Management of panic attack in emergency
"panic attack" AND "emergency department" AND management
"panic disorder" AND "emergency" AND treatment
Management of Panic Attack in the Emergency Department
1. Understanding the Presentation
| Symptom Category | Symptoms |
|---|---|
| Cardiorespiratory | Palpitations, chest pain/discomfort, shortness of breath, feeling smothered, choking |
| Autonomic | Sweating, trembling/shaking, chills or heat sensations |
| Neurological | Dizziness/lightheadedness, paresthesias, derealization/depersonalization |
| GI | Nausea or abdominal distress |
| Cognitive | Fear of losing control/"going crazy," fear of dying |
2. Initial Priority - Rule Out Life-Threatening Causes
| System | Conditions to Exclude |
|---|---|
| Cardiac | Myocardial infarction, unstable angina, dysrhythmias, mitral valve prolapse |
| Pulmonary | Pulmonary embolism, asthma exacerbation, hypoxia |
| Endocrine | Hypoglycemia, hyperthyroidism/thyroid storm, pheochromocytoma, hyperadrenocorticism, hypoparathyroidism |
| Neurologic | CVA, TIA |
| Substance-related | Stimulant intoxication (cocaine, amphetamines, caffeine), withdrawal from benzodiazepines, opiates, SSRIs/SNRIs, or alcohol |
| Medication-induced | Corticosteroids, bronchodilators, decongestants, neuroleptics |
~25% of patients presenting to the ED with chest pain ultimately have panic disorder as the diagnosis. However, the morbidity and mortality of cardiovascular disease demands appropriate cardiac evaluation whenever the distinction is unclear.
- Rosen's Emergency Medicine, Ch. 98; Tintinalli's Emergency Medicine, Ch. 289
- Onset of anxiety after age 35 with no psychiatric history
- No personal/family history of anxiety disorder
- Poor response to anxiolytics
- No avoidance behavior
- No identifiable psychosocial stressor
3. Assessment
- A useful screening question: "Have you experienced brief periods of overwhelming panic or terror accompanied by racing heart, shortness of breath, or dizziness?"
- Ask about prior panic attacks, psychiatric history, substance use, current stressors
- Medications - especially recent changes, stimulants, withdrawal history
- Always screen for suicidal and homicidal ideation - anxiety disorders carry a 10-fold greater suicide risk vs. the general population; risk escalates further with comorbid mood disorder
- ECG (rule out arrhythmia, ischemia)
- Blood glucose
- Pulse oximetry
- Thyroid function (TSH, free T4) if thyroid disorder is suspected
- Urine/serum toxicology if substance use is a concern
- D-dimer / CT pulmonary angiography if PE is on the differential
- Urinary catecholamines or plasma metanephrine if pheochromocytoma is suspected
4. Acute ED Management
Step 1: Non-Pharmacologic First-Line Measures
- Verbal de-escalation: calm, reassuring communication is the most important initial intervention
- Psychoeducation: reassure the patient they are not dying or "going crazy" - normalize the experience and explain that panic attacks are a treatable condition
- Breathing retraining: coach diaphragmatic, slow controlled breathing to interrupt the hyperventilation-anxiety cycle
- Remove triggers: quiet environment, reduce stimuli
- Supportive therapy: allow the patient to problem-solve with support
Note: Intentional hyperventilation can replicate a panic attack (distinguished from medical hyperventilation by its irregular, interrupted pattern). Teaching controlled breathing directly addresses this mechanism.
