Methanol toxicity,Blunt abdominal trauma according to emergency book medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer from ROSEN's and Tintinalli's Emergency Medicine. Here is the full response:
Methanol Toxicity
Sources: ROSEN's Emergency Medicine (9th ed.) and Tintinalli's Emergency Medicine (9th ed.)
Pharmacology / Sources
Methanol (methyl alcohol, "wood alcohol") is a clear, colorless, slightly sweet liquid. Common sources include:
- Windshield washer fluid, antifreeze, paint removers, cleaning solutions, embalming fluid
- Camp stove fuel, industrial solvents, adhesives, enamels
It is rapidly absorbed from the GI tract (absorptive half-life ~5 minutes, peak concentration at 30-60 minutes). Significant toxicity can also occur via inhalation and transdermal routes in occupational settings (painting, varnishing, lithography).
Metabolism and Mechanism of Toxicity
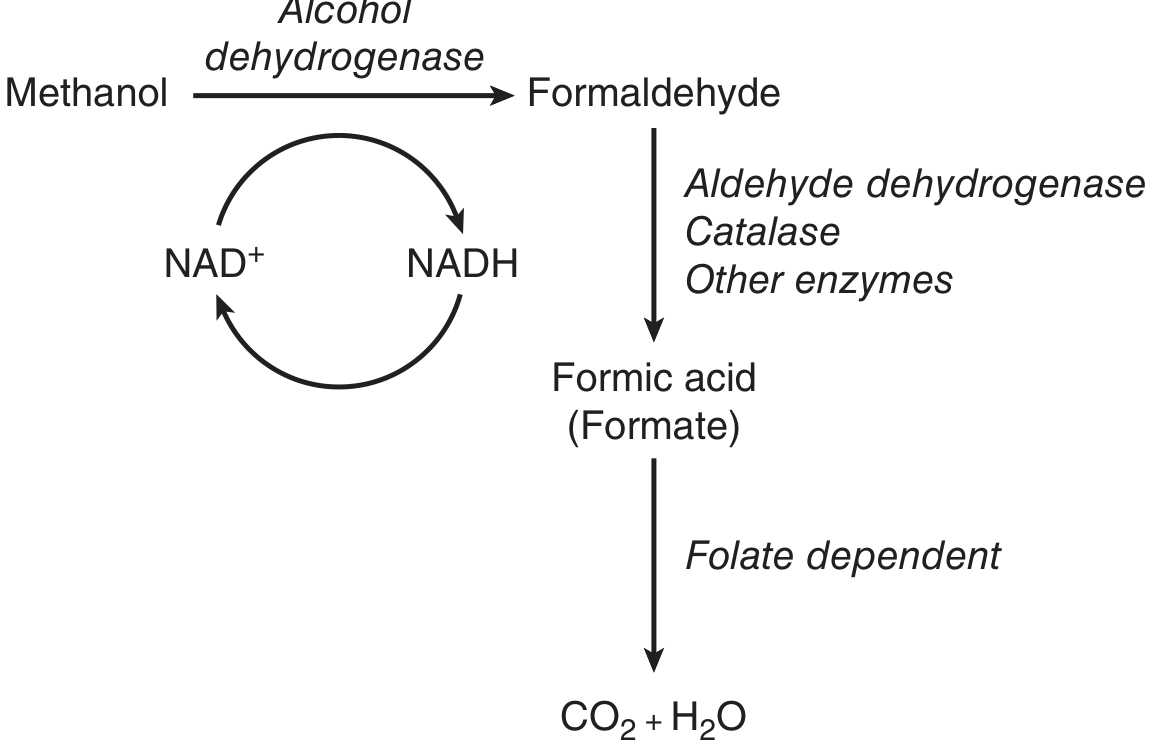
Fig. Metabolism of methanol - ROSEN's Emergency Medicine
Methanol itself is only mildly toxic. The toxicity is entirely due to its metabolites:
- Methanol → (alcohol dehydrogenase / ADH) → Formaldehyde (half-life 1-2 min)
- Formaldehyde → (aldehyde dehydrogenase / ALDH) → Formic acid (formate)
- Formic acid → (folate-dependent pathway / THF synthetase) → CO₂ + H₂O
Formic acid is the key toxic metabolite. Its mechanisms of harm:
- Binds cytochrome oxidase and blocks oxidative phosphorylation → anaerobic metabolism → lactic acidosis
- Increases NADH/NAD+ ratio → favors pyruvate → lactate conversion (worsens lactic acidosis)
- At lower pH, more formic acid exists in undissociated form, crossing tissue barriers more readily → greater CNS and ocular toxicity
- Acidosis also increases tubular reabsorption of formic acid, prolonging its elimination
Kinetics: At toxic concentrations, metabolism follows zero-order kinetics; blood methanol falls at ~8.5 mg/dL/hour. With ADH inhibition, the half-life of methanol extends to >50 hours.
