Give me details about abdominal TB
Reading File
Finding Sources
Finding Sources
Searching PubMed
"abdominal tuberculosis" diagnosis treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from Harrison's, Murray & Nadel, Bailey & Love, and S Das. I have enough to compile a detailed, well-organized answer. Let me now present the full response.
Abdominal Tuberculosis
Abdominal TB refers to tuberculosis affecting any organ within the abdomen, including the gastrointestinal tract, peritoneum, mesenteric lymph nodes, and solid organs (liver, spleen, pancreas). It accounts for approximately 11% of extrapulmonary TB cases and is the sixth most common site of extrapulmonary involvement globally.
Aetiology and Epidemiology
- Causative organism: Mycobacterium tuberculosis (human type predominates); M. bovis (bovine type) is linked to unpasteurized dairy consumption
- Common in resource-limited countries; incidence is rising in developed nations due to migration and immunosuppression
- HIV co-infection is a major risk factor; M. avium intracellulare becomes increasingly prevalent in HIV-positive patients
- M. bovis and M. fortuitum can also cause intestinal TB via unpasteurized dairy and present similarly
Routes of Infection
| Route | Mechanism |
|---|---|
| Ingestion of infected sputum | Patient with active pulmonary TB swallows bacilli-laden sputum |
| Ingestion of infected milk | Drinking unpasteurized milk (bovine type) - colonises Peyer's patches of terminal ileum |
| Haematogenous | Spread from miliary TB or other primary foci |
| Direct extension | Spread from adjacent structures (e.g., Fallopian tubes in genital TB, mediastinal lymph nodes) |
| Lymphatic spread | Via mesenteric lymph nodes |
Classification
Abdominal TB is broadly divided into:
1. Intestinal Tuberculosis
2. Tuberculosis of Mesenteric Lymph Nodes
3. Tuberculous Peritonitis
4. Solid Organ TB (liver, spleen, pancreas - less common)
1. Intestinal Tuberculosis
The terminal ileum and caecum (ileocaecal region) are involved in the vast majority of cases, owing to the abundance of lymphoid follicles (Peyer's patches). Lesions proximal to the terminal ileum are unusual.
Pathological Types
(a) Ulcerative Type
- Results from swallowing sputum in active pulmonary TB
- Organism colonises the lymphatics of the terminal ileum
- Produces transverse ulcers with characteristic undermined edges
- Serosa studded with tubercles
