Rewrite the whole content as it is plus add maximum number of high yield images along the content from your side
# Physiology of General Principles of Gastrointestinal Function
## Comprehensive Guide: Motility, Nervous and Hormonal Control, Blood Circulation, and Microbiota
---
# PART 1: OVERVIEW OF THE GASTROINTESTINAL (GI) TRACT
## Basic Architecture
The gastrointestinal tract is essentially a **long muscular tube** extending from the mouth to the anus, approximately **9 meters (30 feet)** in length in a cadaver (shorter in living persons due to tonic muscle contraction). Its primary functions are:
1. **Motility** – movement and mixing of food
2. **Secretion** – digestive juices and enzymes
3. **Digestion** – breakdown of food
4. **Absorption** – nutrient uptake
5. **Storage and excretion** – waste elimination
6. **Barrier and immune function** – defense against pathogens
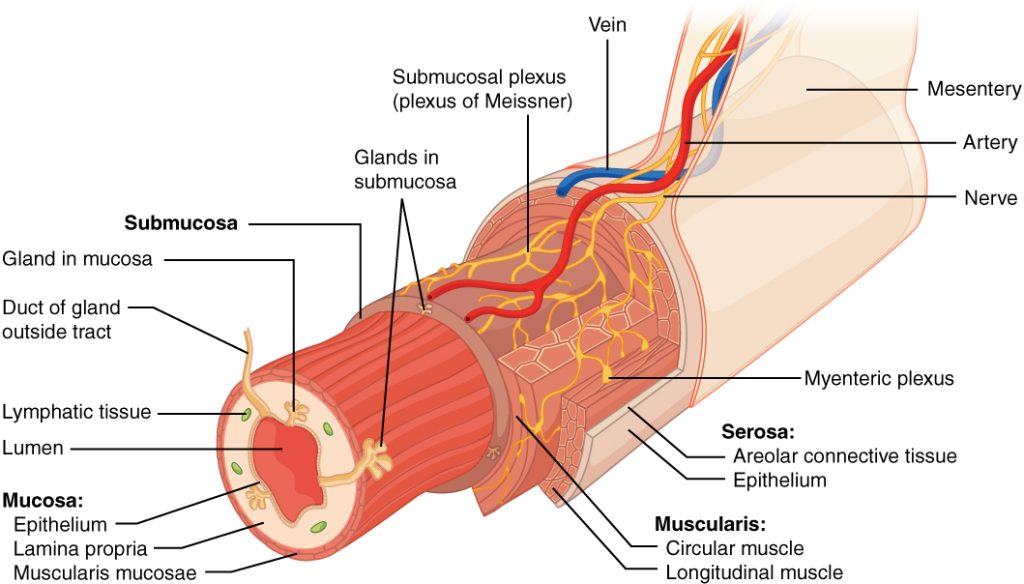
## Layers of the GI Wall (from lumen outward)
Understanding the wall structure is essential because motility, nervous control, and blood flow all depend on it.
### 1. Mucosa (innermost layer)
- **Epithelium**: Single layer; varies by region (stratified squamous in esophagus and anal canal; simple columnar in stomach and intestines)
- **Lamina propria**: Loose connective tissue containing blood vessels, lymphatics, immune cells (MALT – mucosa-associated lymphoid tissue), and glands
- **Muscularis mucosae**: Thin smooth muscle layer that creates local movements and folding of the mucosa, independent of the main muscle layers
### 2. Submucosa
- Dense connective tissue
- Contains **Meissner's plexus** (submucosal plexus) – part of the enteric nervous system
- Contains larger blood vessels, lymphatics, and glands (e.g., Brunner's glands in the duodenum)
### 3. Muscularis Externa (Muscularis Propria)
- **Inner circular layer**: When it contracts, it narrows the lumen
- **Myenteric plexus (Auerbach's plexus)**: Located between the two muscle layers – controls motility
- **Outer longitudinal layer**: When it contracts, it shortens the segment
- **Exception**: The stomach has an **additional oblique layer** (innermost) for churning
- **Exception**: The large intestine's longitudinal layer is gathered into three bands called **teniae coli**
### 4. Serosa (Adventitia)
- Outermost layer
- In the peritoneal cavity: **serosa** (visceral peritoneum) – mesothelium with thin connective tissue
- In retroperitoneal structures and esophagus: **adventitia** – connective tissue that merges with surrounding structures
> **CLINICAL: Hirschsprung's Disease (Congenital Aganglionic Megacolon)**
> - Absence of ganglion cells in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses in a segment of the colon (usually the rectosigmoid region)
> - Due to failure of migration of neural crest cells during embryonic development
> - The aganglionic segment remains tonically contracted → functional obstruction
> - Proximal normal bowel dilates massively (megacolon)
> - Presents in neonates with failure to pass meconium within 48 hours, abdominal distension, and bilious vomiting
> - Diagnosis: Rectal suction biopsy showing absence of ganglion cells, with nerve fiber hypertrophy (hypertrophied nerve trunks staining for acetylcholinesterase)
> - Treatment: Surgical resection of aganglionic segment (pull-through procedure)
---
# PART 2: GASTROINTESTINAL MOTILITY
## A. Smooth Muscle of the GI Tract
### Types of Smooth Muscle in GI
**1. Unitary (Single-unit) Smooth Muscle**
- This is the predominant type in the GI tract
- Cells are connected by **gap junctions** (connexons made of connexin proteins)
- Gap junctions allow electrical coupling → entire sheets of muscle act as a **functional syncytium**
- Action potentials spread from cell to cell
- This explains why contraction waves can propagate along the gut wall
**2. Multi-unit Smooth Muscle**
- Found in the **muscularis mucosae** and in some sphincters
- Each fiber contracts independently
- More precise neural control
### Electrical Activity of GI Smooth Muscle
The electrical activity of GI smooth muscle is unique and forms the basis of all motility patterns.
#### a. Resting Membrane Potential (RMP)
- Ranges from **-50 to -60 mV** (less negative than skeletal muscle at -90 mV)
- This relatively depolarized state is due to higher Na⁺ permeability
- The RMP is not stable – it fluctuates
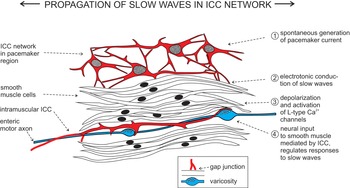
#### b. Slow Waves (Basic Electrical Rhythm, BER)
This is one of the most important concepts in GI physiology.
- **Definition**: Rhythmic, spontaneous oscillations in the resting membrane potential of GI smooth muscle
- **NOT action potentials** – they are undulating changes in membrane potential
- **Amplitude**: 5–15 mV oscillations
- **Origin**: Generated by the **Interstitial Cells of Cajal (ICC)**
##### Interstitial Cells of Cajal (ICC) – The GI Pacemaker Cells
- Located at the interface between the circular muscle layer and the myenteric plexus (ICC-MY) and within the muscle layers (ICC-IM)
- Connected to smooth muscle cells via gap junctions
- They are **mesenchymal** in origin (not neural, not muscle)
- They express the **c-Kit receptor** (a tyrosine kinase receptor) – this is a defining marker
- Mechanism of slow wave generation:
- Cyclic release and uptake of Ca²⁺ from intracellular stores (endoplasmic reticulum)
- Activation of Ca²⁺-activated Cl⁻ channels → Cl⁻ efflux → depolarization (because intracellular Cl⁻ concentration is high in ICC)
- This spontaneous depolarization-repolarization cycle creates the slow wave
- The slow wave then spreads to adjacent smooth muscle cells via gap junctions
> **CLINICAL: Gastrointestinal Stromal Tumors (GISTs)**
> - Tumors arising from the Interstitial Cells of Cajal or their precursors
> - Most common mesenchymal tumor of the GI tract
> - Most frequently found in the **stomach** (60-70%) and small intestine (20-30%)
> - Characterized by **c-Kit (CD117) positivity** on immunohistochemistry
> - Many have activating mutations in the **KIT gene** or **PDGFRA gene**
> - Treatment: Surgical resection + **Imatinib** (Gleevec) – a tyrosine kinase inhibitor that targets c-Kit
> - Loss of ICC function can cause **gastroparesis** and **chronic intestinal pseudo-obstruction**
##### Slow Wave Frequencies (MUST know)
These are intrinsic to each region and set the **maximum frequency** of contractions:
| Region | Slow Wave Frequency (per minute) |
|--------|----------------------------------|
| Stomach (body/antrum) | 3 per minute |
| Duodenum | 12 per minute (highest!) |
| Jejunum | 8-9 per minute |
| Ileum | 8-9 per minute |
| Cecum/Ascending colon | 6 per minute |
| Sigmoid colon | 6-12 per minute |
| Rectum | Variable |
**Key points about slow waves:**
- Slow waves determine the **timing** and **rhythm** of contractions
- Slow waves by themselves usually do **NOT** cause muscle contraction (except in the stomach where large slow waves can cause weak contractions)
- Contraction occurs only when the slow wave depolarizes the membrane enough to reach **threshold** and trigger **spike potentials (action potentials)**
- The strength of contraction depends on the **number of action potentials** firing during the depolarization phase of the slow wave
#### c. Spike Potentials (Action Potentials)
- True action potentials superimposed on the peaks of slow waves
- Occur when the slow wave peak reaches threshold (approximately -40 mV)
- Duration: 10–40 milliseconds (much longer than skeletal muscle APs which last 1-2 ms)
- **Ionic basis**:
- **Depolarization**: Ca²⁺ influx through **L-type voltage-gated Ca²⁺ channels** (NOT Na⁺ channels as in skeletal muscle!) + some Na⁺ influx through Ca²⁺-Na⁺ channels (slow channels)
- **Repolarization**: K⁺ efflux through voltage-gated K⁺ channels
- The Ca²⁺ entry during the spike is crucial because it directly triggers contraction (excitation-contraction coupling)
> This is why **calcium channel blockers** (e.g., verapamil, nifedipine) can reduce GI motility and cause **constipation** as a side effect.
