Notes on emphysema
Reading File
Finding Sources
Searching PubMed
emphysema pathophysiology management
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have all the content needed to write comprehensive notes on emphysema. Let me compile the full notes.
Emphysema - Comprehensive Notes
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine
Definition
Emphysema is defined as permanent, irreversible enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, without significant fibrosis.
- Classified as a COPD (along with chronic bronchitis and asthma)
- Classification is based on anatomic distribution within the lobule (acinus)
- The acinus = structure distal to terminal bronchioles; 3-5 acini = one lobule
Types / Classification
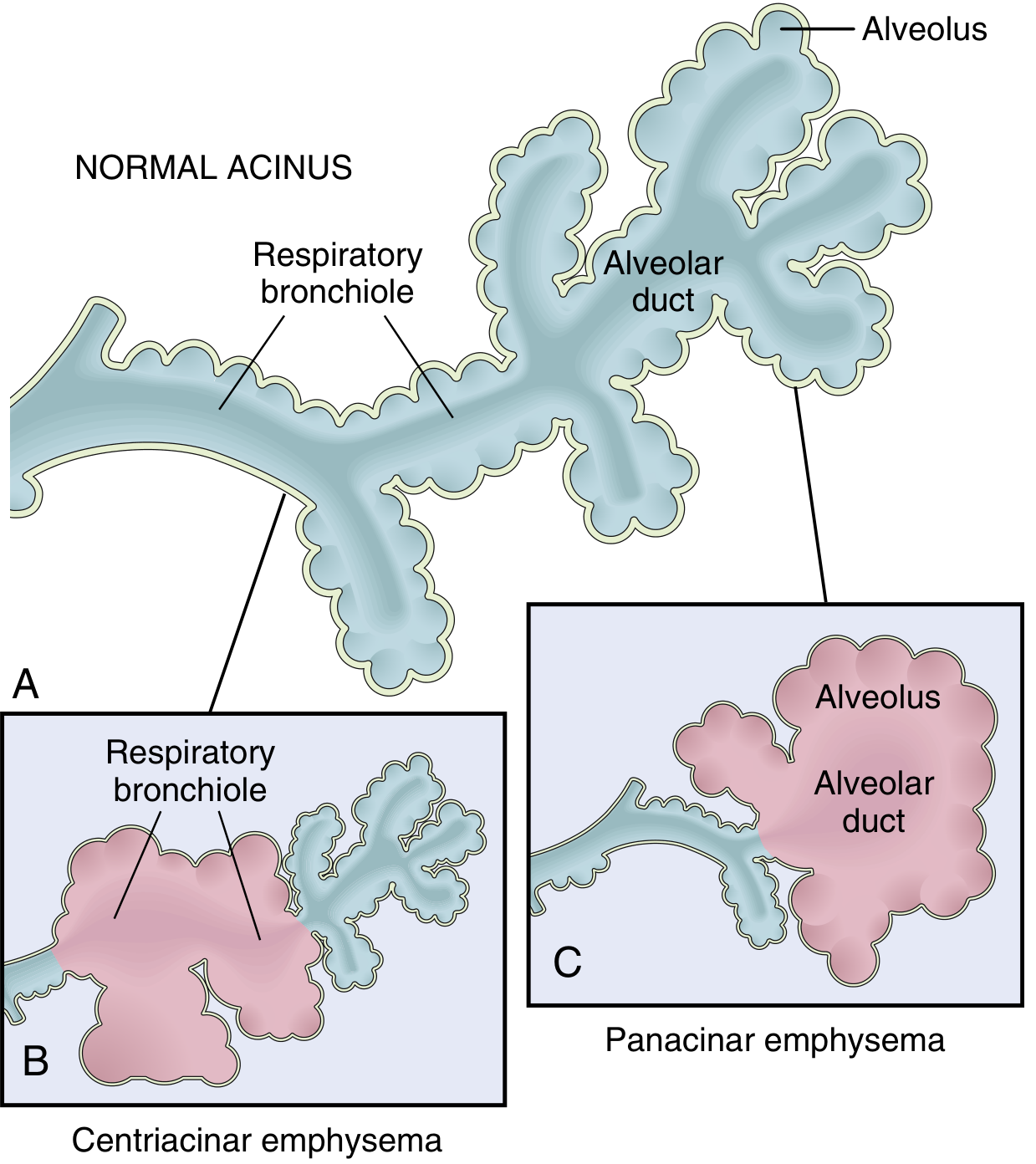
Fig. 15.6 - Patterns of emphysema (A) Normal acinus (B) Centriacinar (C) Panacinar - Robbins, Cotran & Kumar
1. Centriacinar (Centrilobular) Emphysema
- Most common form - >95% of clinically significant cases
- Central/proximal parts of the acinus (respiratory bronchioles) are enlarged; distal alveoli spared
- Both emphysematous and normal airspaces exist within the same acinus
- Distribution: upper lobes, especially apical segments
- Cause: heavy cigarette smoking (most common) + COPD
- Often accompanied by chronic bronchitis
- In severe disease, distal acinus also involved → hard to distinguish from panacinar
2. Panacinar (Panlobular) Emphysema
- Acini are uniformly enlarged - from respiratory bronchiole to terminal blind alveoli
- Distribution: lower lung zones and anterior lung margins; most severe at bases
- Cause: α1-antitrypsin (α1-AT) deficiency (exacerbated by smoking)
- Less common; accounts for ~1% of emphysema cases (α1-AT deficiency)
