Histology and variants of penile carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"penile carcinoma" AND "histological variants"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Histology and Variants of Penile Carcinoma
Overview
Penile carcinoma is predominantly a squamous cell carcinoma (SCC), accounting for the vast majority of penile malignancies. Other rare tumors include melanoma, basal cell carcinoma, sarcoma, and Paget disease, but SCC and its variants are the clinical focus.
Macroscopically, penile SCCs appear as:
- Irregular, fungating cauliflower-like masses
- Flat, indurated lesions
- Large verruciform/papillary tumors
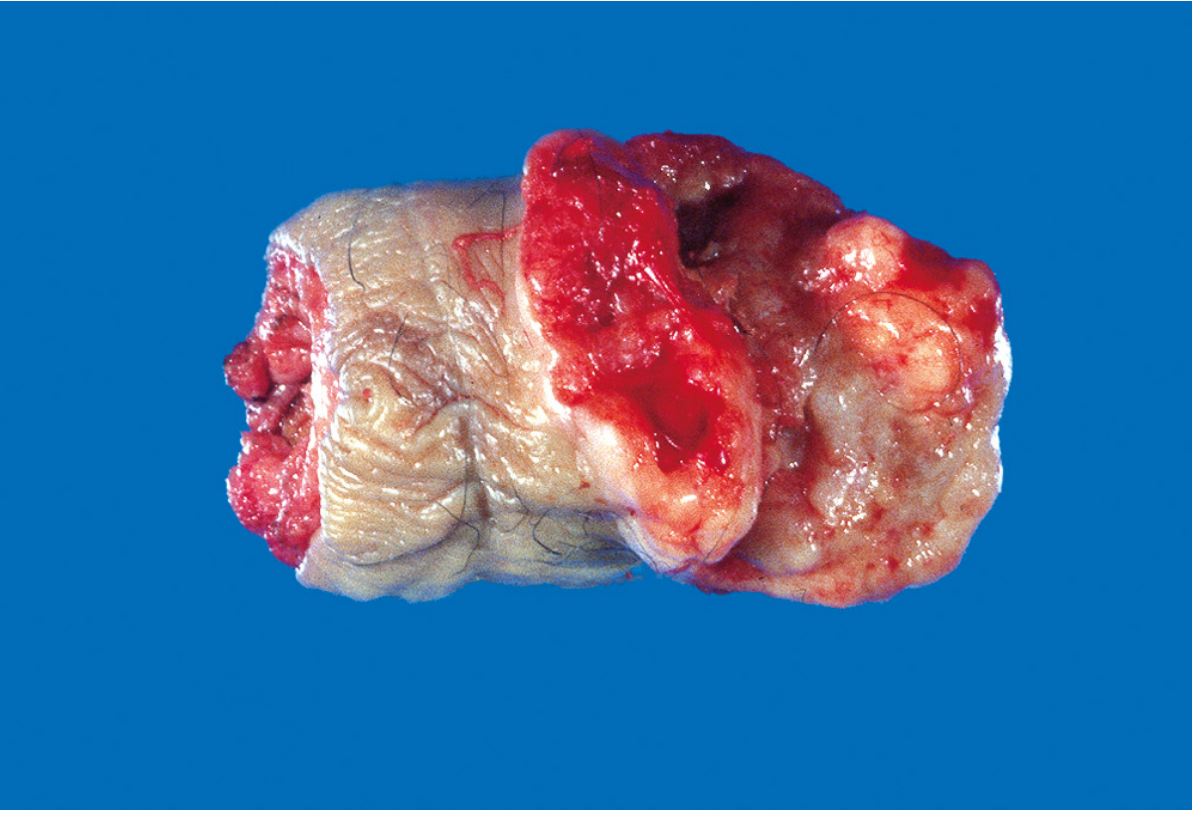
Gross specimen: the glans penis is deformed by a firm, ulcerated, infiltrative mass. (Robbins & Cotran Pathologic Basis of Disease)
General Histologic Features (Usual SCC)
Most penile SCCs demonstrate:
- Keratinization
- Epithelial pearl formation
- Various degrees of mitotic activity
- Disruption of normal rete pegs
- Penetration of the basement membrane with invasion into surrounding structures (corpus spongiosum, corpora cavernosa)
WHO 2022 Classification: HPV-Based Framework
The World Health Organization 2022 classification divides penile SCC into HPV-independent and HPV-associated categories. This system, subsequently adopted by major urologic societies, allows recognition of HPV-associated subtypes not only by p16 immunostaining but also by their histologic features.