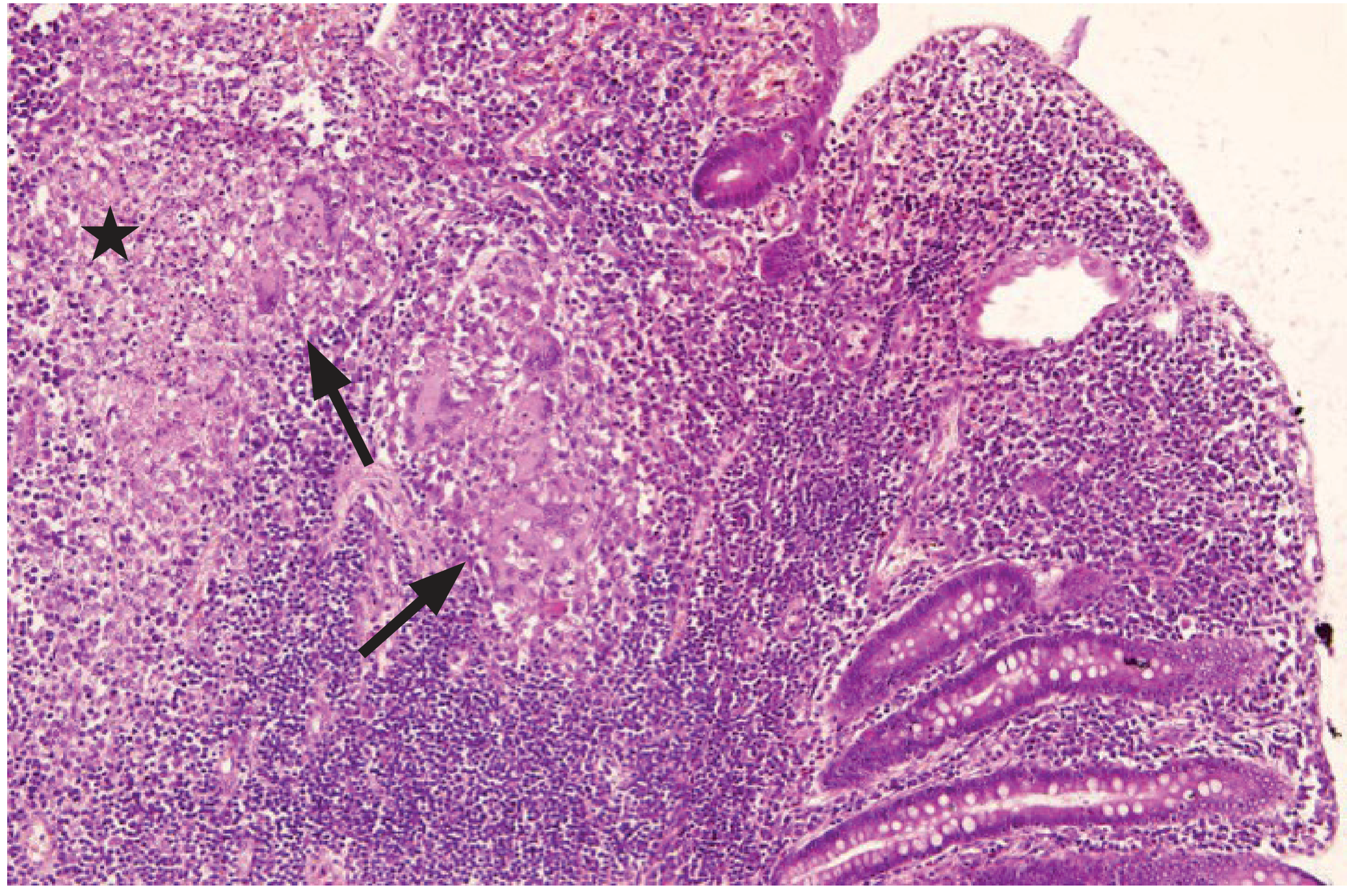
- Histology: caseating granuloma with Langhans' giant cells (see histology image below)
- Healing leads to fibrosis and multiple strictures - a major cause of intestinal obstruction
- Perforation is unusual because the serous coat over the ulcer becomes thickened
(b) Hyperplastic (Hypertrophic) Type
- Occurs when host resistance overcomes organism virulence
- Marked inflammatory reaction causes hyperplasia and thickening of the terminal ileum and caecum
- Fibrosis leads to shortening of bowel with the caecum pulled up into a subhepatic position, widening the ileocaecal angle beyond 90°
- Macroscopically may resemble Crohn's disease
- Presents as a right iliac fossa mass with features of subacute obstruction
Both types may coexist with marked mesenteric lymphadenopathy
Clinical Features
Symptoms
- Abdominal pain (most common) - cramping, worse after meals; right iliac fossa or central
- Weight loss and anorexia
- Diarrhoea (with or without blood/mucus) or alternating bowel habits
- Fever - classically low-grade, evening rise
- Nausea; change in bowel habits
- Night sweats, malaise
Signs
- Palpable right iliac fossa mass in hyperplastic type (may mimic carcinoma or Crohn's)
- Tenderness in the right iliac fossa
- Ascites and abdominal distension (in peritonitis)
- Features of intestinal obstruction (distension, high-pitched bowel sounds)
Differential Diagnoses
- Crohn's disease (most important - very similar clinically and radiologically)
- Carcinoma of the caecum/colon
- Appendicitis / appendix mass
- Amoebic colitis
- Yersinia ileitis
- Lymphoma
2. Tuberculosis of Mesenteric Lymph Nodes
- Mainly seen in children
- Bacilli enter lymph nodes through Peyer's patches of the terminal ileum
- Bovine and human types both implicated
Presentations:
- Chronic abdominal pain - central dull discomfort; enlarged nodes palpable right of umbilicus as firm, discrete, round nodules
- General symptoms only - weight loss, anorexia, pallor, low-grade fever
- Intestinal obstruction - adherence of small bowel to a caseating node
- Mimics appendicitis - pain and tenderness in the RIF; distinguished by persistent nature, negative Rovsing's sign, no high pulse/leucocytosis
- Pseudomesenteric cyst - caseation with cold abscess forming between mesenteric leaves
3. Tuberculous Peritonitis
The peritoneum is involved in 50-80% of patients with abdominal TB.