#### d. Factors Affecting the Electrical Activity
**Factors that DEPOLARIZE (make more positive, increase excitability → more contractions):**
- Stretch of the muscle wall
- Acetylcholine (parasympathetic)
- Substance P
- Serotonin (5-HT)
- Gastrin, CCK, motilin
**Factors that HYPERPOLARIZE (make more negative, decrease excitability → fewer contractions):**
- Norepinephrine and epinephrine (sympathetic)
- VIP (vasoactive intestinal peptide)
- Nitric oxide (NO)
- ATP (purinergic inhibition)
- Secretin, glucagon
### Excitation-Contraction Coupling in GI Smooth Muscle
1. Ca²⁺ enters during spike potentials (through L-type Ca²⁺ channels)
2. Additional Ca²⁺ released from sarcoplasmic reticulum (via IP₃-mediated release or calcium-induced calcium release, CICR)
3. Ca²⁺ binds to **calmodulin** (NOT troponin as in skeletal muscle)
4. Ca²⁺-calmodulin complex activates **myosin light chain kinase (MLCK)**
5. MLCK phosphorylates the **regulatory light chain of myosin** (Ser-19)
6. Phosphorylated myosin interacts with actin → cross-bridge cycling → contraction
7. Relaxation: **Myosin light chain phosphatase (MLCP)** dephosphorylates myosin light chain
**Latch state**: Unique to smooth muscle – after initial phosphorylation, myosin can maintain tension with very low energy expenditure even after dephosphorylation. This is important in sphincters that must remain tonically contracted.
> **CLINICAL: Achalasia**
> - Failure of the lower esophageal sphincter (LES) to relax during swallowing
> - Due to loss of inhibitory neurons (VIP and NO-producing neurons) in the myenteric plexus of the LES
> - The LES remains in a "latch state" of sustained contraction
> - Results in dysphagia (difficulty swallowing), regurgitation, chest pain
> - **Bird's beak** appearance on barium swallow
> - Can be secondary to **Chagas disease** (Trypanosoma cruzi destroys ganglion cells)
> - Treatment: Pneumatic dilation, Heller myotomy, botulinum toxin injection, or peroral endoscopic myotomy (POEM)
---
## B. Types of GI Motility
### 1. Peristalsis
**Definition**: A coordinated wave of contraction preceded by a wave of relaxation that propels luminal contents in the aboral direction (away from mouth, toward anus).
**Mechanism – The "Law of the Intestine" (Bayliss and Starling, 1899)**
This is also called the **peristaltic reflex** or the **myenteric reflex**:
When a bolus distends the gut wall at a point:
1. **Behind the bolus (oral side)**: Contraction occurs
- Circular muscle contracts (narrows lumen)
- Longitudinal muscle relaxes (lengthens segment)
- Mediated by excitatory neurons releasing **ACh** and **Substance P**
2. **Ahead of the bolus (aboral side)**: Relaxation occurs ("receptive relaxation")
- Circular muscle relaxes (widens lumen)
- Longitudinal muscle contracts (shortens segment)
- Mediated by inhibitory neurons releasing **VIP** and **Nitric Oxide (NO)**
**This entire reflex is coordinated by the myenteric plexus (Auerbach's) and can occur in the complete absence of extrinsic innervation!**
**Speed and characteristics:**
- Esophagus: Primary peristalsis travels at 2–4 cm/sec
- Small intestine: 0.5–2 cm/sec
- Colon: Very slow, may take hours for contents to traverse
**Types of peristalsis in the esophagus:**
- **Primary peristalsis**: Initiated by swallowing; continues the pharyngeal peristaltic wave
- **Secondary peristalsis**: Initiated by distension of the esophagus (e.g., retained food bolus); does NOT require a swallow
- **Tertiary contractions**: Non-peristaltic, simultaneous, disorganized contractions; pathological – seen in **diffuse esophageal spasm**
> **CLINICAL: Diffuse Esophageal Spasm**
> - Simultaneous, uncoordinated contractions of the esophageal body
> - "Corkscrew esophagus" or "rosary bead esophagus" on barium swallow
> - High-amplitude, simultaneous contractions on manometry
> - Causes intermittent dysphagia and severe chest pain (can mimic angina!)
> - Treatment: Calcium channel blockers, nitrates, tricyclic antidepressants, botulinum toxin
> **CLINICAL: Scleroderma (Systemic Sclerosis) Esophagus**
> - Fibrosis and atrophy of the smooth muscle in the lower 2/3 of esophagus
> - Loss of peristalsis in the smooth muscle portion
> - Decreased LES pressure → severe GERD
> - Upper 1/3 (skeletal muscle) is spared
> - Can lead to Barrett's esophagus and strictures
### 2. Segmentation
**Definition**: Rhythmic contractions that divide and subdivide the intestinal contents, mixing them thoroughly with digestive juices and bringing them into contact with the absorptive surface.
- Does NOT propel contents significantly – primarily a **mixing** movement
- Predominant motility pattern of the **small intestine** during digestion
- Adjacent segments of circular muscle contract alternately → the chyme is repeatedly divided and recombined
- Frequency is determined by the slow wave frequency of that region
- Segmentation contractions are **more frequent proximally** than distally → this frequency gradient slowly moves chyme aborally
### 3. Tonic Contractions
- Sustained contractions lasting minutes to hours
- Found in **sphincters** (LES, pyloric sphincter, ileocecal valve, internal anal sphincter)
- Also found in the proximal stomach (for reservoir function)
- Maintain closure and prevent backflow
- Sphincters relax at appropriate times to allow passage
### 4. Mass Movements (Mass Peristalsis)
- Occur in the **large intestine**
- A strong peristaltic wave that propels colonic contents over a long distance
- Occurs **1–3 times per day**, often after meals (due to gastrocolic reflex)
- Involves contraction of a long segment that pushes contents toward the rectum
- Initiated by the **gastrocolic reflex** (stomach distension → increased colonic motility) and the **duodenocolic reflex**
> **CLINICAL: Irritable Bowel Syndrome (IBS)**
> - Functional GI disorder with altered motility, visceral hypersensitivity, and brain-gut axis dysfunction
> - Abnormal segmentation patterns and altered slow wave frequencies
> - IBS-D (diarrhea): Increased mass movements, rapid transit
> - IBS-C (constipation): Decreased mass movements, slow transit
> - Visceral hypersensitivity to distension (lower pain thresholds during balloon distension tests)
> - Altered serotonin (5-HT) signaling plays a major role
> - Treatments: Antispasmodics, 5-HT₃ antagonists (alosetron for IBS-D), 5-HT₄ agonists (prucalopride for IBS-C), low FODMAP diet
### 5. Migrating Motor Complex (MMC)
This is the **"housekeeper" of the gut** during the **interdigestive (fasting) state**.
**Definition**: A cyclical pattern of electrical and motor activity that migrates from the stomach to the terminal ileum during fasting, sweeping undigested material, bacteria, and debris from the upper GI tract.