Latency: Symptoms may be delayed 12-24 hours because metabolite formation (not methanol itself) drives toxicity. If ethanol is co-ingested, onset is further delayed as ethanol competes for ADH.
Clinical Features
| System | Features |
|---|---|
| CNS | Headache, vertigo, dizziness, seizures, coma; bilateral putamen necrosis on CT |
| Ocular | Photophobia, blurred or "snow field" vision, papilledema, non-reactive mydriasis (indicates permanent damage), nystagmus (rare) |
| GI | Abdominal pain, nausea, vomiting, gastritis, pancreatitis; transaminitis (mild/transient) |
| Cardiovascular | Tachycardia, hypotension, shock in severe cases |
| Respiratory | Tachypnea (compensating for metabolic acidosis) → may progress to respiratory failure |
| Renal | Rhabdomyolysis, renal failure (severe cases) |
Key prognostic markers: Coma + seizures + severe metabolic acidosis on presentation = poor outcome. The severity of poisoning correlates more with the degree of acidosis than with the methanol level itself.
Diagnosis / Labs
- Anion-gap metabolic acidosis with elevated formate
- Elevated osmolar gap (measured osmolality - calculated osmolality > 10 mOsm/L) - seen early before metabolite formation
- Serum methanol level (send immediately; results may be delayed)
- ABG: low pH, low bicarbonate
- Serum lactate (elevated due to formate's blockade of oxidative phosphorylation)
- Non-contrast head CT before anticoagulation: may show putamen necrosis, subcortical white matter damage, intracranial hemorrhage
Important: An osmolar gap can be normal late in poisoning (after parent alcohol is largely metabolized to formate), while anion gap acidosis is maximal. Both gaps should be considered together.
Management
1. Supportive Care
- ABC management; intubation if needed for airway protection
- IV fluids, cardiac monitoring
- Sodium bicarbonate for severe acidosis (pH <7.0-7.1): helps prevent formic acid from crossing into tissues
2. ADH Blockade (Metabolic Blockade) - Fomepizole (First-line)
Indications for initiating ADH blockade (Box 136.1, ROSEN's):
- Documented plasma methanol ≥ 20 mg/dL, OR
- History of ingestion + osmolar gap > 10 mOsm/L, OR
- Strong clinical suspicion + at least 2 of: pH < 7.3 | HCO₃ < 20 mEq/L | osmolar gap > 10 mOsm/L
Do not wait for confirmatory levels if clinical suspicion is high - treat empirically.
Fomepizole dosing (Box 136.2, ROSEN's):
- Loading dose: 15 mg/kg IV
- Maintenance: 10 mg/kg IV every 12 hours (for up to 48 h)
- After 48 h: 15 mg/kg every 12 h (auto-induction of CYP450 metabolism)
- During hemodialysis: same doses but every 4 hours (fomepizole is dialyzed out)
- Continue until methanol < 20 mg/dL (< 6 mmol/L) AND metabolic acidosis resolved
Side effects: headache, nausea, dizziness, phlebitis, transient transaminase elevation. No absolute contraindications (except known allergy - none reported).
Ethanol as alternative (if fomepizole unavailable):
- Maintain serum ethanol 100-150 mg/dL; ADH has 10x greater affinity for ethanol than methanol
- Oral protocol (80-proof liquor): loading 1.5-2 mL/kg, maintenance 0.2-0.5 mL/kg/hr
- Double maintenance dose during dialysis
- Risk: CNS/respiratory depression, hypoglycemia (especially in children/malnourished), complex dosing
3. Hemodialysis (HD)
Indications (ROSEN's):
- pH < 7.3
- Visual abnormalities
- Renal failure
- Electrolyte imbalances unresponsive to therapy (e.g., hyperkalemia)
- Hemodynamic instability
- Methanol concentration > 50 mg/dL
HD removes both parent methanol and formate, corrects acidosis, and shortens hospital course (important given methanol's 50+ hour half-life with ADH blockade). Intermittent HD is preferred over continuous renal replacement therapy (CRRT) but CRRT is acceptable if HD unavailable.
4. Folinic Acid (Leucovorin)
- Aids formic acid elimination via THF synthetase pathway
- Dose: 1 mg/kg IV (max 50 mg) every 4-6 hours until methanol is eliminated and acidosis resolves
- No human trial proof of efficacy, but use does not delay or replace HD when indicated
5. Disposition
- Admit for all patients being treated
- Early nephrology consult for HD
- Ophthalmology consult within 24 hours to evaluate retina and visual fields
- Transfer to HD-capable facility if not available locally
- Contact regional poison center (USA: 1-800-222-1222) or medical toxicologist
- Discharge only if methanol < 20 mg/dL with no symptoms or lab abnormalities
Blunt Abdominal Trauma (BAT)
Sources: ROSEN's Emergency Medicine and Tintinalli's Emergency Medicine
Epidemiology and Mechanisms
The most common cause of BAT is motor vehicle collision (MVC). Falls are second in frequency. Pedestrians struck by vehicles, motorcyclists, and bicyclists are at especially high risk. Forces involved: compression, shearing/stretching, and acceleration/deceleration.
