significant.
The Important Nuance: Can Colonization Become a Carrier State?
Yes - this is the crux of the conceptual overlap:
- When a colonizing organism is also pathogenic, the line between colonization and carrier state blurs
- In hospital settings, nosocomial bacteria transmitted to a patient may lead to colonization with that organism = a carrier state (Harrison's Principles, 22e)
- MRSA colonization of the nose/skin is explicitly called a "carrier state" because MRSA is a pathogen and can be transmitted to others (Roberts & Hedges' Clinical Procedures)
- The distinction is most meaningful when the colonizing organism is not ordinarily pathogenic in the host, but could infect a vulnerable host
Summary
Colonization = organism present + multiplying + no disease in host + not necessarily transmissible as disease.
Carrier state = pathogen present + no disease in host + actively shed + transmissible to others.
All carriers are colonized, but not all colonized persons are carriers. The carrier state specifically requires that the organism is a known pathogen AND is being shed in a way that poses real transmission risk to the community.
- Park's Textbook of Preventive and Social Medicine, pp. 105, 1556-1564
- Sherris & Ryan's Medical Microbiology, 8e, p. 30
- Harrison's Principles of Internal Medicine, 22e
What is meant by disseminated varicella zoster disease
Finding Sources
Searching the Web
disseminated varicella zoster disease definition clinical features immunocompromised
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive, high-quality textbook content to deliver a thorough answer.
Disseminated Varicella Zoster Disease
Background: VZV Causes Two Distinct Syndromes
Varicella Zoster Virus (VZV) causes:
- Primary infection - Varicella (chickenpox), acquired via respiratory route
- Reactivation - Herpes Zoster (shingles), when latent virus in dorsal root ganglia reactivates
In both forms, disseminated disease refers to the virus spreading far beyond its normal confined pattern - going systemic rather than staying localized.
Definition
Disseminated Herpes Zoster is formally defined as:
"More than 20 lesions outside the affected dermatome."
- Andrews' Diseases of the Skin, 5e, p. 437
It occurs chiefly in older or debilitated individuals, especially those with lymphoreticular malignancy (e.g., Hodgkin's disease, leukemia) or AIDS.
For primary varicella (chickenpox), dissemination refers to progressive varicella with prolonged high-level viremia and visceral organ involvement (lungs, liver, CNS, kidneys), going far beyond the usual self-limited skin rash.
Who Is at Risk?
Dissemination occurs primarily in the immunocompromised:
| Group | Risk Details |
|---|---|
| Hematologic malignancy (Hodgkin's, leukemia) | 5x higher risk of zoster; 12% develop cutaneous dissemination |
| Bone marrow / stem cell transplant | 25% develop disseminated zoster; 10-15% visceral dissemination; overall mortality 5% |
| HIV/AIDS | Zoster 30x more common; ocular/neurologic complications increased; up to 25% develop recurrences |
| Organ transplant (on cyclosporine, tacrolimus, sirolimus, steroids) | Significantly increased risk |
| Neonates (seronegative) | Mortality up to 30% |
| JAK inhibitor therapy | Elevated risk |
A low serum VZV antibody level is a highly significant risk factor for predicting dissemination.
Pathogenesis
In immunocompromised hosts, cell-mediated immunity (CMI) fails to contain viral replication:
- Virus replicates unchecked beyond the initial dermatome or primary rash site
- Prolonged, high-level viremia develops
- Virus seeds visceral organs via the bloodstream
- Results in progressive, extensive cutaneous lesions + visceral organ damage
"Immunosuppressed patients may develop localized shingles followed by dissemination of virus with visceral infection, which resembles progressive varicella." - Sherris & Ryan's Medical Microbiology, 8e, p. 566
Clinical Features
A. Cutaneous Dissemination
- >20 vesicular lesions outside the primary dermatome
- Outlying vesicles/bullae are not grouped, resemble varicella (chickenpox)
- Often umbilicated and may be hemorrhagic or gangrenous
- Dermatomal lesions may be hemorrhagic or gangrenous
- In AIDS: atypical patterns - ecthymatous (punched-out ulcerations) or verrucous lesions
B. Visceral Dissemination
This is the most dangerous form. Organs affected:
| Organ | Manifestation |
|---|---|
| Lungs | VZV pneumonitis - cough, dyspnea, tachypnea, high fever, pleuritic chest pain, cyanosis, hemoptysis; diffuse bilateral peribronchial nodular densities on imaging |
| Liver | Hepatitis - markedly elevated transaminases, sometimes fulminant |
| CNS | Encephalitis - seizures, altered consciousness, focal deficits; also cerebellitis |
| Kidneys | Nephritis |
| Coagulation system | DIC - from mild febrile purpura to fatal purpura fulminans |
Prodromal symptoms of visceral dissemination: Severe abdominal and back pain often precede the rash - an important clinical clue in immunocompromised patients.