Pathogenesis: Spread from ruptured lymph nodes, GI tract (typically ileocaecal region), or haematogenous seeding; in women, direct spread from infected Fallopian tubes is common.
Types
| Type | Features |
|---|---|
| Wet (ascitic) type (90%) | Generalised or loculated ascites; multiple tubercle deposits on both peritoneal layers |
| Dry (plastic/fibrotic) type | Fibrotic loops of bowel and omentum matted together; subacute intestinal obstruction; NO ascites |
| Mixed type | Combined features |
Clinical Features
- Insidious onset: abdominal pain, distension, weight loss, fever, night sweats
- Ascites
- Coexistence with cirrhosis can obscure diagnosis
- Distinction from diffuse peritoneal metastases is often difficult and requires biopsy
CT Findings in TB Peritonitis
The axial CT below shows lymphadenopathy with mesenteric involvement and ascites, typical of abdominal TB:

Investigations
Laboratory
- Raised inflammatory markers (ESR, CRP)
- Anaemia (normochromic normocytic)
- Positive sputum AFB smear/culture (if concurrent pulmonary TB)
- Interferon-gamma release assays (IGRA) - useful for subclinical infection detection
- Mantoux/tuberculin skin test - may be positive
Ascitic Fluid Analysis (TB Peritonitis)
- Straw-coloured exudate (protein >25-30 g/L)
- White cells >500/mL with lymphocyte predominance (>40%)
- Adenosine deaminase (ADA) - high sensitivity (93%) and specificity (96%) for TB peritonitis
- AFB smear: low sensitivity (rarely positive)
- Culture: positive in only ~50% but increases with large volume submission (takes 4-8 weeks)
Imaging
- Chest X-ray: pulmonary infiltrates or miliary pattern in ~50%
- Abdominal USS: loculated ascites, lymphadenopathy, bowel wall thickening
- CT abdomen: bowel wall thickening, lymphadenopathy with central necrosis (hallmark distinguishing from IBD), peritoneal thickening, omental caking, ascites
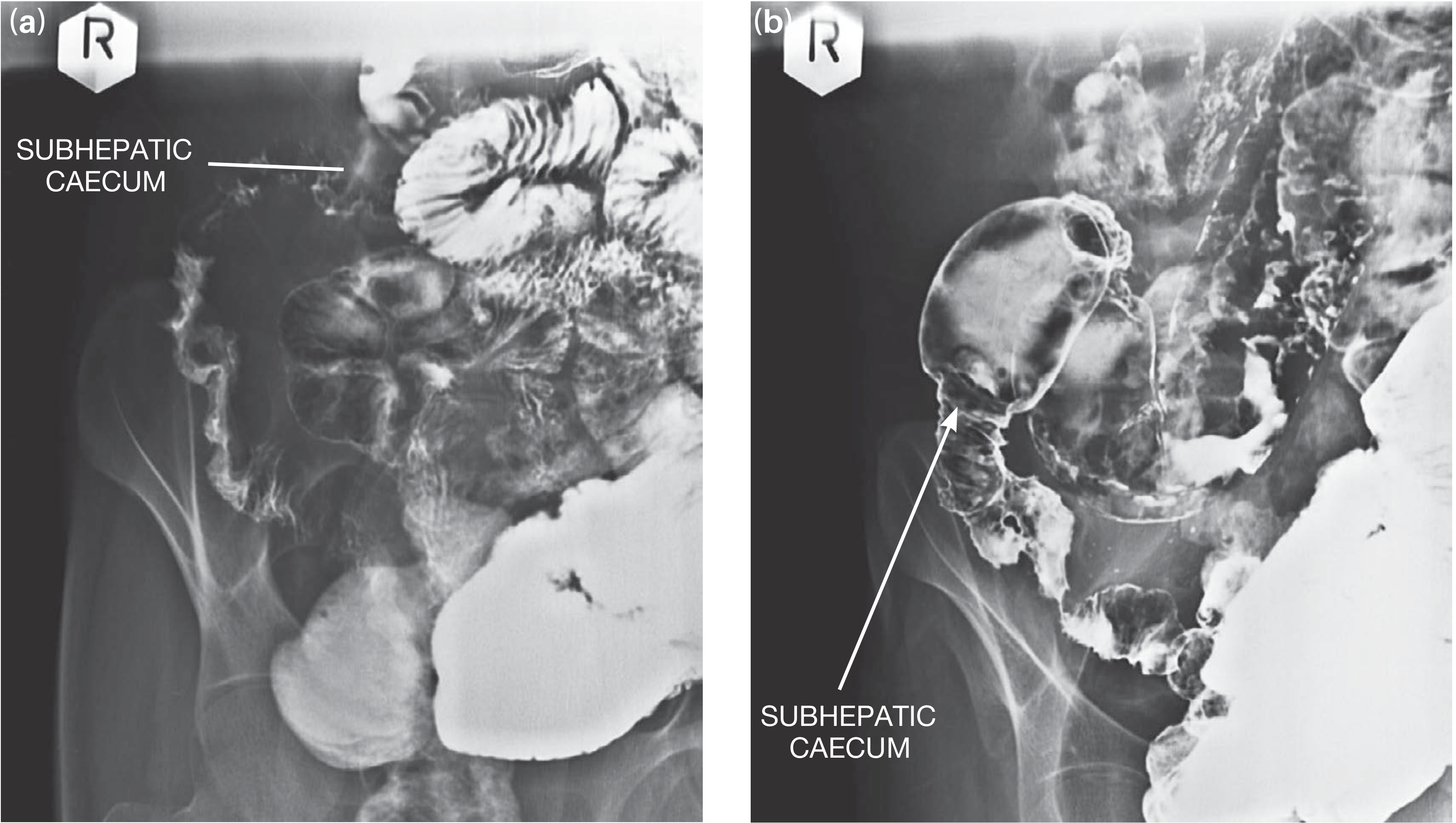
- Barium meal and follow-through: multiple small bowel strictures; subhepatic caecum (caecum pulled up due to fibrosis); non-filling or inadequate filling of terminal ileum and caecum ("Stierlin's sign" area)
The barium studies below demonstrate strictures in the ileum with the caecum pulled into a subhepatic position:
Endoscopy
- Colonoscopy is particularly valuable: visualizes lesions and allows biopsy