**Phases of the MMC:**
1. **Phase I** (Quiescent phase): ~40-60% of cycle; NO contractions; slow waves present but no spikes
2. **Phase II** (Intermittent activity): ~20-30% of cycle; irregular contractions of increasing intensity
3. **Phase III** (Maximal activity): ~5-10 minutes; burst of intense, regular contractions at maximum slow wave frequency (the "activity front"); this is the main propulsive phase
4. **Phase IV** (Transitional): Brief transition back to Phase I
**Cycle duration**: Each cycle lasts approximately **90-120 minutes**
**Important details:**
- **Motilin** is the primary hormone that initiates Phase III of the MMC
- Motilin is released cyclically from Mo cells in the duodenum and jejunum
- Motilin levels peak just before Phase III and decline during it
- **Erythromycin** is a macrolide antibiotic that acts as a **motilin receptor agonist** → stimulates Phase III-like contractions
- Feeding ABOLISHES the MMC → replaced by the fed pattern (segmentation)
- Vagal tone modulates MMC but is not absolutely required
> **CLINICAL: Small Intestinal Bacterial Overgrowth (SIBO)**
> - Normal MMC sweeps bacteria distally, preventing overgrowth in the small intestine
> - When MMC is disrupted (e.g., in diabetic gastroparesis, scleroderma, post-surgical states, opioid use), bacteria proliferate in the small bowel
> - Causes bloating, diarrhea, malabsorption, steatorrhea, vitamin B12 deficiency (bacteria consume B12), folate may be normal or elevated (bacteria produce folate)
> - Diagnosis: Hydrogen breath test, jejunal aspirate >10⁵ CFU/mL
> - Treatment: Antibiotics (rifaximin), prokinetics (erythromycin), treat underlying cause
> **CLINICAL: Gastroparesis**
> - Delayed gastric emptying in the absence of mechanical obstruction
> - Most common causes: Diabetes mellitus (vagal neuropathy), idiopathic, post-surgical
> - Loss of ICC networks, impaired vagal function, disrupted MMC
> - Symptoms: Early satiety, nausea, vomiting, bloating, abdominal pain
> - Diagnosis: Gastric emptying scintigraphy (4-hour study with radiolabeled meal)
> - Treatment: Dietary modification, metoclopramide (D₂ antagonist, 5-HT₄ agonist), erythromycin (motilin agonist), domperidone, gastric electrical stimulation
### 6. Haustral Contractions
- Characteristic of the **colon**
- Rings of circular muscle contraction that form the **haustra** (pouches)
- Slowly migrate → mix contents and facilitate water absorption
- Similar to segmentation but much slower
### 7. Receptive Relaxation
- Occurs in the **stomach** (fundus and body) when food enters
- Mediated by the **vagovagal reflex**
- Neurotransmitters: **VIP and NO** from inhibitory vagal efferents
- Allows the stomach to accommodate large volumes (up to 1.5 L) without significant increase in intragastric pressure
> **CLINICAL: Dumping Syndrome**
> - Occurs after gastric surgery (vagotomy, gastrectomy, bypass)
> - Loss of receptive relaxation and pyloric regulation → rapid gastric emptying of hyperosmolar contents into the duodenum
> - **Early dumping** (15-30 min after eating): Fluid shifts into bowel lumen (osmotic) → abdominal cramping, diarrhea, vasomotor symptoms (tachycardia, sweating, dizziness)
> - **Late dumping** (1-3 hours after eating): Reactive hypoglycemia due to excessive insulin release triggered by rapid glucose absorption
> - Management: Small frequent meals, avoid simple carbs, octreotide for refractory cases
---
## C. Regional Motility Patterns
### Esophageal Motility
**Upper Esophageal Sphincter (UES):**
- **Skeletal muscle** (cricopharyngeus muscle)
- Tonically contracted at rest (prevents air swallowing)
- Relaxes during swallowing (coordination via swallowing center in medulla)
**Esophageal Body:**
- Upper 1/3: Skeletal muscle (voluntary)
- Middle 1/3: Mixed skeletal and smooth muscle
- Lower 1/3: Smooth muscle (involuntary)
- The entire esophagus participates in peristalsis during swallowing
**Lower Esophageal Sphincter (LES):**
- Physiological sphincter (not a distinct anatomical structure, but a zone of high pressure)
- **Smooth muscle**
- Tonically contracted at rest (resting pressure ~15-30 mmHg above intragastric pressure)
- Maintains **tonic contraction** through intrinsic myogenic mechanisms + cholinergic (vagal) stimulation
- Relaxes during swallowing via **VIP and NO** from inhibitory vagal fibers
- Reinforced by the crura of the diaphragm
**Factors affecting LES tone:**
| Increase LES tone | Decrease LES tone |
|---|---|
| Gastrin | Secretin |
| Motilin | CCK |
| Substance P | VIP, NO |
| ACh (muscarinic) | Progesterone |
| α-adrenergic agonists | Dopamine |
| Proteins in meal | Fat in meal |
| Metoclopramide | Chocolate, caffeine, alcohol |
| Cisapride | Smoking |
| | Calcium channel blockers |
| | Nitrates |
| | Theophylline |
| | Anticholinergics |
> **CLINICAL: Gastroesophageal Reflux Disease (GERD)**
> - Transient lower esophageal sphincter relaxations (TLESRs) are the most common mechanism (NOT chronically low LES pressure in most cases)
> - TLESRs are vagally mediated relaxations unrelated to swallowing
> - Risk factors: Obesity, pregnancy (progesterone), hiatal hernia, certain foods/drugs
> - Complications: Esophagitis, strictures, Barrett's esophagus (intestinal metaplasia → risk of adenocarcinoma)
> - Treatment: PPIs, H₂ blockers, lifestyle modifications, surgical fundoplication
### Gastric Motility
**Functional divisions of the stomach:**
1. **Proximal stomach** (fundus + upper body): Reservoir function
- Receptive relaxation (vagovagal reflex) and adaptive relaxation (accommodation)
- Generates slow, sustained tonic contractions that push contents toward the distal stomach
2. **Distal stomach** (lower body + antrum): Mixing and grinding
- Powerful peristaltic contractions (3/min, matching slow wave frequency)
- The antral pump: Strong antral contractions propel chyme toward the pylorus
- **Retropulsion**: The pylorus closes before the peristaltic wave reaches it → chyme is squirted back into the body → grinding effect
- This cycle repeats, reducing particle size to <2 mm for emptying
**Gastric Emptying:**
**Emptying of liquids:**
- Determined primarily by the **tone** of the proximal stomach
- Follows **first-order kinetics** (exponential decline)
- Liquids empty faster than solids
**Emptying of solids:**
- Determined by the **strength of antral contractions**
- Has an initial **lag phase** (grinding) followed by a **linear emptying phase**
- Particles must be reduced to <1-2 mm to pass through the pylorus
**Regulation of gastric emptying:**
*Factors that INCREASE gastric emptying:*
- Gastric distension (stretch → vagal afferents → increased contractions)
- Motilin
- Gastrin (initially promotes emptying by enhancing antral contractions)
- Parasympathetic stimulation
*Factors that DECREASE gastric emptying (feedback from duodenum):*
- Fat in the duodenum (most potent inhibitor!) → CCK release
- Acid in the duodenum → secretin release
- Hyperosmolar content in the duodenum
- Distension of the duodenum
- CCK → contracts pyloric sphincter + relaxes proximal stomach
- Secretin, GIP
- Sympathetic stimulation (stress, pain)
> The **enterogastric reflex** is the neural reflex from duodenum to stomach that inhibits gastric motility when the duodenum is overloaded with chyme.
**Indigestible solids (>2 mm):**
- NOT emptied during the fed state
- Emptied during Phase III of the MMC (interdigestive period)
- This is why large indigestible objects (pills, foreign bodies) are passed between meals
> **CLINICAL: Pyloric Stenosis (Infantile Hypertrophic)**
> - Hypertrophy of the pyloric smooth muscle (especially circular layer)
> - Presents at 2-8 weeks of age (more common in firstborn males)
> - **Projectile, non-bilious vomiting** after feeding
> - Palpable "olive-shaped" mass in the right upper quadrant
> - **Hypochloremic, hypokalemic metabolic alkalosis** (loss of HCl in vomitus)
> - Paradoxical aciduria: Kidneys excrete H⁺ to retain K⁺ and Na⁺
> - Diagnosis: Ultrasound (pyloric muscle thickness >3mm, length >15mm)
> - Treatment: Ramstedt pyloromyotomy (surgical splitting of pyloric muscle)
### Small Intestinal Motility
**Fed state:**
- **Segmentation** is the predominant pattern
- Frequency: ~12/min in duodenum, decreasing to ~8/min in ileum (following slow wave frequency gradient)
- This frequency gradient causes net aboral movement of contents
- Transit time through small intestine: 3-5 hours
**Fasting state:**
- **MMC** takes over (described above)
**Ileocecal Valve (Sphincter):**
- Prevents reflux of colonic contents (and bacteria) back into the small intestine
- Normally tonically contracted
- Relaxes when ileal peristalsis reaches it (via intrinsic reflexes)
- Contraction is enhanced by cecal distension (to prevent further emptying when cecum is full)
- Mediated by local reflexes and sympathetic innervation
> **CLINICAL: Ileus (Paralytic Ileus)**
> - Temporary cessation of intestinal motility without mechanical obstruction
> - Common after abdominal surgery (post-operative ileus), due to handling of bowel, anesthesia, opioid use
> - Also caused by: peritonitis, electrolyte abnormalities (hypokalemia!), retroperitoneal hemorrhage
> - Presents with abdominal distension, absence of bowel sounds, inability to pass gas or stool
> - Imaging: Diffusely dilated loops of bowel with air-fluid levels
> - Management: NPO, NG tube decompression, IV fluids, correction of electrolytes, minimize opioids
> - Alvimopan (peripheral μ-opioid antagonist) can accelerate recovery of GI motility after surgery
### Colonic Motility
**Functions of colonic motility:**
1. **Mixing and absorption**: Haustral contractions mix contents, facilitating water/electrolyte absorption (absorbs ~1.5 L/day)
2. **Storage**: Especially in the transverse and descending colon
3. **Propulsion**: Mass movements propel contents toward the rectum
**Patterns:**
1. **Haustral contractions** (segmentation-like): Predominant; slow; facilitate absorption
2. **Mass movements**: 1-3 times daily; powerful; propulsive; triggered by meals (gastrocolic and duodenocolic reflexes)
3. **Retrograde contractions**: In the proximal colon; slow transit further to maximize absorption
**Transit time in colon**: 12-36 hours (can be up to 48-72 hours)
**Gastrocolic Reflex:**
- Eating a meal → distension of stomach → increased colonic motility
- Mediated by:
- Neural: Extrinsic parasympathetic pathways
- Hormonal: Gastrin, CCK
- This is why many people feel the urge to defecate after meals (especially breakfast)
> **CLINICAL: Ogilvie's Syndrome (Acute Colonic Pseudo-obstruction)**
> - Massive dilation of the colon without mechanical obstruction
> - Typically occurs in hospitalized, debilitated patients (post-surgical, ICU, electrolyte disorders)
> - Due to imbalance between sympathetic and parasympathetic tone
> - Risk of cecal perforation if diameter >12 cm
> - Treatment: Neostigmine (acetylcholinesterase inhibitor – enhances parasympathetic tone), colonoscopic decompression
### Defecation
**Anatomy:**
- **Internal anal sphincter (IAS)**: Smooth muscle; tonically contracted; involuntary; controlled by ANS
- **External anal sphincter (EAS)**: Skeletal muscle (striated); voluntary control; innervated by **pudendal nerve (S2-S4)**
- **Puborectalis muscle**: Creates the anorectal angle (~90°); maintains continence; relaxes during defecation
**Defecation Reflex:**
1. Mass movement propels feces into the rectum
2. Rectal distension stimulates **stretch receptors** in the rectal wall
3. **Intrinsic reflex**: Via myenteric plexus → increased peristalsis in sigmoid and rectum
4. **Parasympathetic reflex** (spinal reflex center at **S2-S4**):
- Afferents via pelvic nerves → spinal cord → efferents via pelvic nerves
- Increases peristalsis in descending colon, sigmoid, and rectum
- **Relaxes the internal anal sphincter** (rectoanal inhibitory reflex, RAIR)
5. The **rectoanal inhibitory reflex (RAIR)**: Rectal distension → IAS relaxation; this is mediated by **intrinsic inhibitory neurons releasing NO and VIP**
6. **Sampling reflex**: Small amount of rectal contents contacts the highly sensitive anoderm in the anal canal → distinguishes between solid, liquid, and gas
7. If defecation is appropriate:
- Voluntary relaxation of EAS and puborectalis (via pudendal nerve inhibition)
- Squatting position straightens the anorectal angle
- **Valsalva maneuver**: Increased intra-abdominal pressure (contraction of diaphragm and abdominal muscles)
- Feces expelled
8. If defecation is NOT appropriate:
- Voluntary contraction of EAS
- Rectum accommodates the feces (compliance increases)
- Urge temporarily subsides (rectal accommodation)
> **CLINICAL: Hirschsprung's Disease – Revisited**
> - The RAIR is **absent** in Hirschsprung's disease (because it requires intrinsic inhibitory neurons)
> - Anorectal manometry showing absent RAIR is a useful diagnostic test
> - Contrast this with **functional constipation** where RAIR is present
> **CLINICAL: Fecal Incontinence**
> - Can be due to:
> - **IAS dysfunction**: Passive incontinence (seepage without awareness)
> - **EAS/pudendal nerve damage**: Urge incontinence (aware but cannot hold)
> - **Rectal sensory impairment**: Overflow incontinence
> - Common causes: Obstetric injury (most common in women), surgical damage, neurological diseases, aging, rectal prolapse
> - Diagnosis: Anorectal manometry, endoanal ultrasound, pudendal nerve terminal motor latency (PNTML)
> **CLINICAL: Spinal Cord Injury and Defecation**
> - **Lesion above S2-S4** (upper motor neuron lesion):
> - Loss of voluntary control of EAS
> - Intrinsic reflex and spinal reflex intact
> - Reflex defecation can occur (digital stimulation triggers it)
> - "Reflexic bowel"
> - **Lesion at or below S2-S4** (lower motor neuron lesion) or **cauda equina**:
> - Loss of both voluntary and reflex control
> - Denervation of IAS and EAS
> - "Areflexic bowel" – requires manual evacuation
---
# PART 3: NERVOUS CONTROL OF THE GI TRACT
The GI tract has the most extensive nervous system outside the CNS. The system has three components:
## A. Enteric Nervous System (ENS) – "The Little Brain" / "Second Brain"
### General Features
- Contains approximately **100 million neurons** (as many as in the spinal cord!)