HPV-Independent Squamous Cell Carcinomas
| Subtype | Key Features | Grade / Behavior |
|---|---|---|
| Usual type (conventional SCC) | Most common; ~47-59% of cases; cords of atypical squamous cells with keratinization, intercellular bridges, keratin pearls | Intermediate (Grades 1-3); 36% disease-specific mortality |
| Verrucous carcinoma | Exophytic, warty, highly differentiated; invades along a broad pushing border; HPV-independent | Well-differentiated (Grade 1); rarely metastasizes |
| Carcinoma cuniculatum | Subtype of verrucous; deeply burrowing (tunnel-like) growth pattern | Well-differentiated; low metastatic potential |
| Papillary squamous cell carcinoma | Exophytic papillary fronds; keratinizing; not verrucous | Well-differentiated (Grade 1); low metastatic risk |
| Sarcomatoid (spindle cell) carcinoma | Biphasic: SCC component + spindle cell/mesenchymal component; highly pleomorphic | Poorly differentiated (Grade 3); aggressive |
| Pseudoglandular / adenosquamous | Rare; gland-like spaces within SCC | Variable |
HPV-Associated Squamous Cell Carcinomas
| Subtype | Key Features | Grade / Behavior |
|---|---|---|
| Basaloid carcinoma | Small, hyperchromatic, uniform cells with scant cytoplasm and minimal squamous differentiation; ~10% of penile SCC; destructive invasion | Poorly differentiated (Grade 3); HPV+ in ~80%; aggressive (63% mortality in one series) |
| Warty (condylomatous) carcinoma | Exophytic with papillary condyloma-like architecture; koilocytosis present; ~10% of cases | Moderate differentiation; intermediate prognosis |
| Warty-basaloid carcinoma | Mixed features of warty and basaloid; combined HPV-driven pathway | Intermediate-high grade |
| Clear cell squamous carcinoma | Cells with abundant clear glycogen-rich cytoplasm | Intermediate |
| Lymphoepithelial carcinoma | Undifferentiated cells with prominent lymphocytic infiltrate (similar to nasopharyngeal carcinoma) | Variable |
| Papillary basaloid carcinoma | Papillary architecture + basaloid cytology | High grade |
Other/Rare Variants
- Adenosquamous carcinoma - mixed glandular and squamous elements
- Mucoepidermoid carcinoma - mixed mucus-secreting and squamous cells
- Extramammary Paget disease - intraepithelial adenocarcinoma with Paget cells (large vacuolated cells); often underlying adenocarcinoma
Histologic Grading (Broders System)
Grading uses the Broders classification, typically adapted to a 3-grade system:
| Grade | Features | Frequency |
|---|---|---|
| Grade 1 (well-differentiated) | Abundant keratinization, keratin pearls, prominent intercellular bridges, minimal nuclear pleomorphism | ~70-80% of cases at diagnosis |
| Grade 2 (moderately differentiated) | Intermediate features | |
| Grade 3/4 (poorly differentiated) | Loss of keratinization, high nuclear pleomorphism, many mitoses; absent keratin pearls | ~20-30%; associated with shaft tumors |