- Findings pointing to TB: terminal ileitis with ulceration, pseudodiverticulosis, stricture mucosa
- Histopathology provides diagnosis in 40-55% of specimens; culture yield 20-50%
- Xpert MTB/RIF assay on tissue samples: sensitivity up to 80%; preferred initial diagnostic option
Laparoscopy
- Gold standard when other investigations fail
- Allows direct visualization of characteristic appearances (peritoneal tubercles) and peritoneal biopsy
- Couples typical visual appearance with histopathological confirmation
Treatment
Medical (First-Line Anti-TB Chemotherapy)
Standard multidrug regimen following WHO/national guidelines:
- Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) - 2HRZE
- Continuation phase (4 months): Isoniazid + Rifampicin - 4HR
- Total duration: 6 months for uncomplicated cases; some centres extend to 9 months for abdominal TB
- Note: Multidrug resistance (MDR-TB) may be higher for abdominal than pulmonary TB; DST should guide therapy
- Supportive care: nutritional rehabilitation and hydration are essential components
Surgical Management
Elective surgery is indicated when medical treatment fails or for significant residual strictures:
| Indication | Procedure |
|---|---|
| Single ileal stricture | Strictureplasty |
| Limited ileocolic hyperplastic disease | Ileocolic resection with anastomosis |
| Multiple closely-spaced strictures | Bowel resection |
| Extensive ileocolic disease | Right hemicolectomy |
Emergency surgery (obstruction, perforation, haemorrhage):
- Patient often severely ill: dehydrate, malnourished, anaemic, possibly with active pulmonary TB
- Vigorous resuscitation first
- Minimum life-saving procedure: resection of diseased segment + proximal ileostomy + distal mucus fistula (avoids high-risk anastomosis in presence of active infection)
- One-stage resection and anastomosis only if general condition permits
Surgical principles mirror those in Crohn's disease - keep resections as conservative as possible. Post-operatively, complete the full course of anti-TB chemotherapy (6-12 months).
Key Distinguishing Features: TB vs Crohn's Disease
| Feature | Intestinal TB | Crohn's Disease |
|---|---|---|
| Geography | Endemic areas | Developed countries |
| Perianal disease | Rare | Common (80%) |