Step 2: Pharmacologic Therapy
| Drug | Dose | Notes |
|---|---|---|
| Lorazepam (Ativan) | 0.5-1.0 mg PO/IM/IV (up to 3x/day) | Most commonly used in ED; IM route convenient |
| Alprazolam (Xanax) | 0.25-1.0 mg PO (3-4x/day) | Rapid onset; higher dependence potential |
| Clonazepam (Klonopin) | 0.5-1.0 mg PO (twice daily) | Longer half-life |
| Diazepam (Valium) | 2-10 mg PO (2-4x/day) | Longer half-life; useful for bridging |
- Duration: prescribe for 1 week or less from the ED; avoid in long-term management
- Avoid in: history of alcohol/drug abuse, elderly patients (fall risk, paradoxical agitation, cognitive slowing, polypharmacy interactions), emotionally dependent patients
- Has rapid anxiolytic effect
- No dependence potential
- Particularly useful in patients with substance use history
5. Long-Term Pharmacotherapy (Initiate with PCP/Psychiatrist, not typically started in ED)
| Drug Class | Agent | Dose | Notes |
|---|---|---|---|
| SSRI | Sertraline | 25-200 mg/day (start 25 mg) | FDA approved: PD, PTSD, SAD, OCD |
| SSRI | Paroxetine | 10-70 mg/day (start 10-20 mg) | FDA approved: GAD, PD, PTSD, SAD, OCD |
| SSRI | Fluoxetine | 10-60 mg/day (start 10 mg) | FDA approved: PD, OCD |
| SNRI | Venlafaxine XR | 37.5-300 mg/day | FDA approved: GAD, PD, SAD; preferred formulation for anxiety |
| Buspirone | - | - | Works well for GAD; onset 1-3 weeks; no dependence potential; not effective for acute attacks |
- SSRIs/SNRIs take effect in several weeks; benzodiazepines may be prescribed to bridge until effect
- MAOIs and TCAs are effective but have been supplanted due to side effect profiles
6. Disposition
| Situation | Action |
|---|---|
| Medically cleared, first or recurrent attack, no suicidality | Discharge with close PCP or psychiatrist follow-up |
| Difficulty navigating outpatient system | Consider short stay in psychiatric observation or crisis stabilization unit |
| Suicidal or homicidal ideation | Urgent psychiatric consultation, hospitalization required |
| Comorbid severe depression | Urgent psychiatric attention |
| Underlying medical condition identified | Treat the primary cause |