3. Distal Acinar (Paraseptal) Emphysema
- Proximal acinus is normal; distal part predominantly involved
- Located near pleura, along lobular connective tissue septa, near areas of fibrosis
- Airspaces range from <0.5 mm to >2 cm; form bullae as they enlarge
- Cause: unknown
- Presentation: spontaneous pneumothorax in young adults
- Usually more severe in upper half of lungs
4. Irregular (Paracicatricial) Emphysema
- Irregular acinar involvement; almost always associated with scarring
- Usually clinically insignificant
- Occurs in small foci
Clinical importance: Only centriacinar and panacinar types cause clinically significant airflow obstruction.
Pathogenesis
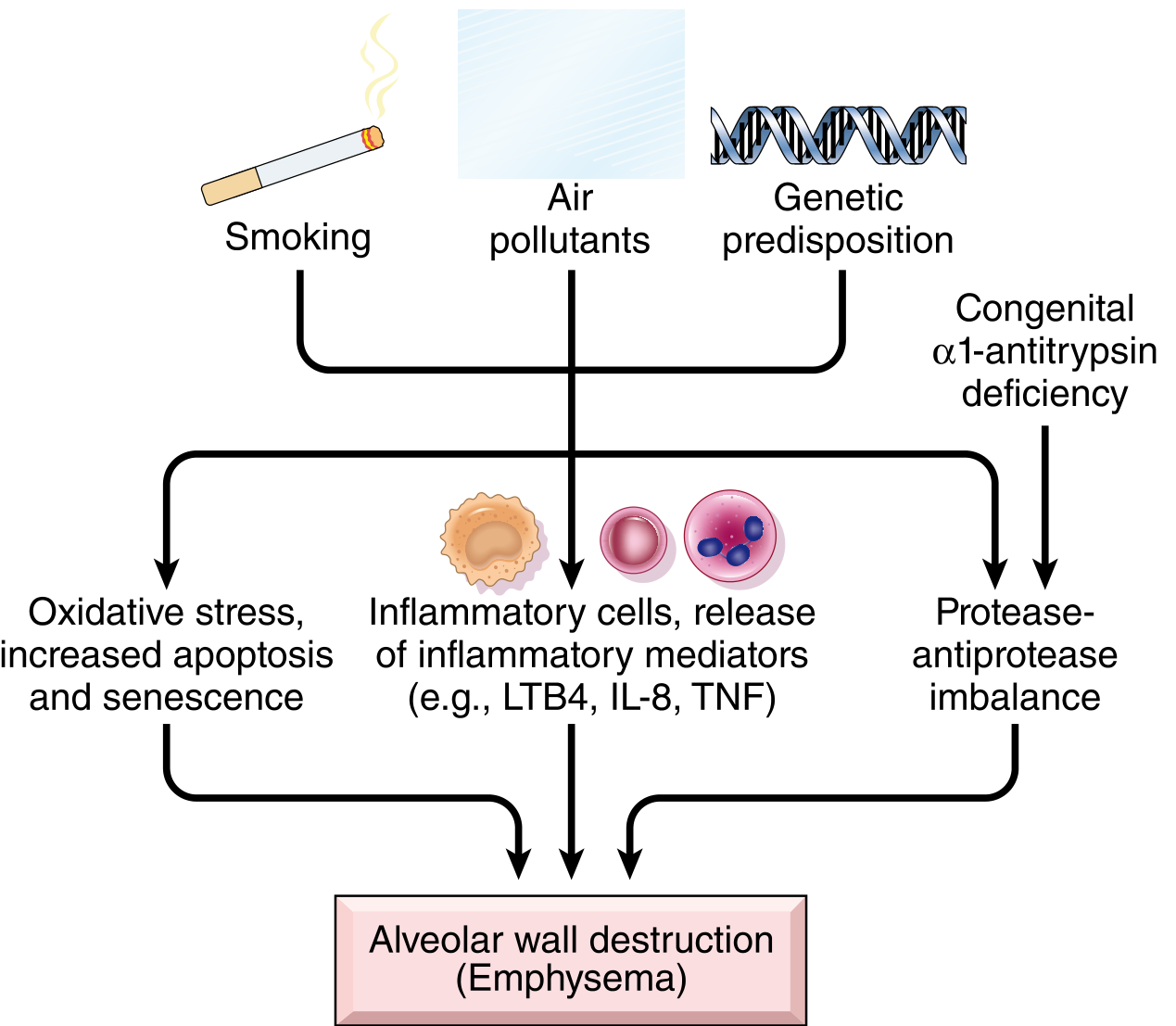
Fig. 15.8 - Pathogenesis of emphysema - Robbins, Cotran & Kumar
Key Mechanisms:
1. Toxic Injury and Inflammation
- Inhaled smoke damages respiratory epithelium → chronic inflammation
- Mediators elevated: LTB4, IL-8, TNF
- Neutrophils, macrophages, CD4+ and CD8+ T cells accumulate
- Chemotactic factors attract more inflammatory cells; proinflammatory cytokines amplify damage
2. Protease-Antiprotease Imbalance (central mechanism)
- Inflammatory and epithelial cells release proteases that break down connective tissue
- Key enzyme: elastase (from neutrophils) degrades elastin
- In emphysema, there is a relative deficiency of antiproteases (e.g., α1-AT)
- Loss of elastic tissue in alveolar walls → airways collapse on expiration → functional airflow obstruction
- Small airways lose radial traction from surrounding elastic tissue → collapse during expiration
3. Oxidative Stress
- Tobacco smoke contains reactive oxygen species (ROS); macrophages/neutrophils release more
- NRF2 (encoded by NFE2L2) is a sensor transcription factor - upregulates cytoprotective genes in alveolar cells