- Can function **independently** of the CNS (unique among organ systems)
- Even if all extrinsic nerves are cut, the gut can still perform peristalsis, segmentation, and secretion
- However, extrinsic nerves modulate ENS activity
### Two Major Plexuses
#### 1. Myenteric Plexus (Auerbach's Plexus)
- **Location**: Between the outer longitudinal and inner circular muscle layers
- **Primary function**: Controls **motility** (motor function)
- Extends the entire length of the GI tract
- When stimulated, its effects include:
- Increased tonic contraction ("tone") of gut wall
- Increased intensity of rhythmic contractions
- Slightly increased rate of contractions
- Increased velocity of peristaltic waves
- Contains both **excitatory and inhibitory neurons**:
- Excitatory: Release **ACh** and **Substance P**
- Inhibitory: Release **VIP**, **NO**, and **ATP** → responsible for receptive relaxation and sphincter relaxation
#### 2. Submucosal Plexus (Meissner's Plexus)
- **Location**: In the submucosa
- **Primary function**: Controls **secretion** and local **blood flow**
- Also detects the environment within the lumen (via sensory neurons)
- Regulates absorptive function of the epithelium
- Most prominent in the small intestine
- Controls the muscularis mucosae → local mucosal folding
### Types of Neurons in the ENS
**1. Intrinsic Primary Afferent Neurons (IPANs) – Sensory neurons**
- Detect mechanical stimuli (stretch, distension) and chemical stimuli (pH, osmolarity, specific nutrients)
- Their cell bodies are within the plexuses
- They initiate local reflexes
- Receptors include:
- Mechanoreceptors
- Chemoreceptors
- Thermoreceptors
- Nociceptors
**2. Interneurons**
- Connect sensory and motor neurons within and between plexuses
- Form chains for propagation of reflexes along the gut
- Ascending interneurons (oral direction) → excitatory; transmitters: ACh, Substance P
- Descending interneurons (aboral direction) → inhibitory; transmitters: NO, VIP, Somatostatin
**3. Motor Neurons**
- **Excitatory motor neurons** → smooth muscle and secretory cells
- ACh, Substance P, Serotonin
- **Inhibitory motor neurons** → smooth muscle
- NO, VIP, ATP
- **Secretomotor neurons** → glands and epithelial cells
- ACh, VIP
### Neurotransmitters and Neuromodulators of the ENS
| Transmitter | Primary Action |
|---|---|
| Acetylcholine (ACh) | Excitatory – contraction, secretion |
| Substance P | Excitatory – contraction, secretion |
| Serotonin (5-HT) | Excitatory – peristalsis initiation, secretion |
| Nitric Oxide (NO) | Inhibitory – relaxation (sphincters, receptive relaxation) |
| VIP | Inhibitory – relaxation, vasodilation, secretion |
| ATP | Inhibitory – fast inhibitory junction potential |
| CGRP | Sensory – vasodilation |
| Enkephalins/Endorphins | Inhibitory – decrease motility, decrease secretion |
| GRP (Gastrin-releasing peptide) | Stimulates gastrin release |
| Neuropeptide Y (NPY) | Inhibitory – vasoconstriction, decreased secretion |
| Galanin | Inhibitory |
| Somatostatin | Inhibitory – decreases motility and secretion |
| GABA | Modulatory |
| Dopamine | Inhibitory – decreases motility |
> **CLINICAL: Carcinoid Syndrome**
> - Carcinoid tumors (neuroendocrine tumors) produce excessive **serotonin (5-HT)** and other vasoactive substances
> - When metastatic to the liver (bypasses hepatic metabolism), causes:
> - Flushing, diarrhea (due to increased GI motility and secretion from 5-HT), bronchoconstriction, right-sided heart valve disease (carcinoid heart disease)
> - Diagnosis: Elevated urinary 5-HIAA (5-hydroxyindoleacetic acid), elevated serum chromogranin A
> - Treatment: Somatostatin analogs (octreotide, lanreotide), surgical resection
---
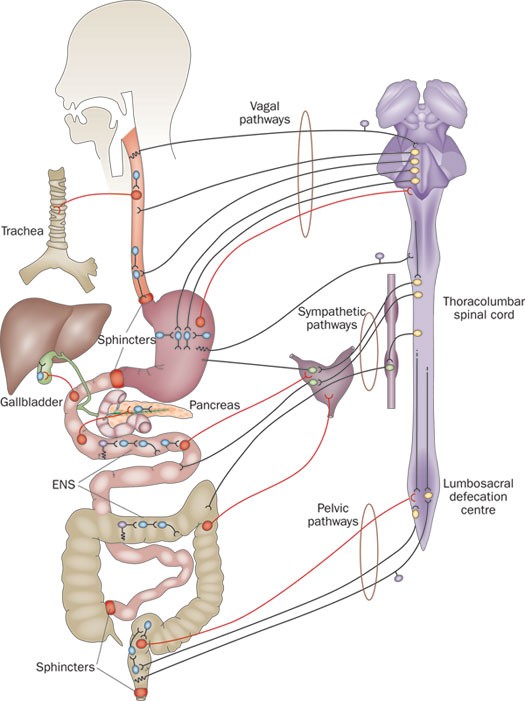
## B. Extrinsic Innervation (Autonomic Nervous System)
### 1. Parasympathetic Innervation (Generally EXCITATORY)
**Cranial division:**
- **Vagus nerve (CN X)**: Innervates the GI tract from the esophagus to the **splenic flexure** of the colon (approximately the first 2/3 of the transverse colon)
- The vagus is the most important extrinsic nerve of the GI tract
- Contains both **afferent (80%)** and efferent (20%) fibers!