- Connect the patient with a social worker or mental health worker if available (better outcomes than simply providing a referral list)
- Counsel on avoiding exacerbating factors: caffeine, alcohol, recreational stimulants
- Provide psychoeducation about cognitive-behavioral therapy (CBT) - evidence shows even a single session of CBT at ED discharge for noncardiac chest pain reduces panic symptoms within 2 weeks and may reduce ED return visits
- Medication changes or initiation of antidepressants should be coordinated with the primary care provider or psychiatrist, not started de novo in the ED without a follow-up plan
Summary Algorithm
Patient with acute panic symptoms
↓
Rule out life-threatening causes (MI, PE, arrhythmia, hypoglycemia, thyroid storm, pheochromocytoma, substance withdrawal)
↓
Screen for suicidality (10x elevated risk)
↓
Non-pharmacologic: de-escalation, psychoeducation, breathing retraining
↓
If inadequate: Benzodiazepine (lorazepam 0.5-1 mg) or hydroxyzine
↓
Disposition:
- No suicidality → Discharge + PCP/psychiatry follow-up + CBT education
- Suicidal/homicidal → Psychiatric admission
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Ch. 98 (Anxiety Disorders)
- Tintinalli's Emergency Medicine: A Comprehensive Study, Ch. 289 (Anxiety Disorders) - Table 289-7
Create a comparison poster: Panic Disorder vs. Cardiogenic Chest Pain
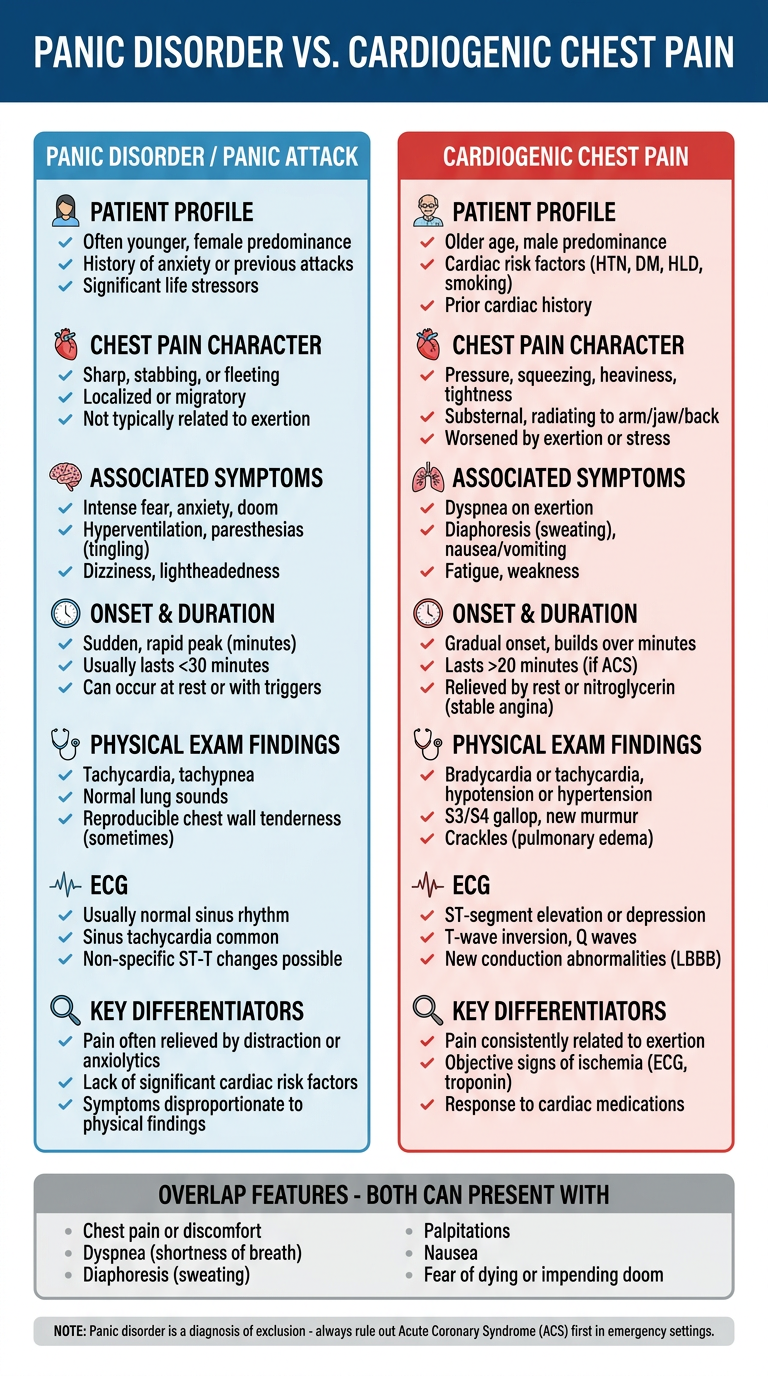
- Patient profile: younger females with psychiatric history (panic) vs. older patients with cardiac risk factors (cardiogenic)
- Pain character: atypical, variable, positional vs. classic pressure/squeezing, radiation to arm/jaw
- Associated symptoms: derealization, paresthesias, fear of "going crazy" (panic) vs. diaphoresis, nausea, syncope (cardiac)
- Onset/duration: peaks in minutes, resolves in under 1 hour (panic) vs. persistent, crescendo pattern (cardiac)
- ECG: normal or sinus tachycardia (panic) vs. ST changes, LBBB, T-wave inversions (cardiac)
- Overlap zone: both share chest pain, dyspnea, palpitations, diaphoresis, and fear of dying - reinforcing the bottom-line reminder that panic disorder is always a diagnosis of exclusion.