| Subhepatic caecum | Present | Absent |
| Granulomas | Caseating | Non-caseating |
| Lymph node necrosis on CT | Yes | No |
| Response to anti-TB therapy | Yes | No |
| ADA in ascites | Elevated | Normal |
| Skin/joint/eye involvement | Less common | Erythema nodosum, synovitis, iritis |
Complications
- Intestinal obstruction (most common)
- Intestinal perforation (less common due to serosal thickening, but occurs)
- Fistula formation (entero-enteric, entero-cutaneous)
- Malabsorption
- Haemorrhage
- Mesenteric cyst formation
- Constrictive peritonitis
Recent Evidence
A 2025 systematic review (PMID 40533676) on abdominal TB in children highlights ongoing challenges in diagnosis and management, emphasizing that the condition remains under-recognized and that surgical intervention is frequently required in the paediatric population.
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1110-1112 & pp. 109-111
- Harrison's Principles of Internal Medicine, 22nd Ed., pp. 1431-1432
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1422-1432
- S Das: A Manual on Clinical Surgery, 13th Ed., pp. 517-518
Abdominal tb in pediatrics
Finding Sources
Searching PubMed
"abdominal tuberculosis" children pediatric
Reading Article
PMID: 40533676
Reading Article
PMID: 40963962
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"abdominal tuberculosis" children diagnosis
Reading Article
PMID: 36211645
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
abdominal tuberculosis children pediatric diagnosis treatment guidelines 2024 2025
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12446891
Finding Sources
I now have comprehensive data from multiple sources. Let me compile the full pediatric-focused response.
Abdominal Tuberculosis in Pediatrics
Abdominal TB in children is an important but underdiagnosed condition, classified as extrapulmonary TB (EPTB). It is described as an "enigma" in the literature because of its non-specific symptoms that overlap with many other childhood conditions, making it a major cause of diagnostic delay. A 2025 systematic review (Raj & Sharma) covering 807 pediatric cases across 51 studies highlighted this challenge, concluding that it "needs to be differentiated from other conditions" due to vague presentations.