- Mice without NRF2 are hypersensitive to tobacco smoke; genetic NRF2 variants are associated with COPD in humans
- Oxidants cause tissue damage, endothelial dysfunction, and amplify inflammation
4. Infection
- Not an initiating factor, but bacterial/viral infections acutely exacerbate existing disease
α1-Antitrypsin Deficiency
- α1-AT is the major inhibitor of elastase secreted by neutrophils
- Encoded by the Proteinase Inhibitor (Pi) locus on chromosome 14
- Homozygous ZZ allele → very low serum levels (~0.012% of U.S. population)
-
80% of ZZ individuals develop symptomatic panacinar emphysema
- Occurs at earlier age and with greater severity if the individual smokes
- About 1% of all emphysema patients have this defect
Morphology
Gross:
- Lungs are voluminous, pale, soft - may obscure the heart when the chest is opened
- Panacinar: entire lung pale and voluminous
- Centriacinar: localized destruction, upper lobes, surrounded by normal parenchyma
- Large airspaces (bullae) may form, especially in paraseptal type
Microscopic:
- Destruction of alveolar walls
- Reduction in pulmonary capillary bed
- In centriacinar: emphysematous spaces surrounded by normal tissue in same acinus
- Subtle but functionally important small airway fibrosis (distinct from chronic bronchitis) also contributes to airflow obstruction
Chest X-ray:
- Hyperinflation
- Low, flat diaphragm (arrow visible on CXR above)
- Normal or small heart size
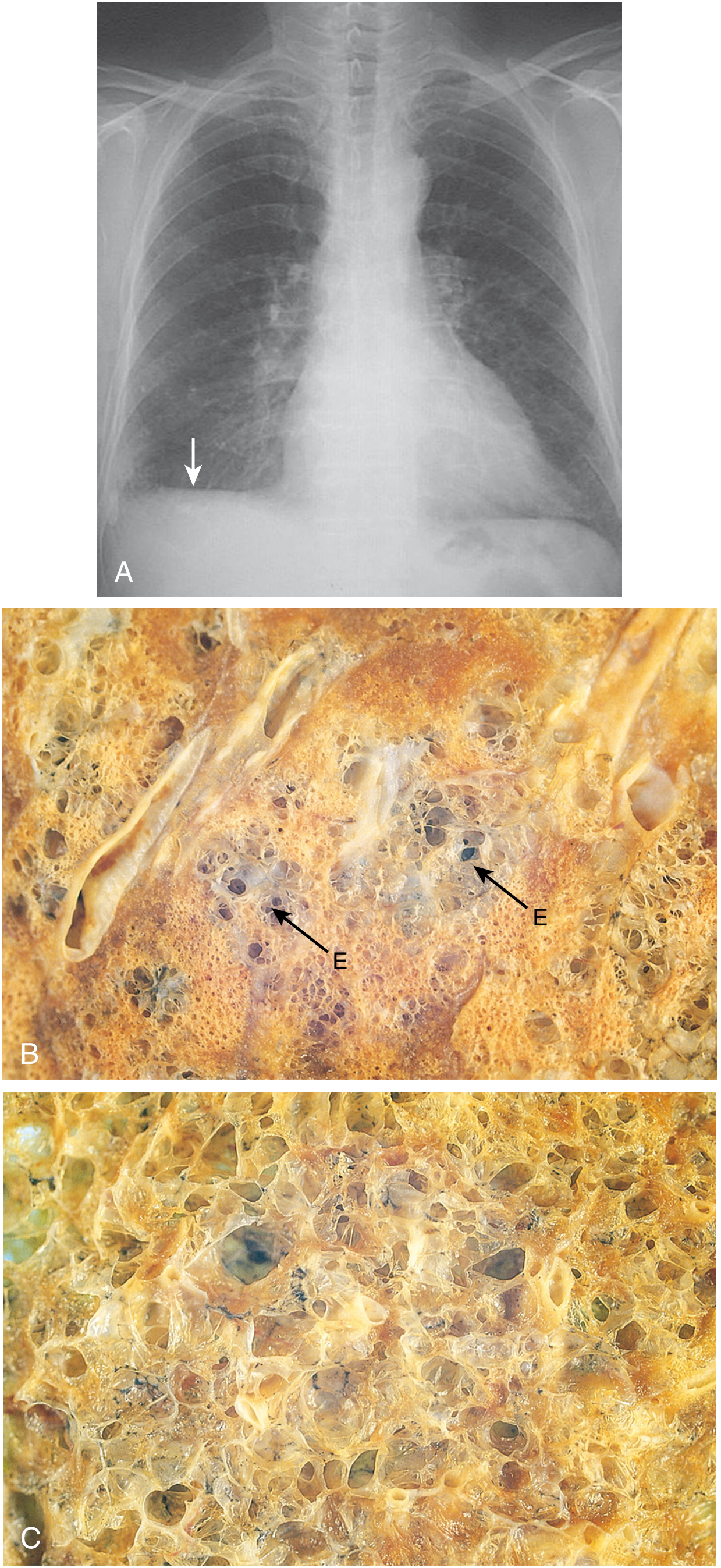
Fig. 15.7 - (A) CXR of advanced emphysema (B) Centriacinar emphysema with focal emphysematous destruction (E) (C) Panacinar emphysema with diffuse destruction - Robbins, Cotran & Kumar
Clinical Features