Most commonly injured organs:
- Spleen - most common; isolated injury in ~two-thirds of cases
- Liver - second most common
- Hollow viscus (small bowel) - uncommon but important (CT is less sensitive for these injuries)
Clinical Features
Signs range from subtle to severe shock. Diagnosis is challenging because:
- Concomitant injuries (especially head trauma) may mask or distract from abdominal findings
- Intoxication or altered mental status limits examination reliability
- Young, healthy patients may compensate for significant hemorrhage before vital sign changes appear
- Elderly patients on beta-blockers or anticoagulants may blunt physiologic response
Key signs:
- Abdominal tenderness, guarding, rigidity, rebound (signs of peritoneal irritation)
- Seatbelt sign (lap belt contusion): intra-abdominal injury in ~1/3 of cases
- Gray-Turner sign (flank ecchymosis): retroperitoneal hemorrhage (can be delayed 12 h to days)
- Cullen sign (periumbilical ecchymosis): retroperitoneal hemorrhage (delayed)
- Distension: from hemoperitoneum, pneumoperitoneum, gastric dilation, or ileus
- Unexplained hypotension after significant blunt trauma = intraperitoneal hemorrhage until proven otherwise
As many as 45% of blunt trauma patients thought to have a benign abdomen on initial exam are later found to have significant intra-abdominal injury (Tintinalli's).
Diagnostic Approach
Primary Survey and e-FAST
The extended FAST (e-FAST) is performed at the transition from primary to secondary survey in all patients. It detects free intraperitoneal fluid (hemoperitoneum) and is at least as sensitive and specific as portable chest X-ray for hemothorax/pneumothorax.
Unstable patient + positive e-FAST (hemoperitoneum) → immediate laparotomy.
Laboratory Tests
- CBC: leukocytosis 12,000-20,000/mm³ can result from demargination (non-specific)
- Metabolic acidosis: base deficit ≥ 6, lactate > 4 mmol/L, or decreasing bicarbonate suggest perfusion compromise
- LFTs: elevated transaminases suggest hepatic injury (does not distinguish contusion from severe injury)
- Amylase/lipase: NOT useful acutely - normal values do not exclude pancreatic injury, and elevated values are non-specific
Radiology
- Portable chest X-ray (or e-FAST chest component): screen for hemothorax/pneumothorax before CT transfer
- Plain abdominal films: not indicated in blunt trauma (except projectile localization)
- Pelvic X-ray: may be omitted in hemodynamically stable patients heading directly to CT
- CT abdomen/pelvis (with contrast): gold standard for the hemodynamically stable patient - identifies organ injuries, active hemorrhage (blush), retroperitoneal injury
CT limitations: Less sensitive for hollow viscus injury, diaphragmatic injuries, and some pancreatic injuries. Free fluid without a clear solid organ source warrants high suspicion for bowel injury.