Explain what happens when you're attached to person and they suddenly leave, explain neurobiochemical basis
"social attachment" AND "neurobiological" AND "separation"
grief bereavement neurobiology dopamine opioid
social attachment loss neurobiology opioid dopamine oxytocin
The Neurobiochemistry of Losing an Attachment Figure
1. What Attachment Actually Does to the Brain - The Baseline State
Oxytocin and Vasopressin - The "Bonding Molecules"
- Attachment and pair bonding
- Fear extinction
- Emotion recognition
- Empathy
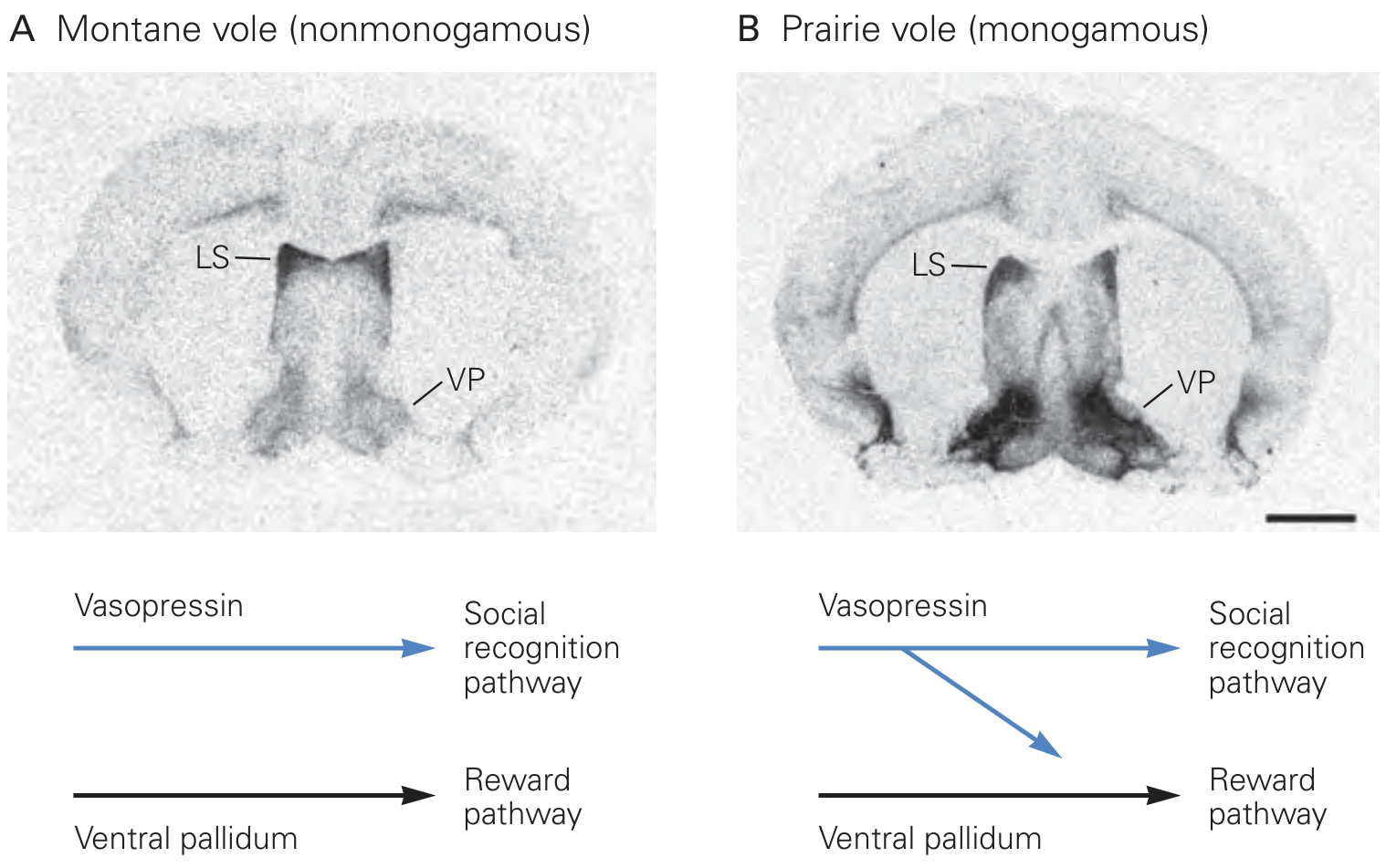
- Principles of Neural Science, 6th Ed. (Kandel), Ch. 2
Dopamine - The Reward Prediction System
- You develop a conditioned dopaminergic response to cues associated with that person
- Anticipation of seeing them generates dopamine ("wanting")
- Their presence generates opioid release ("liking")
Endogenous Opioids - The "Comfort" System
"Growing literature describes the opioid system as a powerful modulator of social separation distress and attachment formation in rodents and primates... endogenous opioids are key to forming and sustaining social bonds."