- Afferents: Carry information about distension, chemical environment, nausea signals to the NTS (nucleus tractus solitarius) in the medulla
- Efferents: Preganglionic fibers synapse on neurons in the myenteric and submucosal plexuses
- Preganglionic fibers are LONG; postganglionic fibers (ENS neurons) are SHORT
- The postganglionic transmitter is **ACh** (acting on muscarinic receptors on smooth muscle, glands)
**Sacral division:**
- **Pelvic nerves (S2-S4)**: Innervate the **distal 1/3 of the transverse colon, descending colon, sigmoid, rectum, and anal canal**
- Important for the defecation reflex
**Effects of parasympathetic stimulation:**
- ↑ Motility (↑ contractions)
- ↑ Secretion
- Relaxation of sphincters (via inhibitory ENS neurons)
- ↑ Blood flow
### 2. Sympathetic Innervation (Generally INHIBITORY)
**Origin**: Thoracolumbar outflow (T5-L2)
**Pathway:**
- Preganglionic fibers (short, cholinergic) → synapse in **prevertebral ganglia**:
- **Celiac ganglion** → stomach, liver, spleen, proximal duodenum
- **Superior mesenteric ganglion** → distal duodenum, jejunum, ileum, ascending colon, proximal transverse colon
- **Inferior mesenteric ganglion** → distal transverse, descending, sigmoid colon, rectum
- **Hypogastric plexus** → rectum, internal anal sphincter
- Postganglionic fibers (long, **noradrenergic**) → ENS plexuses, smooth muscle, blood vessels
**Effects of sympathetic stimulation:**
- ↓ Motility (inhibits smooth muscle contraction, both directly and by inhibiting ENS neurons)
- **Norepinephrine** acts on:
- **α₂-adrenergic receptors** on ENS neurons → inhibits ACh release (presynaptic inhibition)
- **α₁ and β₂-adrenergic receptors** on smooth muscle → relaxation (except sphincters, which contract via α₁)
- ↓ Secretion
- **Contraction of sphincters** (α₁ receptors on sphincter smooth muscle)
- **Vasoconstriction** of GI blood vessels (α₁ receptors)
> **Summary of Autonomic Effects:**
> | | Parasympathetic | Sympathetic |
> |---|---|---|
> | Motility | ↑ | ↓ |
> | Secretion | ↑ | ↓ |
> | Sphincters | Relaxation | Contraction |
> | Blood flow | ↑ | ↓ |
> | Overall | "Rest and digest" | "Fight or flight" |
> **CLINICAL: Vagotomy – Historical Perspective**
> - Previously used for peptic ulcer disease (before PPIs and H. pylori eradication)
> - **Truncal vagotomy**: Cuts both vagal trunks → loss of receptive relaxation, loss of gastric acid secretion regulation, disrupted MMC, gastroparesis
> - Required drainage procedure (pyloroplasty or gastrojejunostomy) because of impaired gastric emptying
> - **Selective vagotomy**: Denervates only the stomach
> - **Highly selective (parietal cell) vagotomy**: Denervates only the acid-producing fundus/body; preserves antral innervation → no dumping syndrome, minimal gastroparesis
> - Post-vagotomy complications: Dumping syndrome, diarrhea, gastroparesis, gallstones (decreased gallbladder contraction)
> **CLINICAL: Diabetic Autonomic Neuropathy**
> - Affects both parasympathetic and sympathetic nerves
> - GI manifestations:
> - **Gastroparesis** (most common GI complication)
> - Esophageal dysmotility
> - Constipation (most common GI symptom) or diarrhea
> - Fecal incontinence
> - Small intestinal bacterial overgrowth
> - Gallbladder atony → gallstones
---
## C. GI Reflexes
### 1. Long Reflexes (Vagovagal Reflexes)
- **Pathway**: GI afferents → vagus nerve → NTS in medulla → dorsal motor nucleus of vagus (DMV) → vagal efferents → ENS → effector
- Examples:
- **Cephalic phase of gastric secretion**: Sight, smell, taste of food → vagal stimulation → ↑ gastric secretion
- **Receptive relaxation** of the stomach: Swallowing → vagal inhibitory fibers → fundal relaxation
- **Gastrocolic reflex**: Gastric distension → vagus → sacral parasympathetics → ↑ colonic motility
- **Vomiting reflex**: Coordinated by vomiting center in medulla
### 2. Short Reflexes (ENS Reflexes)
- Entirely within the ENS; do not require CNS involvement
- Examples:
- **Peristaltic reflex** (myenteric reflex/law of the intestine): Described above
- **Intestino-intestinal reflex**: Distension of one segment → relaxation of rest of intestine (protective; prevents further filling)
- **Rectoanal inhibitory reflex (RAIR)**: Rectal distension → IAS relaxation
- Local secretory reflexes: Mucosal stimulation → local secretion
### 3. Reflexes from GI to Other Organs
- **GI to peritoneum**: Peritoneal irritation → reflex inhibition of GI motility (paralytic ileus from peritonitis)
- **Renointestinal reflex**: Renal inflammation → intestinal inhibition
- **Vesicointestinal reflex**: Bladder distension → intestinal inhibition
> **CLINICAL: The Vomiting Reflex (Emesis)**
>
> **Vomiting center**: Located in the lateral reticular formation of the medulla
> - NOT a single discrete nucleus but a network
> - Coordinates the complex motor act of vomiting
>
> **Inputs to the vomiting center:**
> 1. **Chemoreceptor Trigger Zone (CTZ)**: Area postrema in the floor of the 4th ventricle
> - OUTSIDE the blood-brain barrier → detects toxins in blood and CSF
> - Rich in **D₂ (dopamine), 5-HT₃ (serotonin), NK₁ (substance P/neurokinin), opioid** receptors
> - Stimulated by drugs (opioids, chemotherapy, digoxin), uremia, ketoacidosis
> 2. **Vagal afferents from GI tract**: Distension, inflammation, toxins
> - 5-HT₃ receptors on vagal afferents (enterochromaffin cells release 5-HT → vagal afferents)
> 3. **Vestibular system**: Motion sickness (via H₁ and muscarinic receptors)
> 4. **Higher cortical centers**: Emotional stimuli, pain, sight/smell
>
> **Motor act of vomiting:**
> 1. Retroperistalsis in small intestine
> 2. Relaxation of stomach, LES, and esophagus
> 3. Closure of glottis (airway protection)
> 4. Elevation of soft palate (closes nasopharynx)
> 5. Forceful contraction of diaphragm and abdominal muscles → ↑ intra-abdominal pressure
> 6. Ejection of gastric contents
>
> **Antiemetic drugs (classified by receptor):**
> - **5-HT₃ antagonists**: Ondansetron, granisetron – best for chemotherapy-induced nausea
> - **D₂ antagonists**: Metoclopramide, prochlorperazine, droperidol
> - **NK₁ antagonists**: Aprepitant – for delayed chemotherapy-induced nausea
> - **H₁ antagonists**: Meclizine, dimenhydrinate – for motion sickness
> - **Anticholinergics (muscarinic)**: Scopolamine – for motion sickness
> - **Cannabinoids**: Dronabinol – for chemotherapy-induced nausea
> - **Corticosteroids**: Dexamethasone – mechanism unclear, enhances other antiemetics
>
> **CLINICAL: Cyclic Vomiting Syndrome**
> - Recurrent stereotypical episodes of severe nausea and vomiting
> - Related to migraine; associated with mitochondrial dysfunction
> - Treatment: Tricyclic antidepressants (prophylaxis), triptans (acute)
---
## D. Role of Serotonin (5-HT) in GI Physiology
- **95% of body's serotonin** is in the GI tract
- Produced by **enterochromaffin (EC) cells** in the GI mucosa (the largest endocrine organ by cell number)
- EC cells are "taste cells of the gut" – they sense luminal contents (nutrients, pH, distension) and release 5-HT
**Actions of 5-HT in the gut:**
1. Activates **5-HT₃ receptors** on vagal afferents → signals to CNS (nausea, satiety, pain)
2. Activates **5-HT₄ receptors** on ENS neurons → enhances peristalsis, increases secretion
3. Activates **5-HT₃ receptors** on ENS neurons → fast excitatory transmission
4. Activates **5-HT₁P receptors** on IPANs → initiates peristaltic reflex
**Clinical significance of 5-HT receptors:**
- **5-HT₃ antagonists** (ondansetron): Anti-emetic and can cause constipation
- **5-HT₄ agonists** (tegaserod, prucalopride): Prokinetic, used in constipation-predominant IBS and chronic constipation
- **5-HT₃ antagonists** (alosetron): Used in severe diarrhea-predominant IBS (slows motility)
> **CLINICAL: Serotonin Syndrome vs. GI Effects**
> - Excess serotonergic activity (SSRIs, MAOIs, linezolid combinations) can cause GI symptoms (diarrhea, nausea) along with mental status changes, hyperthermia, and neuromuscular hyperactivity
---
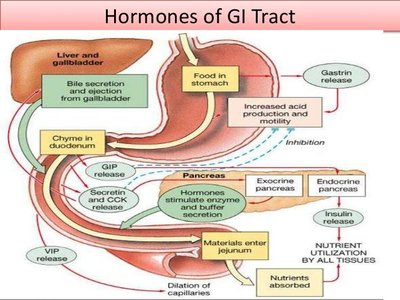
# PART 4: HORMONAL CONTROL OF THE GI TRACT
## A. Overview of GI Hormones
The GI tract is the **largest endocrine organ** in the body. GI hormones are peptides secreted by enteroendocrine cells scattered throughout the GI mucosa (the diffuse neuroendocrine system, DNES, or APUD cells – Amine Precursor Uptake and Decarboxylation).
**Modes of signaling:**
1. **Endocrine**: Hormone released into blood → acts on distant target (classic hormone)
2. **Paracrine**: Released locally → acts on neighboring cells (e.g., somatostatin, histamine)
3. **Neurocrine**: Released from nerve endings as neurotransmitters (e.g., GRP, VIP, NO)
4. **Autocrine**: Acts on the cell that produced it
5. **Luminal (Luminocrine)**: Secreted into the gut lumen (e.g., trefoil factors)
### Major GI Hormone Families
**1. Gastrin-CCK Family**
- Share the same C-terminal pentapeptide sequence (Gly-Trp-Met-Asp-Phe-NH₂)
- Both act through CCK-B (gastrin) receptor or CCK-A receptor
**2. Secretin Family (Secretin-Glucagon Family)**
- Secretin, glucagon, GIP, VIP, GLP-1, GLP-2
- Share structural homology
- All are single-chain peptides
**3. Others**: Motilin, ghrelin, somatostatin, substance P, neurotensin, PYY, etc.
---
## B. Individual Hormones – Detailed
### 1. GASTRIN
**Source**: **G cells** in the antrum of the stomach (also some in duodenum)
**Forms**:
- **G-34** (big gastrin): 34 amino acids; predominant fasting form; longer half-life
- **G-17** (little gastrin): 17 amino acids; predominant postprandial form; most potent; shorter half-life
- **G-14** (minigastrin): 14 amino acids; less common
**Stimuli for release:**
- Peptides and amino acids in the stomach lumen (especially phenylalanine and tryptophan)
- Stomach distension (vagal and local reflexes)
- Vagal stimulation via **GRP (gastrin-releasing peptide)** – NOT ACh directly on G cells (ACh acts indirectly by inhibiting somatostatin release from D cells)
- Calcium in the lumen
- Elevated gastric pH (alkaline environment)
- Coffee, alcohol
**Inhibition of release:**
- Low gastric pH (<2) – **negative feedback** (acid stimulates D cells to release somatostatin → somatostatin inhibits G cells)
- Somatostatin (from D cells) – the most important inhibitor
- Secretin
- GIP
- VIP
- CCK (mild)
**Actions of gastrin:**
1. **Stimulates gastric acid (HCl) secretion** – primary action
- Directly: Acts on CCK-B receptors on parietal cells
- Indirectly: Stimulates ECL (enterochromaffin-like) cells to release histamine → histamine acts on H₂ receptors on parietal cells (this is the more important pathway!)