Epidemiology and Risk Factors
- Predominant age group: adolescents are most commonly affected; however, cases have been reported from neonates (congenital TB) to young adults
- Female preponderance noted in large case series
- Highest burden in TB-endemic regions (South Asia, sub-Saharan Africa)
- Key risk factors in children:
- Close household contact with an adult with active pulmonary TB (most important source of exposure)
- HIV co-infection (dramatically increases susceptibility)
- Malnutrition and poverty
- Unpasteurized milk consumption (bovine-type TB, M. bovis)
- Absence of BCG vaccination
Pathogenesis - How it Differs in Children
Children acquire TB differently from adults in several important ways:
| Feature | Children | Adults |
|---|---|---|
| Primary infection | More common - often no prior TB exposure | Usually reactivation |
| Route of GI involvement | Haematogenous spread from primary focus more prominent | Swallowed sputum predominates |
| Bovine type (M. bovis) | More significant (milk ingestion) | Less common |
| Mesenteric LN involvement | Primary form of abdominal TB in children | Secondary to gut involvement |
| Miliary spread | More common, especially in infants | Less common |
| Concurrent pulmonary TB | Only reported in ~6 studies; often subclinical | More commonly identified |
In children, Peyer's patches in the terminal ileum are the primary gateway - bacilli penetrate here and colonise the draining mesenteric lymph nodes, making mesenteric lymphadenitis the most characteristic form of abdominal TB in pediatrics.
Classification (Same as Adults - with Different Frequency)
- Mesenteric lymph node TB - most common form in children
- Intestinal TB (ulcerative or hyperplastic)
- Tuberculous peritonitis
- Solid organ TB (hepatic, splenic, pancreatic) - rare but reported
Clinical Presentation
Symptoms (Most Common to Less Common)
- Fever (low-grade, evening rise) - most frequent complaint
- Abdominal pain - can be acute, subacute, or chronic; central or right iliac fossa
- Abdominal distension - often from ascites or matted loops
- Weight loss / failure to thrive - chronic cases
- Anorexia
- Constipation or diarrhea (alternating or one predominant)
- Vomiting
- Ascites
From the AIIMS prospective study (2025, PMID 40978883), abdominal TB was found to be "a common cause of acute abdomen in the pediatric population" - it should be actively considered whenever a child in an endemic region presents with abdominal pain, fever, and weight loss.
Unusual/Atypical Presentations Reported in Children
- Splenic microabscess (especially in HIV-positive cases)
- Liver abscess (HIV co-infection)
- Deep vein thrombosis (hypercoagulable state from TB inflammation)
- Mesenteric artery stenosis
- Intracranial sinus thrombosis
- Neonatal/congenital abdominal TB (rare - from haematogenous spread in utero)
Why Children are Frequently Misdiagnosed
A 2025 systematic review and meta-analysis (Siddiqui et al., PMID 40963962) identified key reasons for misdiagnosis in 60 pediatric ATB cases:
- No single clinical feature reliably predicts ATB - clinical features alone are insufficient for diagnosis
- Ascites and abdominal distension were more common in misdiagnosed children (confused with nephrotic syndrome, cirrhosis, malignancy)
- The symptoms overlap significantly with:
- Appendicitis / appendix mass
- Malignancy (lymphoma, neuroblastoma)
- Inflammatory bowel disease
- Nephrotic syndrome
- Acute mesenteric adenitis
- Amoebic liver abscess
- Typhoid abdomen
The study concluded: "Clinical characteristics alone are not reliable indicators for diagnosing ATB... early suspicion and timely diagnostic evaluation in TB-endemic regions is crucial."