- Galiza Soares et al., Frontiers in Neuroanatomy, 2024 [PMID: 39917739]
2. What Happens When They Leave - The Cascade
Phase 1: Immediate (Minutes to Hours) - Acute Stress Response
- Pituitary ACTH release
- Adrenal cortisol secretion
Phase 2: Hours to Days - Withdrawal State
- The conditioned reward cues (their texts, their smell, their voice) are still present in your environment
- They trigger dopamine-mediated craving and anticipation
- But no reward is delivered
Decrease in dopamine release and function in the nucleus accumbens is the neurochemical signature of withdrawal, along with powerful craving. Sensitization of dopamine responses can persist long after the source ceases and relates to craving and relapse.
- Neuroscience: Exploring the Brain, 5th Ed.; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- A drop in endogenous opioid tone
- The emotional equivalent of opioid withdrawal: dysphoria, aching emptiness, hypersensitivity to pain, irritability
- Separation distress calls in animal models are directly suppressed by opioid administration and triggered by opioid antagonists - the same pattern as physical pain
- Disrupts fear extinction circuits (fears that were suppressed in their presence resurface)
- Impairs social reward processing
- Reduces empathy calibration and emotional regulation
Phase 3: The Pain Is Literally Pain - The Anterior Cingulate Cortex
"The finding that social rejection is mediated in the same part of the brain as physical pain - the dorsal anterior cingulate cortex - suggests that the fear of social engagement is tantamount to a fear of being injured. Some studies suggest that the experimental use of pain-relieving medications even temporarily reduces social pain."
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Phase 4: Serotonin and the Mood Disruption
- Low mood, sadness
- Rumination (repetitive, circular negative thinking)
- Sleep disruption (especially early morning waking - a classic serotonin/norepinephrine-deficient pattern)
- Appetite changes
3. Why Some People Are Hit Harder - Individual Variation
| Factor | Mechanism |
|---|---|
| Attachment style (anxious) | Overactivated amygdala baseline; hyperreactive to rejection cues |
| Early life adversity | Disrupts oxytocinergic and opioid circuit development; increases HPA reactivity |
| Depth of the bond | Greater dopamine conditioning; more opioid tone to lose |
| Sudden vs. gradual loss | Sudden loss removes the regulatory signal without time for adaptive downregulation |
| Social isolation | No compensatory opioid/oxytocin sources; escalates deprivation |
Summary: The Full Cascade
Attachment present
↓
Oxytocin / vasopressin → bonding & recognition
Dopamine (VTA → nucleus accumbens) → reward, anticipation
Endogenous opioids → comfort, social analgesia
Cortisol / HPA → suppressed (co-regulation)
Amygdala → quieted (fear extinction)
--- Person LEAVES suddenly ---
↓
HPA axis fires → cortisol surge → stress response
Amygdala activates → hypervigilance, rumination
Norepinephrine rises → physical arousal, anxiety
Dopamine drops → anhedonia, craving, compulsive thoughts
Opioid tone falls → aching emptiness, dysphoria, pain hypersensitivity
Oxytocin/vasopressin destabilizes → fears re-emerge, emotion dysregulation
Serotonin disruption → low mood, sleep disturbance
Dorsal ACC activates → the loss literally registers as pain
- Principles of Neural Science, 6th Ed. (Kandel), Ch. 2 - oxytocin/vasopressin pair bonding circuits
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - dACC social pain, dopamine social reward
- Harrison's Principles of Internal Medicine, 22nd Ed. - oxytocin as neurotransmitter in socioemotional functioning
- Neuroscience: Exploring the Brain, 5th Ed. - dopamine, nucleus accumbens, withdrawal
- Galiza Soares et al. (2024). "Opioidergic tuning of social attachment." Frontiers in Neuroanatomy [PMID: 39917739]
Tell about changing epidemiology of liver cirrhosis
"liver cirrhosis" AND epidemiology AND trends
changing epidemiology liver cirrhosis MASLD NAFLD alcohol 2024 2025 global trends
changing epidemiology liver cirrhosis NAFLD MASLD alcohol HBV HCV trends global burden
"MASLD" OR "metabolic dysfunction associated" AND cirrhosis AND epidemiology
Changing Epidemiology of Liver Cirrhosis
1. Scale of the Problem - The Global Burden
- 58.4 million incident cases globally in 2021, up from 36.9 million in 1990 (Global Burden of Disease 2021)
- >1.32 million deaths per year worldwide; ~45,000 per year in the United States, making it the 11th leading cause of death
- Primarily affects individuals aged 25-64 years - their most economically productive decades - with enormous economic consequences from disability and premature death
- Global prevalence of cirrhosis in the general population: 1.3% (95% CI 0.9-1.7%), with advanced fibrosis at 3.3%; both rising significantly since 2016
- DALYs (disability-adjusted life years) have declined on an age-standardized basis since 1990 due to viral hepatitis control, but the absolute burden continues to grow driven by MASLD and alcohol
"Cirrhosis annually causes more than 1.32 million deaths worldwide... chronic liver disease mainly affects individuals between 25 and 64 years of age, with a significant impact on the economy."