2. **Stimulates pepsinogen secretion** from chief cells
3. **Trophic effect** on gastric mucosa – promotes growth of gastric oxyntic mucosa
- This is why chronic hypergastrinemia causes **mucosal hypertrophy** and **ECL cell hyperplasia**
4. **Stimulates gastric motility** – enhances antral contractions
5. **Contracts the LES** (prevents reflux)
6. **Relaxes the pyloric sphincter** (at physiological levels, promotes emptying; at pharmacological levels, contracts it)
7. Stimulates secretion of insulin (weakly), pancreatic enzymes (weakly)
8. Stimulates gallbladder contraction (weakly)
> **CLINICAL: Zollinger-Ellison Syndrome (Gastrinoma)**
> - Gastrin-secreting tumor (gastrinoma), usually in the pancreas (most common) or duodenum
> - Part of the "gastrinoma triangle" (junction of cystic duct/CBD, junction of 2nd-3rd part of duodenum, junction of neck-body of pancreas)
> - Massive gastric acid hypersecretion
> - Features: Severe peptic ulcers (often multiple, distal, atypical locations – jejunal ulcers), diarrhea (acid inactivates pancreatic enzymes, damages mucosa), steatorrhea
> - Serum gastrin levels markedly elevated (>1000 pg/mL strongly suggestive)
> - **Secretin stimulation test**: In normal individuals, secretin inhibits gastrin. In gastrinoma, paradoxical INCREASE in gastrin (>200 pg/mL increase) after IV secretin
> - 25% associated with **MEN1** (Multiple Endocrine Neoplasia type 1: parathyroid adenoma, pituitary adenoma, pancreatic islet tumors – "3 P's")
> - Treatment: High-dose PPIs, surgical resection if localized
> **CLINICAL: Hypergastrinemia – Causes and Consequences**
> - **Causes**: Zollinger-Ellison syndrome, chronic PPI use (most common cause), chronic atrophic gastritis (pernicious anemia – destruction of parietal cells → decreased acid → loss of negative feedback → G cell hyperplasia), H. pylori infection of antrum, G cell hyperplasia, retained antrum after Billroth II surgery, renal failure (decreased gastrin clearance)
> - **Consequences of chronic hypergastrinemia**: ECL cell hyperplasia → risk of gastric carcinoid tumors (especially in pernicious anemia); mucosal hypertrophy
> - This is a reason for concern about long-term PPI use
### 2. CHOLECYSTOKININ (CCK)
**Source**: **I cells** in the duodenum and jejunum
**Stimuli for release:**
- **Fatty acids** (especially long-chain fatty acids >12 carbons) in the duodenum (most potent stimulus)
- **Amino acids and peptides** (especially tryptophan and phenylalanine)
- Partially digested proteins (peptones)
- Released by **CCK-releasing factor** (a peptide secreted into the duodenal lumen by mucosal cells; normally degraded by trypsin – see below)
- **Monitor peptide** (from pancreas) also stimulates CCK release
**Inhibition:**
- Trypsin in the duodenum degrades the CCK-releasing factor → negative feedback
- Bile salts (mild)
- Somatostatin
**Actions of CCK:**
1. **Stimulates gallbladder contraction** – primary action (hence "cholecysto-kinin" = "gallbladder mover")
2. **Relaxes the sphincter of Oddi** → allows bile and pancreatic juice to enter the duodenum
3. **Stimulates pancreatic enzyme secretion** (via acinar cells – CCK-A receptors)
4. **Potentiates secretin's effect** on pancreatic bicarbonate secretion (synergy!)
5. **Inhibits gastric emptying** – contracts pyloric sphincter (most important negative regulator of gastric emptying)
6. **Inhibits gastric acid secretion** (at physiological levels)
7. **Trophic effect** on pancreas (promotes growth of exocrine pancreas)
8. **Satiety signal** – acts on vagal afferents and hypothalamic centers to promote satiety (anorexigenic)
9. Stimulates intestinal motility (mild)
10. Stimulates hepatic bile secretion (mild)
> The CCK-releasing factor/trypsin feedback mechanism:
> When protein enters the duodenum → CCK-releasing factor is secreted into lumen → stimulates I cells → CCK release → pancreatic enzymes (including trypsin) released → trypsin degrades CCK-releasing factor → CCK release stops
> In **chronic pancreatitis** (reduced trypsin) → unchecked CCK-releasing factor → chronic CCK hypersecretion → abdominal pain may be partly CCK-mediated
> **CLINICAL: Gallstones and CCK**
> - CCK is used diagnostically: **CCK-HIDA scan** (cholescintigraphy) – CCK analog is injected to assess gallbladder contraction
> - Gallbladder ejection fraction <35% suggests **biliary dyskinesia**
> - In patients with deficient CCK release or CCK receptor abnormalities → gallbladder stasis → predisposition to gallstone formation
### 3. SECRETIN
**Source**: **S cells** in the duodenum (and to lesser extent, jejunum)
**The first hormone ever discovered** (Bayliss and Starling, 1902) – this discovery established the concept of hormones!
**Stimuli for release:**
- **Acid (H⁺)** in the duodenum (pH <4.5) – most potent stimulus
- Fatty acids in the duodenum
- Bile salts (mild)
**Inhibition:**
- Gastric acid neutralization (pH >4.5 in duodenum → no more stimulus)
- Somatostatin
- H₂ blockers (indirectly – less acid reaching duodenum)
**Actions of secretin:**
1. **Stimulates pancreatic bicarbonate (HCO₃⁻) secretion** from ductal cells – PRIMARY ACTION
- Most important action; neutralizes duodenal acid
- Acts through cAMP pathway → activates CFTR (Cl⁻ channels) and Cl⁻/HCO₃⁻ exchangers on ductal cells
2. **Stimulates biliary bicarbonate secretion** (choleretic – increases bile volume)
3. **Inhibits gastric acid secretion** (opposes gastrin)
4. **Inhibits gastric motility** (reduces gastric emptying)
5. **Stimulates pepsinogen secretion** (mild, via vagal pathways)
6. **Trophic effect on pancreas** (ductal cells)
7. **Potentiates CCK's action** on pancreatic enzyme secretion
> **CLINICAL: Secretin Stimulation Test**
> - Used to diagnose Zollinger-Ellison syndrome (gastrinoma)
> - In normal patients, IV secretin → no change or decrease in serum gastrin
> - In gastrinoma, IV secretin → paradoxical increase in gastrin (>200 pg/mL)
> - Because secretin acts directly on gastrinoma cells via secretin receptors that are aberrantly coupled to gastrin release
> - Also used to assess **pancreatic exocrine function**: Secretin IV → collect duodenal aspirate → measure HCO₃⁻ output (decreased in chronic pancreatitis)
> **CLINICAL: Cystic Fibrosis**
> - CFTR mutation → defective Cl⁻ and HCO₃⁻ secretion by pancreatic ductal cells
> - Secretin cannot stimulate adequate HCO₃⁻ secretion
> - Thick, viscous pancreatic secretions → duct obstruction → pancreatitis → pancreatic insufficiency
> - Leads to malabsorption, steatorrhea, fat-soluble vitamin deficiency (A, D, E, K)
### 4. GLUCOSE-DEPENDENT INSULINOTROPIC PEPTIDE (GIP)
(Previously called Gastric Inhibitory Peptide)
**Source**: **K cells** in the duodenum and jejunum
**Stimuli for release:**
- Glucose and other sugars (most potent)
- Fatty acids
- Amino acids
- All nutrients in the duodenum stimulate GIP
**Actions of GIP:**
1. **Stimulates insulin secretion** from pancreatic β-cells – PRIMARY ACTION (incretin effect)