Investigations
Microbiological
- Mycobacterial culture: 50-75% positivity in pediatric series (higher than in adults due to tissue sampling)
- CB-NAAT / Xpert MTB/RIF: increasing use in children; preferred initial test; sensitivity ~80%
- AFB smear: low sensitivity
- Gastric aspirate: used when sputum cannot be obtained (particularly in infants and young children) for concurrent pulmonary TB detection
Immunological
- Mantoux test (TST): supportive but not diagnostic; may be negative in severely malnourished/immunocompromised children
- Interferon-gamma release assays (IGRA): better specificity than TST; useful for subclinical TB infection; preferred in BCG-vaccinated children
- Adenosine Deaminase (ADA) in ascitic fluid or tissue: An authoritative meta-analysis (Zhou et al., 2022, PMID 36211645) demonstrated pooled sensitivity 93% and specificity 95% for abdominal TB diagnosis - ADA is an excellent diagnostic biomarker
Blood Tests
- Raised inflammatory markers: elevated ESR, CRP
- Anaemia (normochromic normocytic) - very common in children
- Leucocytosis (mild, non-specific)
- Low albumin in chronic cases
- Lymphopenia in severe disease
Imaging
Chest X-Ray
- Look for pulmonary infiltrates, miliary pattern, pleural effusion, mediastinal lymphadenopathy
- Abnormal in up to 50% - even when child has no pulmonary symptoms
Abdominal Ultrasound (first-line in children)
- Mesenteric lymphadenopathy
- Free or loculated ascites
- Bowel wall thickening
- Omental thickening
- Hepatosplenic involvement (granulomas appear as small hypoechoic foci)
CT Abdomen (gold standard imaging)
- Lymphadenopathy with central necrosis - highly specific for TB vs. other causes
- Bowel wall thickening (especially terminal ileum and caecum)
- Peritoneal thickening and enhancement
- Omental caking - seen in peritoneal TB
- Ascites (free or loculated)
- Calcified lymph nodes in healed/old mesenteric TB (also visible on plain X-ray)
Barium Studies
- Multiple small bowel strictures
- Subhepatic caecum (caecum pulled superiorly by fibrosis)
- Incomplete filling or hypermotility of terminal ileum ("Stierlin's sign")
- Less commonly used now; CT/MRI preferred
MRI
- Preferred in children to avoid radiation
- Excellent for soft tissue delineation and peritoneal disease
Endoscopy/Laparoscopy
- Colonoscopy with biopsy - visualises ileocaecal lesions; histopathology diagnostic in 40-55%
- Laparoscopy: gold standard for peritoneal TB; allows direct visualization + biopsy; typical appearance of small white peritoneal tubercles
- All attempts for tissue diagnosis (imaging-guided biopsy, endoscopic, laparoscopic, surgical) should be made
Definite vs. Probable Abdominal TB (Diagnostic Categories)
| Category | Criteria |
|---|---|
| Definite | Positive mycobacterial culture OR positive CB-NAAT OR typical histology (caseating granuloma with AFB) |
| Probable | Clinical + imaging + TST/IGRA consistent with TB, with response to anti-TB therapy |
In children, many cases are treated as probable TB because confirming culture or histology is not always feasible.
Treatment
Medical Management (First-Line)
The WHO-recommended 6-month regimen (2HRZE / 4HR) is standard for drug-susceptible abdominal TB in children:
| Phase | Duration | Drugs | Pediatric Dosing (WHO 2025) |
|---|---|---|---|
| Intensive | 2 months | HRZE | See below |
| Continuation | 4 months | HR | See below |
2025 WHO / South African Guideline Dosing for Children (<15 years):
| Drug | Dose | Maximum |
|---|---|---|
| Isoniazid (H) | 10 mg/kg/day (range 10-15 mg/kg) | 300 mg/day |
| Rifampicin (R) | 15 mg/kg/day (range 10-20 mg/kg) | 600 mg/day |
| Pyrazinamide (Z) | 35 mg/kg/day (range 30-40 mg/kg) | 2 g/day |
| Ethambutol (E) | 20 mg/kg/day (range 15-25 mg/kg) | 1 g/day |
CNS/miliary TB (if coexistent): uses 6-9 month single-phase treatment with higher-dose Isoniazid (15-20 mg/kg) and ethionamide instead of ethambutol, per 2024 South African pediatric guidelines.