- Goldman-Cecil Medicine, Ch. 139
2. The Etiological Shift - What's Changing
A. MASLD/NAFLD - The Rising Dominant Force
| Metric | Figure |
|---|---|
| Global adult population affected | ~30-40% (MASLD); 38% by recent meta-analyses |
| Individuals with type 2 diabetes | 60-70% have MASLD |
| Individuals with obesity | 70-80% have MASLD |
| MASLD cirrhosis incidence (1990) | 24.8 million cases |
| MASLD cirrhosis incidence (2021) | 48.3 million - near doubling in 30 years |
| EAPC (annual % change in incidence) | +0.73 - fastest among all etiologies |
- Global obesity epidemic - particularly in middle-income countries undergoing nutritional transition
- Type 2 diabetes pandemic
- Urbanization and sedentary lifestyles
- Dietary shifts toward ultra-processed foods, fructose, and refined carbohydrates
- Younger age of onset - individuals affected earlier have more time to develop severe complications
MASLD affects ~30-40% of the global adult population and is associated with cirrhosis, hepatocellular carcinoma, cardiovascular disease, and extrahepatic cancers. Resmetirom and semaglutide are now conditionally FDA-approved for MASH with moderate-to-advanced fibrosis.
- Tilg et al., JAMA 2026 [PMID: 41212550]
B. Alcohol-Associated Liver Disease (ALD) - A Persistent and Resurging Threat
- Global alcohol per-capita consumption rose from 5.5 litres in 2005 → 6.4 litres in 2016, projected to reach 7.6 litres by 2030
- The global estimated age-standardized death rate (ASDR) for alcohol-associated cirrhosis was 4.5 per 100,000 population
- Between 2012 and 2017, ASDR for alcohol cirrhosis slightly declined - but absolute deaths rose: from 223,000 in 1990 to 354,000 in 2021
- The ASDR for alcohol-associated liver cancer increased even as cirrhosis rates slightly fell
- Degree and duration of alcohol intake (15-20% of heavy drinkers develop cirrhosis)
- Female sex (greater susceptibility per unit consumed)
- Obesity and type 2 diabetes (synergistic hepatotoxicity)
- Gut microbial dysbiosis
- Genetic variants (e.g., PNPLA3, TM6SF2)
"Alcohol was associated with approximately one-fifth of global HCC-related deaths in 2019. Measures are required to curb heavy alcohol consumption to reduce the burden of alcohol-associated cirrhosis and HCC."
- Huang et al., Nat Rev Gastroenterol Hepatol 2023 [PMID: 36258033]
C. Viral Hepatitis (HBV/HCV) - Declining but Still Dominant Globally
| Etiology | Trend (EAPC) | Key driver |
|---|---|---|
| HBV-cirrhosis | -2.74 (fastest declining) | Universal infant vaccination, antivirals (TDF, entecavir) |
| HCV-cirrhosis | -0.51 | Direct-acting antivirals (DAAs) achieving >95% SVR |
- Still the primary cause of cirrhosis in China, sub-Saharan Africa, and Southeast Asia
- Universal HBV vaccination programs since the 1990s have dramatically cut new infections
- Long-term TDF/entecavir therapy achieves cirrhosis regression in 75% of responders at 5 years
- However, 296 million people globally remain chronically infected - the legacy burden persists for decades
- Was the most common cause of cirrhosis in the United States until DAAs became widely available (2013-2014)
- DAAs (sofosbuvir-based regimens) cure >95% of patients within 8-12 weeks
- However, in low/middle-income countries, access to DAAs remains inequitable, and HCV cirrhosis burden continues in these regions
"Hepatitis C was the most common cause of cirrhosis in the United States until effective antiviral therapy became available... many cases of cryptogenic cirrhosis are now thought to be due to nonalcoholic steatohepatitis."