- This is why oral glucose causes a greater insulin response than the same amount of IV glucose ("incretin effect")
- GIP acts on GIP receptors (GPCRs) on β-cells → cAMP → enhanced glucose-stimulated insulin secretion
- The effect is GLUCOSE-DEPENDENT – works only when blood glucose is elevated (safety mechanism against hypoglycemia)
2. **Inhibits gastric acid secretion** (pharmacological doses; questionable at physiological levels)
3. **Inhibits gastric motility** (mild, at high doses)
4. Stimulates lipoprotein lipase → fatty acid uptake into adipocytes
5. Stimulates osteoblast activity (emerging role in bone metabolism)
> **CLINICAL: Incretin-Based Therapies for Type 2 Diabetes**
> - The incretin effect accounts for 50-70% of the postprandial insulin response
> - Two main incretins: GIP and GLP-1
> - In Type 2 DM, the incretin effect is diminished
> - **GLP-1 receptor agonists** (exenatide, liraglutide, semaglutide): Mimic GLP-1; enhance insulin secretion, suppress glucagon, delay gastric emptying, promote satiety → weight loss
> - **DPP-4 inhibitors** (sitagliptin, saxagliptin): Inhibit dipeptidyl peptidase-4, which degrades GIP and GLP-1 → prolong incretin action; weight-neutral
### 5. GLP-1 (Glucagon-Like Peptide-1)
**Source**: **L cells** in the ileum and colon (distal gut)
**Stimuli:** Nutrients in the distal small intestine and colon (carbohydrates, fats, proteins)
**Actions:**
1. **Incretin effect** – stimulates glucose-dependent insulin secretion (more potent than GIP)
2. **Inhibits glucagon secretion** from α-cells
3. **Delays gastric emptying** (significant effect – contributes to postprandial glucose lowering)
4. **Promotes satiety** (acts on hypothalamic centers via vagal afferents)
5. **Trophic effect on β-cells** (promotes β-cell proliferation, inhibits apoptosis)
6. Possible cardioprotective effects
**Degradation**: Rapidly degraded by **DPP-4** (half-life ~2 minutes)
> **CLINICAL: GLP-1 Receptor Agonists (Semaglutide, Liraglutide)**
> - Major role in Type 2 DM and obesity
> - Semaglutide (Ozempic/Wegovy) has gained enormous attention for weight loss
> - Side effects include nausea, vomiting, diarrhea (due to delayed gastric emptying), pancreatitis risk (controversial), potential thyroid C-cell tumor risk (seen in rodents, contraindicated in MEN2 and medullary thyroid cancer)
> - GLP-1 RAs have shown cardiovascular benefit (reduced MACE events in LEADER, SUSTAIN-6, REWIND trials)
### 6. GLP-2 (Glucagon-Like Peptide-2)
**Source**: L cells (co-secreted with GLP-1)
**Actions:**
- **Trophic effect on intestinal mucosa** – stimulates mucosal growth, increases villous height, increases absorptive capacity
- Inhibits gastric acid secretion
- Enhances intestinal blood flow
- Reduces intestinal permeability
> **CLINICAL: Teduglutide**
> - GLP-2 analog used for **Short Bowel Syndrome** (SBS)
> - Promotes intestinal adaptation → increases absorption → reduces parenteral nutrition requirements
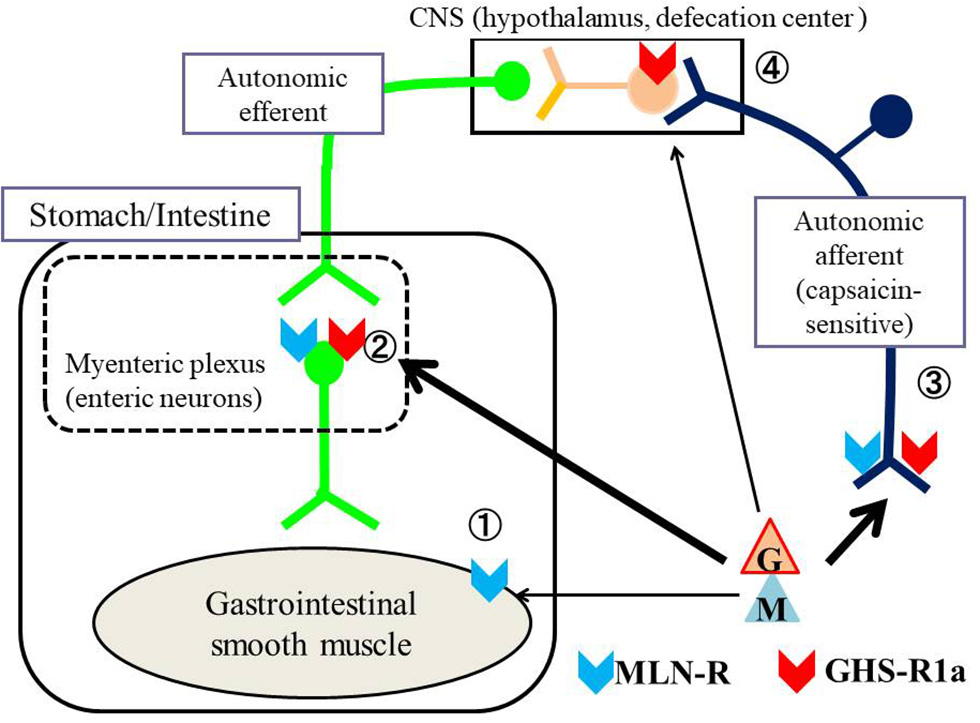
### 7. MOTILIN
**Source**: **Mo cells** (M cells) in the duodenum and jejunum
**Stimuli:** Cyclical release during fasting (every 90-120 minutes); alkaline pH; fat
**Actions:**
1. **Initiates Phase III of the Migrating Motor Complex (MMC)** – PRIMARY ACTION
2. Increases gastric motility and gastric emptying
3. Increases LES pressure
**Important note**: Motilin release is **ABOLISHED by feeding** (and MMC ceases)
**Erythromycin** acts as a **motilin receptor agonist** → this is why it's used as a prokinetic agent
> **CLINICAL: Erythromycin as a Prokinetic**
> - Low-dose erythromycin (40-250 mg) IV or oral acts as a motilin agonist
> - Used for diabetic gastroparesis and acute gastroparesis
> - Tolerance develops with chronic use (receptor desensitization)
> - Must be aware of drug interactions (CYP3A4 inhibition) and QT prolongation risk
### 8. SOMATOSTATIN
**Source**: **D cells** throughout the GI tract (especially antrum and fundus), pancreatic δ cells, hypothalamus
**Stimuli:** Acid in the lumen, fat, amino acids, bile acids
**It is the UNIVERSAL INHIBITOR of the GI tract!**
**Actions of somatostatin (all inhibitory):**
1. Inhibits gastrin release from G cells (paracrine in antrum)
2. Inhibits acid secretion from parietal cells (direct)
3. Inhibits histamine release from ECL cells
4. Inhibits pepsinogen from chief cells
5. Inhibits pancreatic enzyme and bicarbonate secretion
6. Inhibits insulin and glucagon release from pancreas
7. Inhibits GH, TSH from anterior pituitary
8. Inhibits CCK, secretin, GIP, VIP, motilin release
9. Inhibits intestinal absorption
10. Inhibits gallbladder contraction
11. Reduces splanchnic blood flow
12. Inhibits growth/proliferation of GI mucosa and tumors
> **CLINICAL: Octreotide (Somatostatin Analog)**
> - Long-acting somatostatin analog
> - Uses:
> - **Variceal bleeding** (reduces splanchnic blood flow and portal pressure)
> - **Carcinoid syndrome** (inhibits hormone release)
> - **VIPoma** (watery diarrhea)
> - **Glucagonoma**
> - **Acromegaly** (inhibits GH)
> - **Diarrhea** (secretory diarrhea, short bowel syndrome, dumping syndrome)
> - **Pancreatic fistula** (reduces pancreatic secretion)
> - Side effects: Gallstones (inhibits gallbladder contraction), steatorrhea, hyperglycemia (inhibits insulin), bradycardia
### 9. GHRELIN
**Source**: **Gr cells (X/A-like cells)** in the fundus of the stomach (primary source), also hypothalamus
**Unique among GI hormones**: Only known **orexigenic (appetite-stimulating)** hormone from the GI tract
**Stimuli:** Fasting (levels rise before meals, fall after eating)
**Actions:**
1. **Stimulates appetite** (orexigenic) – acts on hypothalamic arcuate nucleus via **GHS-R (growth hormone secretagogue receptor)**
2. **Stimulates GH release** from anterior pituitary (original discovery function)
3. Stimulates gastric acid secretion
4. Increases gastric motility and emptying
5. Promotes adiposity (lipogenesis)
6. Possible roles in reward-seeking behavior and food hedonics
> **CLINICAL: Ghrelin and Obesity Surgery**
> - After **sleeve gastrectomy** (removal of fundus), ghrelin levels drop dramatically (because the source is removed) → contributes to appetite suppression and weight loss
> - After **Roux-en-Y gastric bypass**, ghrelin levels may also decrease (blunted postprandial response)
> - Ghrelin antagonists are being explored as anti-obesity drugs
>
> **CLINICAL: Prader-Willi Syndrome**
> - Genetic disorder with markedly elevated ghrelin levels → insatiable appetite → severe obesity
> - Deletion on chromosome 15q11-q13 (paternal)
### 10. VASOACTIVE INTESTINAL PEPTIDE (VIP)
**Source**: Neurons throughout the ENS (it's primarily a neurocrine, not a classic hormone)
**Actions:**
1. **Relaxes smooth muscle** – especially sphincters (LES, pylorus, ileocecal valve, internal anal sphincter)
2. **Stimulates intestinal and pancreatic secretion** (water and electrolytes)
3. **Vasodilation** of GI blood vessels (increases blood flow)
4. **Inhibits gastric acid secretion**
5. Stimulates hepatic bile flow
> **CLINICAL: VIPoma (Verner-Morrison Syndrome / WDHA Syndrome)**