Special considerations in children:
- Fixed-dose combination (FDC) tablets are preferred for ease of administration and adherence
- Pyridoxine (vitamin B6) supplementation is recommended with isoniazid in children to prevent peripheral neuropathy
- Regular LFT monitoring (hepatotoxicity risk with H, R, Z)
- Nutritional rehabilitation is a critical component of management - malnutrition worsens prognosis and impairs drug metabolism
- Duration may be extended to 9 months for extensive or complicated abdominal TB
HIV Co-Infected Children
- Start anti-TB therapy first; initiate ART within 2-8 weeks
- Drug interactions between rifampicin and antiretrovirals require careful management (rifampicin reduces lopinavir/ritonavir levels significantly)
- Higher doses of some drugs may be needed
- MDR-TB must be actively excluded
Surgical Management
Main indications for surgery in children:
| Indication | Procedure |
|---|---|
| Intestinal perforation (most common surgical indication) | Resection + primary anastomosis if stable, or diversion |
| Intestinal obstruction | Strictureplasty / limited resection |
| Diagnostic uncertainty | Laparoscopic biopsy |
| Residual strictures post-medical treatment | Resection or strictureplasty |
| Mesenteric cyst (cold abscess) | Drainage/excision |
Key surgical principles in children:
- Medical management is always tried first; obstruction may resolve with anti-TB therapy alone
- Emergency cases: severely ill children (dehydrated, anaemic, malnourished) need vigorous resuscitation before operating
- Preferred emergency approach: limited resection + proximal ileostomy + distal mucus fistula (avoids high-risk anastomosis in the presence of active infection and poor general condition)
- Anastomosis may be performed at a second-stage operation once the child has recovered
- Post-operatively, complete the full anti-TB course (6-12 months) under combined pediatric medicine and surgical care
Complications
- Intestinal obstruction (most common)
- Intestinal perforation
- Fistula formation
- Malabsorption and growth failure
- Mesenteric cyst formation
- Constrictive peritonitis
- Adhesive obstruction post-surgery
- DVT / vascular complications (rare)
- Disseminated/miliary TB
- Drug-induced liver injury (from ATT)
Prognosis
- Good prognosis with early diagnosis and prompt initiation of ATT
- Delayed diagnosis significantly worsens outcomes - complications (perforation, obstruction) increase mortality
- Children in endemic regions with non-specific symptoms require a high index of suspicion
- The AIIMS 2025 study emphasizes: "early detection through recognition of common clinical features, guided imaging, and timely sampling for confirmation is vital for initiating ATT and improving outcomes"
Summary: Key Pediatric-Specific Points
- Mesenteric lymph node TB is the most characteristic form in children (rare in adults)
- Haematogenous spread and primary TB are more prominent pathways in children
- Fever + abdominal pain + weight loss in a child from an endemic area = suspect TB until proven otherwise
- No single clinical feature reliably distinguishes ATB from other abdominal conditions - early suspicion and multi-modal workup are essential
- ADA (pooled sensitivity 93%, specificity 95%) is an excellent biomarker
- Intestinal perforation is the primary indication for surgery in children (cf. obstruction in adults)
- Nutritional rehabilitation is as important as ATT
- 6-month HRZE/HR regimen is standard; weight-based dosing is mandatory in children
- Unusual presentations (splenic abscess, DVT, neonatal TB) must be recognized
- BCG vaccination provides significant protection against disseminated and extrapulmonary TB in children
Sources:
- Raj V, Sharma S. Abdominal tuberculosis in children: a systematic review on current advances. Pediatr Surg Int, 2025. [PMID 40533676]
- Siddiqui MJ et al. Clinical characteristics leading to misdiagnosis of abdominal TB in children. Front Pediatr, 2025. [PMID 40963962]
- Zhou R et al. Diagnostic performance of ADA for abdominal TB: meta-analysis. Front Public Health, 2022. [PMID 36211645]
- S Das: A Manual on Clinical Surgery, 13th Ed., p. 517
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 109-111
- WHO/South African National Guideline: Management of TB in Children and Adolescents, 2024-2025
This is a shared conversation. Sign in to Orris to start your own chat.