- History: usually >40 pack-years smoking
- Onset: insidious - slowly increasing dyspnea on exertion, chronic cough
- FEV1/FVC < 0.7 on spirometry (key diagnostic test)
"Pink Puffer" (Emphysema-dominant)
| Feature | Detail |
|---|---|
| Appearance | Well oxygenated, barrel-chested |
| Dyspnea | Severe, early |
| Cough | Late, scanty sputum |
| Breathing | Pursed lip breathing, hunched forward |
| Lung exam | Hyperinflation, prolonged expiration |
| Diffusion capacity | Low |
| Blood gases | Relatively normal at rest |
| Weight loss | Common, may suggest occult cancer |
| Cor pulmonale | Uncommon (end-stage) |
"Blue Bloater" (Chronic Bronchitis-dominant)
| Feature | Detail |
|---|---|
| Appearance | Cyanotic |
| Cough | Early, copious sputum |
| Dyspnea | Mild, late |
| Infections | Common |
| Respiratory insufficiency | Early, periodic |
| Cor pulmonale | Common |
Most patients fall somewhere in between with mixed features.
Comparison Table: Emphysema vs. Chronic Bronchitis
| Feature | Chronic Bronchitis | Emphysema |
|---|---|---|
| Age (years) | 40-45 | 50-75 |
| Dyspnea | Mild; late | Severe; early |
| Cough | Early; copious sputum | Late; scanty sputum |
| Infections | Common | Occasional |
| Respiratory insufficiency | Early, periodic | End-stage |
| Cor pulmonale | Common | Uncommon, end-stage |
| Airway resistance | Increased | Normal or slightly increased |
| Elastic recoil | Normal | Low |
| Chest radiograph | Prominent vessels; large heart | Hyperinflation; normal heart |
| Appearance | Cyanotic (blue bloater) | Well oxygenated (pink puffer) |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 15.4
Complications
- Pulmonary hypertension → cor pulmonale → right heart failure (especially with bronchitic component)