C. SIADH Syndrome (Rare)
- Disseminated zoster in stem cell transplant patients can be associated with Syndrome of Inappropriate ADH (SIADH)
- Presents with: hyponatremia + abdominal pain + ileus - sometimes with very few skin lesions ("papules" not vesicles), making diagnosis deceptively difficult
- Can be fatal even with IV acyclovir therapy
Progressive Varicella (Disseminated Primary Infection)
"Immunocompromised children may develop progressive varicella, which is associated with prolonged viremia and visceral dissemination as well as pneumonia, encephalitis, hepatitis, and nephritis. Progressive varicella has an estimated mortality rate of 20%." - Sherris & Ryan's Medical Microbiology, 8e
Key features in immunocompromised patients:
- Continuing eruption of new lesions (normally stops after 5-7 days)
- High fever persisting into second week of illness (normally resolves)
- In thrombocytopenic patients: hemorrhagic skin lesions
- Severe abdominal/back pain as prodrome
Diagnosis
- Clinical: extensive rash beyond dermatome + systemic features in an immunocompromised patient
- PCR of vesicle fluid - most sensitive and specific
- Direct fluorescent antibody (DFA) from vesicle scraping
- Tzanck smear: shows multinucleated giant cells (not VZV-specific)
- Serology (VZV IgM/IgG): less useful in acute setting
- Liver function tests, chest X-ray/CT to assess visceral involvement
Treatment
| Setting | Treatment |
|---|---|
| Disseminated zoster / visceral involvement | IV Acyclovir (10 mg/kg every 8 hours) - start immediately |
| Transition (after visceral involvement excluded + ≥2-3 days IV therapy) | Can step down to oral valacyclovir or famciclovir |
| Immunocompromised patients regardless of time of rash onset | Treat regardless of 72-hour window |
"Disseminated zoster should be treated with IV acyclovir." - Rosen's Emergency Medicine
- Isolation: Contact + Airborne precautions (disseminated zoster is far more contagious than localized zoster)
- Hospital admission is mandatory for disseminated or visceral disease
Prevention in High-Risk Patients
- Pre-transplant VZV IgG serostatus checked - all seropositive transplant patients receive prophylaxis
- Acyclovir 800 mg twice daily or valacyclovir 500 mg twice daily for 1 year post-transplant (or longer if still immunosuppressed)
- VariZIG (VZV immune globulin) given to non-immune immunocompromised patients within 10 days of exposure to VZV
- Recombinant zoster vaccine (Shingrix) - preferred over live vaccine in immunocompromised patients
Summary
| Feature | Localized Zoster | Disseminated Zoster |
|---|---|---|
| Skin involvement | 1-3 dermatomes | >20 lesions outside dermatome |
| Visceral involvement | No | Lungs, liver, CNS, kidneys possible |
| Host | Immunocompetent (usually elderly) | Immunocompromised |
| Treatment | Oral antivirals | IV Acyclovir + hospital admission |
| Isolation | Standard precautions | Airborne + Contact precautions |
| Mortality | Very low | Up to 5-20% depending on extent |
- Andrews' Diseases of the Skin, 5e, p. 437
- Sherris & Ryan's Medical Microbiology, 8e, pp. 565-566
- Fitzpatrick's Dermatology, 9e
- Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.