Management Algorithm
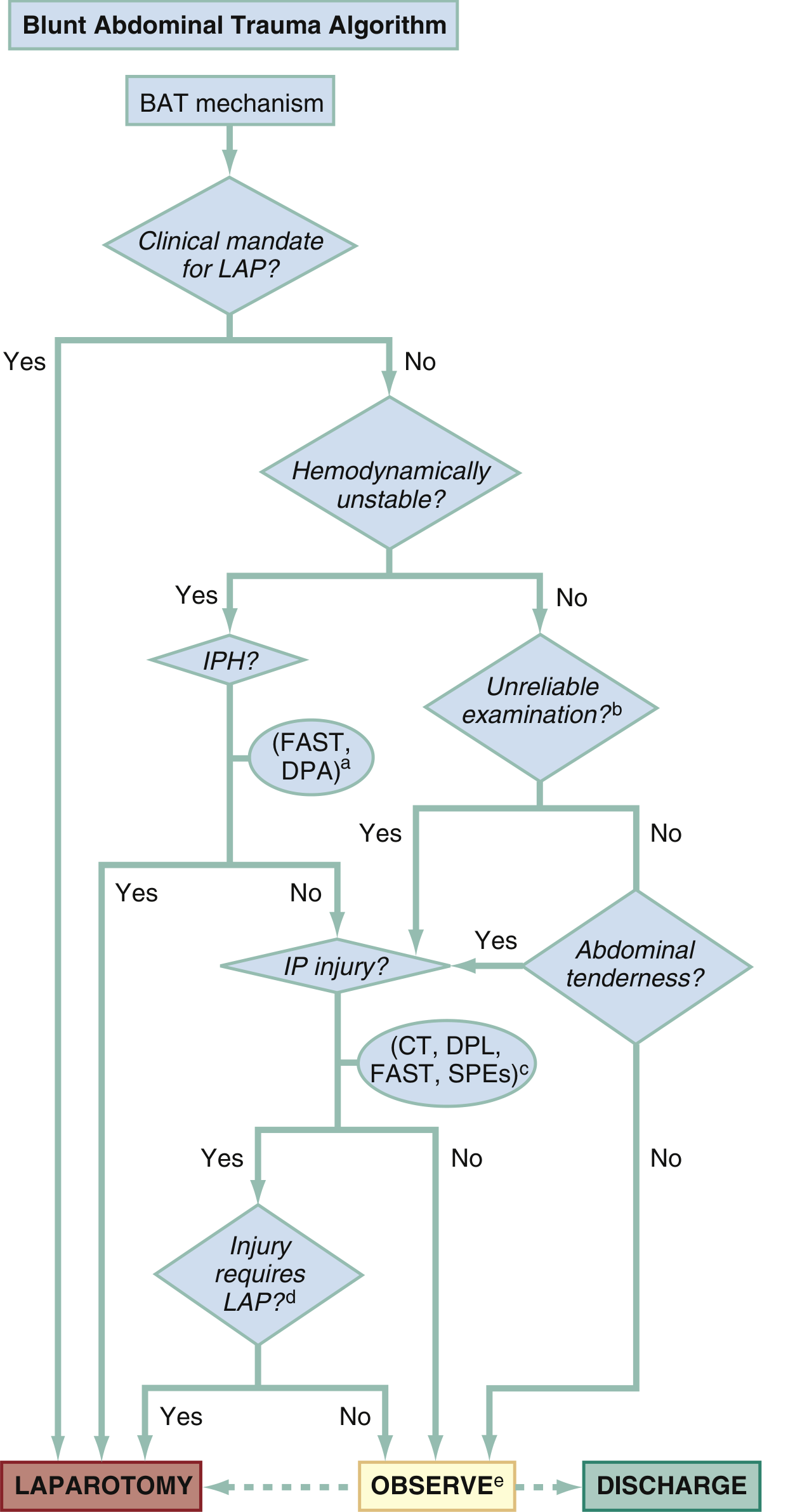
Fig. 38.8 Blunt Abdominal Trauma (BAT) Algorithm - ROSEN's Emergency Medicine
Indications for Immediate Laparotomy (Blunt Trauma):
Absolute:
- Anterior abdominal injury with hypotension
- Abdominal wall disruption
- Peritonitis
- Free air under diaphragm on chest X-ray
- Positive FAST or DPL in hemodynamically unstable patient
- CT-diagnosed injury requiring surgery
Relative:
- Positive FAST or DPL in hemodynamically stable patient
- Solid visceral injury in stable patient
- Hemoperitoneum on CT without clear source
Nonoperative Management
In hemodynamically stable patients, nonoperative management of blunt liver and spleen injuries has a 95% success rate - provided the institution has:
- Trauma surgeons immediately available
- Adequate blood bank resources
- Radiologists capable of emergent angioembolization
- Rapid transfer capability to OR
Critical caveat: Hollow viscus injury (bowel, bladder) requires operative management when present. It is easily missed on CT.
Special Considerations
- Tranexamic acid: Consider in all patients with traumatic abdominal hemorrhage. Based on CRASH-2 trial: most benefit within 1 hour; administration beyond 3 hours increases risk of death. Should be available in all EDs managing trauma.
- Anticoagulation reversal: Warfarin or factor Xa inhibitors (rivaroxaban, apixaban, edoxaban): prothrombin complex concentrate (PCC). Dabigatran: idarucizumab.
- Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA): Available at Level 1 trauma centers for unresponsive shock from intra-abdominal hemorrhage; acts as endovascular aortic clamp.
- Angioembolization: Advancing nonoperative option for vascular injuries; transcatheter coil or Gelfoam embolization to arrest hemorrhage.
Disposition
- Significant intra-abdominal injury: admit to surgical/trauma service
- Consider admission even for minor abdominal injury if concomitant injuries present
- Discharge patients: thorough return precautions (fever, vomiting, increased pain, dizziness, weakness)
References: ROSEN's Emergency Medicine - Concepts and Clinical Practice, 9th ed. (Ch. 38, 136); Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed. (Ch. 185, 263)
This is a shared conversation. Sign in to Orris to start your own chat.