- Acute respiratory failure from superimposed infection
- Spontaneous pneumothorax from rupture of subpleural blebs (especially paraseptal type)
- Mucus plugging - associated with increased all-cause mortality in COPD
- Polycythemia from chronic hypoxia (especially bronchitic dominant)
Treatment
- Smoking cessation (most important)
- Long-acting bronchodilators (LABAs, LAMAs)
- Inhaled corticosteroids (in combination)
- Oxygen therapy (for hypoxemia)
- Antibiotics (for exacerbations)
- Physical/pulmonary rehabilitation
- Bullectomy (surgical resection of large bullae)
- Lung volume reduction surgery (selected patients - upper lobe predominant)
- Lung transplantation (selected patients)
- α1-AT replacement therapy (for deficiency)
Despite intervention, COPD often progresses and is frequently fatal. Prevention of smoking remains the most effective strategy.
Key Concepts Summary
- Emphysema = irreversible airspace enlargement + alveolar wall destruction, without significant fibrosis
- Most common in smokers (>40 pack-years); centriacinar type predominates
- α1-AT deficiency → panacinar type, earlier onset, lower lobes
- Central mechanism: protease-antiprotease imbalance with elastin destruction
- Loss of elastic recoil → airway collapse during expiration → obstructive physiology
- "Pink puffer" = emphysema dominant; "Blue bloater" = bronchitis dominant
- Serious complications: cor pulmonale, pneumothorax, respiratory failure
- Robbins & Kumar Basic Pathology, p. 448; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 635-636
Can you make quiz on this topic
Here's a 15-question quiz on emphysema, covering all the major concepts from the notes:
Emphysema Quiz
Q1. Which of the following is the correct definition of emphysema?