- Low-grade lesions constitute 70-80% of cases at diagnosis
- Tumors of the shaft are ~50% poorly differentiated
- Tumors of the prepuce are only ~10% poorly differentiated
- High grade strongly correlates with regional nodal metastasis
Precursor / Pre-malignant Lesions (Penile Intraepithelial Neoplasia - PeIN)
All three entities below are forms of carcinoma in situ and share similar histology (full-thickness dysplasia without basement membrane invasion):
| Entity | Location | Histology | Risk |
|---|---|---|---|
| Erythroplasia of Queyrat (EQ) | Glans/prepuce; red velvety plaque | Atypical hyperplastic cells; vacuolation; hyperchromatic nuclei; plasma cell-rich submucosa; rete elongation | 10-33% risk of progression to invasive carcinoma |
| Bowen Disease (BD) | Penile shaft; scaly erythematous plaque | Identical CIS changes; full-thickness dysplasia | ~5% risk of invasion |
| Bowenoid Papulosis (BP) | Shaft of young men; multiple pigmented papules | Histologically identical to CIS | Benign course; rarely progresses |
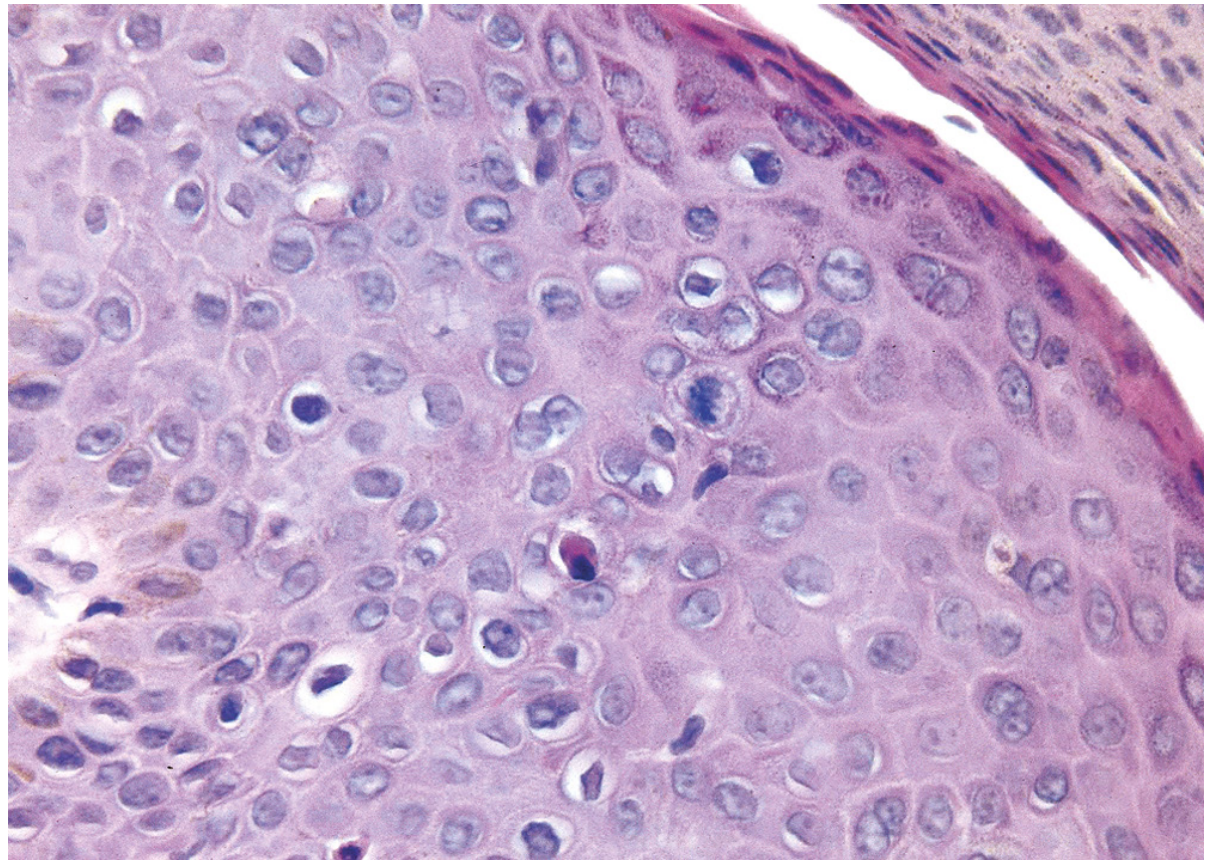
Bowen disease (carcinoma in situ) of the penis: hyperchromatic, dysplastic cells and scattered mitoses above the basal layer. (Robbins & Cotran Pathologic Basis of Disease)
HPV infection (predominantly high-risk types) is found in ~90% of penile dysplasia/CIS cases.
Pathogenesis: Two Molecular Pathways
HPV-associated pathway (~30-50% of penile SCC):
- High-risk HPV (types 16, 18) encodes E6 and E7 oncoproteins
- E6 inactivates p53 (promotes apoptosis resistance)
- E7 inactivates RB (promotes cell cycle progression)
- Results in genomic instability and proliferation
- Subtypes: basaloid, warty, warty-basaloid, clear cell, lymphoepithelioma-like
HPV-independent pathway (~50-70%):
- Chronic inflammation, phimosis, smegma accumulation, lichen sclerosus (balanitis xerotica obliterans), smoking
- Usual type SCC, verrucous carcinoma, papillary NOS, cuniculatum, sarcomatoid
- Molecular events not fully defined; not mediated by E6/E7
Prognostic Implications by Subtype
| Subtype | Nodal Metastasis Risk | Prognosis |
|---|---|---|
| Verrucous | Very low | Excellent; ~0% death |
| Papillary NOS | Low | Favorable |
| Usual type | Moderate | Intermediate; ~36% mortality |
| Warty | Moderate | Intermediate |
| Basaloid | High | Poor; ~63% mortality |
| Sarcomatoid | High | Poor |
Pathologic prognostic factors overall: stage, grade, histologic subtype, vascular invasion, perineural invasion.
Sources:
- Campbell Walsh Wein Urology, 3-Volume Set, pp. 2319-2331 (Histologic Features, Grading, PeIN)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 893-895 (Morphology, WHO 2022 Classification, Pathogenesis)
This is a shared conversation. Sign in to Orris to start your own chat.