- Goldman-Cecil Medicine, Ch. 139
3. Special Populations and Emerging Shifts
Pediatric and Adolescent Cirrhosis
- Global incidence of cirrhosis in children and adolescents has risen
- HBV-related cirrhosis declining in the young (vaccination impact)
- HCV, NAFLD, and alcohol-related cirrhosis increasing in this age group
- Childhood obesity epidemic is producing MASH in teenagers - a cohort who will reach cirrhosis-risk age much earlier than prior generations
The "Dual Etiology" and "Multi-Hit" Problem
- MASLD + alcohol (ALD + MASLD overlap, now termed MetALD in the new nomenclature)
- MASLD + HCV (metabolic syndrome accelerates HCV fibrosis)
- Heavy alcohol + obesity (synergistically accelerating cirrhosis)
Geographic Divergence
| Region | Dominant etiology shifting TO |
|---|---|
| Western Europe / North America | MASLD, ALD |
| East Asia (China, Korea, Japan) | MASLD (surpassing HBV in younger cohorts) |
| Sub-Saharan Africa | HBV still dominant; MASLD emerging |
| South Asia | HBV + MASLD convergence |
| Middle East | Very high MASLD rates (driven by obesity/T2DM) |
4. Mortality Trends - The Paradox
- Age-standardized mortality rates (ASMR) are declining overall - reflecting improved detection, management (beta-blockers, banding, liver transplant, antivirals)
- Absolute deaths are rising - because the denominator of at-risk people (particularly MASLD and ALD) is growing faster than treatment gains can offset
- The ASDR for NAFLD/MASLD-associated cirrhosis increased even while all other etiologies' ASDRs declined
- Projections: total cirrhosis deaths will increase in the next decade if MASLD and alcohol trends continue unchecked
"The global number of deaths from cirrhosis increased between 2012 and 2017, but age-standardized death rates declined. However, the ASDR for NAFLD-associated cirrhosis increased... the number of deaths from cirrhosis is projected to increase in the next decade."
- Huang et al., Nat Rev Gastroenterol Hepatol 2023 [PMID: 36977794]
5. Summary: The Etiological Transition at a Glance
PAST (pre-2000) NOW / FUTURE
─────────────────────────────────────────────────────────
HBV/HCV dominant globally → HBV/HCV declining (vaccines + antivirals)
HCV dominant in USA/Europe → MASLD/ALD now leading in high-income countries
NAFLD: rare/underrecognized → MASLD: #1 cause by incidence globally
ALD: stable or declining → ALD: rising again (pandemic, alcohol normalization)
Cirrhosis = older males → Cirrhosis moving younger, more females (MASLD)
Single etiology → Dual/multi-etiology increasingly common
Key References
| Source | Contribution |
|---|---|
| Huang DQ et al. Nat Rev Gastroenterol Hepatol 2023 [PMID: 36977794] | Comprehensive global epidemiology, trends, predictions |
| Huang DQ et al. Nat Rev Gastroenterol Hepatol 2023 [PMID: 36258033] | Alcohol-associated cirrhosis & HCC global epidemiology |
| Zamani M et al. Clin Gastroenterol Hepatol 2025 [PMID: 39209202] | Systematic review/meta-analysis: global prevalence of cirrhosis |
| Wong VW et al. J Hepatol 2023 [PMID: 37169151] | Changing epidemiology of NAFLD/MASLD |
| Tilg H et al. JAMA 2026 [PMID: 41212550] | Current MASLD review including FDA-approved therapies |
| GBD 2021 Cirrhosis Study (PMC12273999) | NAFLD incidence doubled 1990-2021; HBV/HCV declining |
| Goldman-Cecil Medicine, Ch. 139 | Textbook epidemiology and etiology overview |
| Textbook of Family Medicine 9e, Ch. 38 | Cirrhosis causes and complications overview |