- A) Reversible narrowing of airways with mucus hypersecretion
- B) Permanent enlargement of airspaces distal to terminal bronchioles with alveolar wall destruction and significant fibrosis
- C) Permanent enlargement of airspaces distal to terminal bronchioles with alveolar wall destruction but without significant fibrosis
- D) Inflammation of bronchioles with goblet cell hyperplasia
Answer
C - Emphysema is defined as permanent, irreversible enlargement of airspaces distal to the terminal bronchiole with destruction of alveolar walls, but crucially WITHOUT significant fibrosis. Fibrosis would point to a restrictive, not obstructive, pattern.
Q2. A 30-year-old non-smoker presents with spontaneous pneumothorax. Which type of emphysema is the most likely underlying cause?
- A) Centriacinar
- B) Panacinar
- C) Distal acinar (paraseptal)
- D) Irregular (paracicatricial)
Answer
C - Distal (paraseptal) emphysema preferentially affects the subpleural airspaces and forms bullae. Rupture of these bullae is the classic cause of spontaneous pneumothorax in young adults.
Q3. A 58-year-old man with a 45 pack-year smoking history has emphysema. Which distribution pattern would you expect on imaging?
- A) Lower lobes, uniform acinar involvement
- B) Upper lobes, central/proximal acinar involvement with spared distal alveoli
- C) Adjacent to pleura with bulla formation
- D) Irregular involvement associated with old scars
Answer
B - Centriacinar (centrilobular) emphysema, the most common form associated with heavy smoking, preferentially affects the upper lobes. The central/proximal acinus (respiratory bronchioles) is destroyed while distal alveoli are spared - a key distinguishing feature.
Q4. α1-Antitrypsin deficiency is most strongly associated with which type of emphysema?
- A) Centriacinar, upper lobe predominant
- B) Distal acinar with bullae
- C) Panacinar, lower lobe predominant
- D) Irregular emphysema
Answer
C - α1-AT deficiency causes panacinar emphysema with uniform enlargement of the entire acinus. It is most severe at the lung bases (lower lobes), in contrast to smoking-related centriacinar emphysema which is upper lobe predominant.
Q5. α1-Antitrypsin is encoded by which locus, and what chromosome is it on?
- A) HLA locus, chromosome 6
- B) Proteinase Inhibitor (Pi) locus, chromosome 14
- C) Pi locus, chromosome 7
- D) CFTR locus, chromosome 7
Answer
B - α1-AT is encoded by the Proteinase Inhibitor (Pi) locus on chromosome 14. The ZZ homozygous genotype results in very low serum levels and is the highest risk genotype for developing emphysema.
Q6. In the protease-antiprotease hypothesis of emphysema, which enzyme is primarily responsible for alveolar wall destruction?
- A) Collagenase released by fibroblasts
- B) Elastase secreted by neutrophils
- C) Trypsin secreted by macrophages
- D) Matrix metalloprotease from bronchial epithelium
Answer
B - Neutrophil elastase is the primary culprit. It degrades elastin in alveolar walls. α1-Antitrypsin normally inhibits this enzyme, and when it is deficient (genetically or due to smoking-related oxidative inactivation), unchecked elastase activity destroys the parenchyma.
Q7. What is the functional consequence of losing elastic tissue in alveolar walls surrounding respiratory bronchioles?
- A) Increased mucus secretion
- B) Increased diffusion capacity
- C) Airway collapse during expiration (functional airflow obstruction)
- D) Increased radial traction and hyperventilation
Answer
C - Small airways are normally held open by elastic recoil (radial traction) from surrounding alveolar walls. When this elastin is destroyed, the airways lose this support and collapse during expiration, producing functional airflow obstruction even without any mechanical blockage of the lumen.
Q8. Which of the following inflammatory mediators is NOT typically elevated in emphysema?
- A) Leukotriene B4 (LTB4)
- B) IL-8
- C) TNF
- D) IL-10
Answer
D - LTB4, IL-8, and TNF are all pro-inflammatory mediators elevated in emphysematous lung tissue. IL-10 is an anti-inflammatory cytokine and is not listed among the key mediators elevated in emphysema pathogenesis.
Q9. A patient with emphysema sits forward in a hunched position, breathes through pursed lips, has a barrel chest, and is well oxygenated at rest. His cough is mild with scanty sputum. Which term describes this clinical picture?
- A) Blue bloater
- B) Pink puffer
- C) Mixed COPD
- D) Cardiac asthma
Answer
B - This is the classic "pink puffer" - emphysema dominant COPD. The pursed-lip breathing maintains positive end-expiratory pressure to splint open collapsing airways. These patients maintain relatively normal blood gases by working hard to breathe.
Q10. Which spirometric finding is the key diagnostic criterion for COPD/emphysema?
- A) FEV1/FVC > 0.8
- B) FVC < 70% predicted
- C) FEV1/FVC < 0.7
- D) Peak expiratory flow < 300 L/min
Answer
C - An FEV1/FVC ratio of less than 0.7 (post-bronchodilator) defines obstructive airflow limitation and is the key spirometric diagnostic criterion for COPD, which includes emphysema.
Q11. What percentage of emphysema patients have α1-antitrypsin deficiency as the underlying cause?
- A) 10%
- B) 5%
- C) ~1%
- D) ~25%
Answer
C - About 1% of all patients with emphysema have α1-AT deficiency as the primary cause. Despite being rare as a cause of emphysema overall, it is an important condition because it presents earlier in life and is dramatically worsened by smoking.
Q12. The transcription factor NRF2 (encoded by NFE2L2) plays a protective role in emphysema by:
- A) Inhibiting neutrophil elastase directly
- B) Upregulating genes that protect cells from oxidant damage
- C) Suppressing TNF and IL-8 production
- D) Increasing mucus secretion to trap pollutants
Answer
B - NRF2 is an oxidant-sensing transcription factor in alveolar epithelial cells. When activated by intracellular oxidants, it upregulates cytoprotective antioxidant genes. Mice lacking NRF2 are hypersensitive to tobacco smoke, and NRF2 pathway genetic variants are associated with COPD in humans.
Q13. Which complication of emphysema is most directly related to the bronchitic component of COPD?
- A) Spontaneous pneumothorax
- B) Pulmonary hypertension and cor pulmonale
- C) Reduced diffusion capacity
- D) Weight loss mimicking malignancy
Answer
B - Long-standing COPD, particularly with a significant bronchitic component (hypoxemia, hypercapnia), commonly leads to pulmonary vasoconstriction, pulmonary hypertension, and ultimately cor pulmonale (right heart failure). Spontaneous pneumothorax is more linked to the emphysematous (paraseptal) component.
Q14. Which surgical option specifically targets destruction of large air-trapping spaces that compress adjacent viable lung tissue?
- A) Lobectomy
- B) Pleurodesis
- C) Bullectomy
- D) Pneumonectomy
Answer
C - Bullectomy involves surgical resection of large bullae (giant air-filled spaces). Removing these non-functioning, space-occupying bullae can decompress adjacent viable lung tissue and improve overall pulmonary function.
Q15. Which type of emphysema is almost always associated with scarring and is usually clinically insignificant?
- A) Centriacinar
- B) Panacinar
- C) Distal acinar
- D) Irregular (paracicatricial)
Answer
D - Irregular (paracicatricial) emphysema is named for its irregular acinar involvement. It is almost invariably associated with pre-existing scarring and typically occurs in small foci that do not produce significant airflow obstruction.
Score Guide
| Score | Result |
|---|---|
| 13-15 | Excellent - solid command of emphysema |
| 10-12 | Good - review pathogenesis mechanisms |
| 7-9 | Fair - revisit types, clinical features, and α1-AT |
| <7 | Go back to the notes and try again |
This is a shared conversation. Sign in to Orris to start your own chat.