> - VIP-secreting tumor (usually pancreatic islet cell tumor)
> - WDHA: **Watery Diarrhea, Hypokalemia, Achlorhydria** (also called "pancreatic cholera")
> - Massive secretory diarrhea (>3 L/day), flushing, metabolic acidosis (loss of HCO₃⁻ in stool)
> - Diagnosis: Elevated serum VIP
> - Treatment: Octreotide (inhibits VIP release), surgical resection
### 11. PEPTIDE YY (PYY)
**Source**: **L cells** in the ileum and colon (co-released with GLP-1)
**Form**: PYY₃₋₃₆ is the active circulating form
**Stimuli:** Fat and bile acids in the distal ileum/colon
**Actions:**
1. **"Ileal brake"** – inhibits gastric emptying, gastric acid secretion, pancreatic secretion, and upper GI motility when nutrients reach the distal gut
2. **Satiety signal** – reduces appetite (acts on Y₂ receptors in hypothalamus)
3. Inhibits intestinal secretion (promotes absorption)
> The "ileal brake" is an important negative feedback mechanism: When unabsorbed nutrients reach the ileum → PYY and GLP-1 are released → slow down upper GI transit → allow more time for absorption
### 12. SUBSTANCE P
**Source**: Neurons in the ENS and CNS
**Actions:**
- Excitatory neurotransmitter → increases smooth muscle contraction
- Stimulates salivary secretion
- Involved in pain transmission (nociception)
- Promotes inflammation and immune cell activation in the gut
- Acts on NK₁ receptors
> **CLINICAL: NK₁ Receptor Antagonists**
> - Aprepitant: NK₁ antagonist used as an antiemetic for chemotherapy-induced nausea (targets substance P pathway)
### 13. GASTRIN-RELEASING PEPTIDE (GRP)
**Source**: Vagal nerve endings in the gastric wall (neurocrine)
**Actions:**
- Stimulates gastrin release from G cells (this is how the vagus stimulates gastrin)
- GRP is the mammalian equivalent of **bombesin** (amphibian peptide)
> Important: Atropine (muscarinic blocker) does NOT block vagally stimulated gastrin release because vagal fibers use GRP, not ACh, to stimulate G cells
> However, atropine DOES block vagal stimulation of parietal cells (direct cholinergic pathway)
### 14. NEUROTENSIN
**Source**: N cells in the ileum
**Stimuli**: Fatty acids
**Actions**: Inhibits GI motility, stimulates pancreatic secretion, vasodilation, histamine release from mast cells
---
### Summary Table of Major GI Hormones
| Hormone | Cell | Location | Primary Stimulus | Primary Action |
|---|---|---|---|---|
| Gastrin | G cells | Antrum | Peptides, distension, vagal (GRP) | ↑ Acid secretion |
| CCK | I cells | Duodenum/Jejunum | Fat, amino acids | GB contraction, ↑ pancreatic enzymes |
| Secretin | S cells | Duodenum | Acid (pH <4.5) | ↑ Pancreatic HCO₃⁻ |
| GIP | K cells | Duodenum/Jejunum | Glucose, fat, amino acids | ↑ Insulin (incretin) |
| GLP-1 | L cells | Ileum/Colon | Nutrients | ↑ Insulin (incretin), satiety |
| Motilin | Mo cells | Duodenum/Jejunum | Cyclical (fasting) | Initiates MMC Phase III |
| Somatostatin | D cells | Throughout GI + pancreas | Acid, fat | Universal inhibitor |
| Ghrelin | Gr cells | Fundus | Fasting | ↑ Appetite, ↑ GH |
| VIP | ENS neurons | Throughout GI | Nerve stimulation | Smooth muscle relaxation, ↑ secretion |
| PYY | L cells | Ileum/Colon | Fat, bile acids | Ileal brake, satiety |
---
### Candidate Hormones and Other Regulatory Peptides
These are substances with hormonal actions but whose complete hormonal status has not been fully established:
- **Guanylin and uroguanylin**: Secreted by intestinal epithelial cells; activate guanylyl cyclase C → ↑ cGMP → Cl⁻ and water secretion → fluid secretion into lumen
> **CLINICAL: Linaclotide and Plecanatide**
> - Guanylyl cyclase C agonists
> - Used for chronic idiopathic constipation and IBS-C
> - Mimic guanylin → increase intestinal fluid secretion → relieve constipation
> - Also have visceral analgesic effects (reduce pain in IBS)
> **CLINICAL: E. coli Heat-Stable Enterotoxin (STa)**
> - The mechanism of traveler's diarrhea (ETEC)
> - STa activates guanylyl cyclase C → excessive cGMP → massive Cl⁻ and water secretion → secretory diarrhea
---
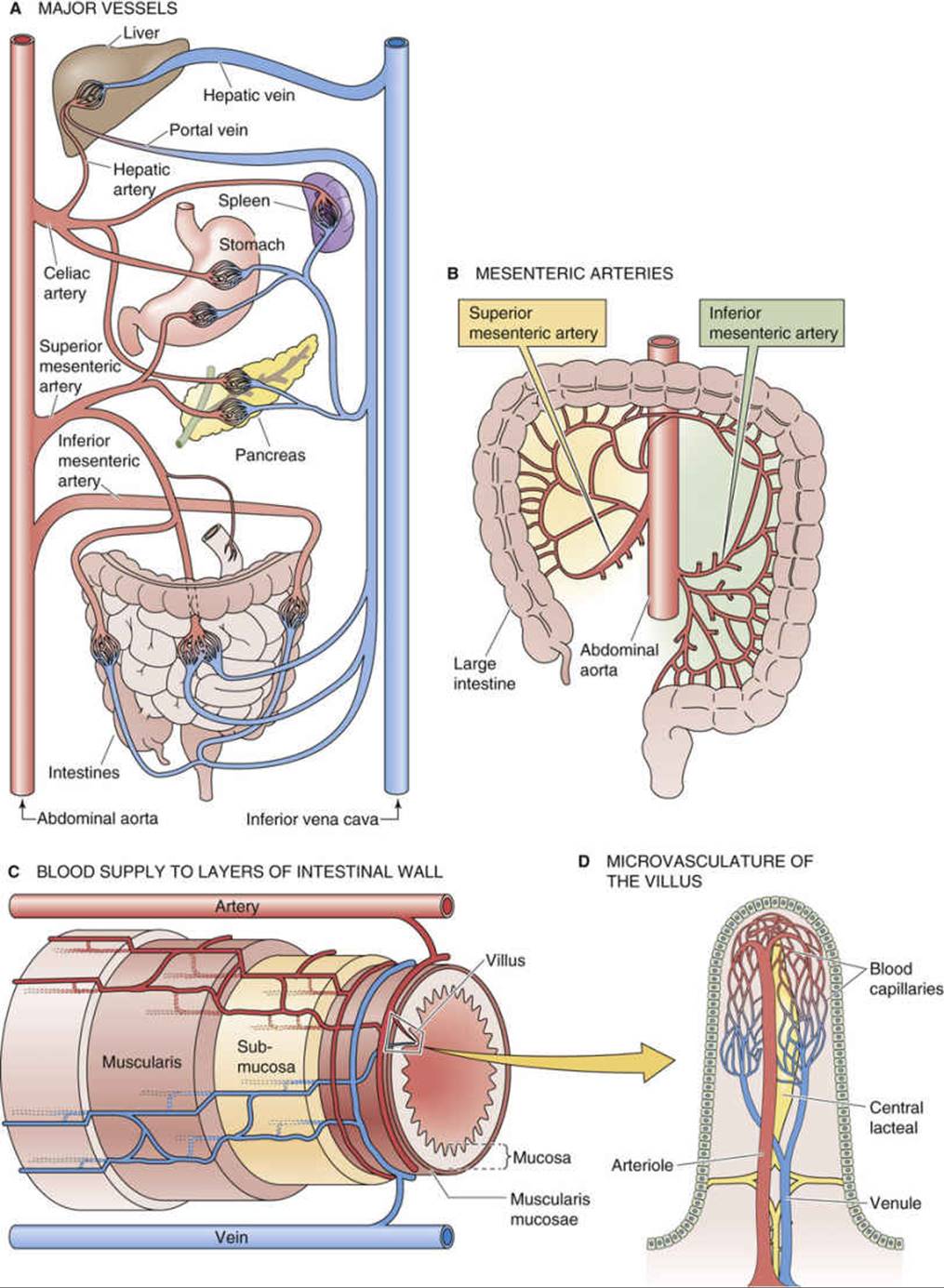
# PART 5: GASTROINTESTINAL BLOOD CIRCULATION (SPLANCHNIC CIRCULATION)
## A. Overview and Anatomy
The GI tract receives approximately **25-30% of cardiac output** at rest, making it the largest regional vascular bed in the body. After a meal, this can increase to up to **35-40%** of cardiac output.
### Arterial Supply
| Region | Arterial Supply |
|---|---|
| Foregut (esophagus to mid-duodenum, liver, spleen, pancreas) | **Celiac trunk** (left gastric, splenic, common hepatic arteries) |
| Midgut (mid-duodenum to proximal 2/3 transverse colon) | **Superior mesenteric artery (SMA)** |
| Hindgut (distal 1/3 transverse colon to rectum) | **Inferior mesenteric artery (IMA)** |
### Microvascular Organization
**Countercurrent exchange mechanism in the villi:**
- Each villus has a central arteriole and venule running in close proximity
- Ascending arteriole runs parallel to descending venule
- This creates a **countercurrent exchange** system
- **O₂ can diffuse from arteriole to venule at the base of the villus** → the tip of the villus has relatively lower O₂ tension
- This makes the **villus tips vulnerable to ischemia** (watershed zone)
- At rest, villus tip PO₂ is ~20 mmHg compared to ~50-60 mmHg at the base
> **CLINICAL: Non-occlusive Mesenteric Ischemia (NOMI)**
> - In low-flow states (heart failure, shock, sepsis), the villus tips are the first to become ischemic
> - Due to the countercurrent exchange "stealing" O₂ at the base
> - Leads to mucosal necrosis starting at the villus tips → progresses deeper
> - Explains why early ischemia affects mucosa before muscularis and serosa
### Portal Venous System
- All venous blood from the GI tract (except the lower rectum) drains into the **portal vein**
- Portal vein carries nutrient-rich blood to the **liver** for processing (first-pass metabolism)
- The portal vein forms from the confluence of the **superior mesenteric vein** and **splenic vein**
- The **inferior mesenteric vein** drains into the splenic vein (usually)
- The liver receives dual blood supply: 75% from portal vein, 25% from hepatic artery
> **CLINICAL: Portal Hypertension**
> - Most commonly due to **hepatic cirrhosis** (intrahepatic, sinusoidal)
> - Normal portal pressure: 5-10 mmHg; portal HTN defined as >12 mmHg (or HVPG >5 mmHg)
> - Consequences (portosystemic shunts develop):
> 1. **Esophageal varices** (left gastric vein → esophageal veins → azygos system) – most dangerous, risk of massive hemorrhage
> 2. **Caput medusae** (paraumbilical veins → superficial epigastric veins)
> 3. **Hemorrhoids** (superior rectal vein → middle/inferior rectal veins)
> 4. **Retroperitoneal shunts**
> 5. **Splenomegaly** (congestive)
> 6. **Ascites** (increased hydrostatic pressure + decreased albumin + splanchnic vasodilation)
> 7. **Hepatic encephalopathy** (toxins bypass liver → reach brain)
---
## B. Regulation of GI Blood Flow
### 1. Intrinsic (Local) Regulation
#### a. Metabolic Autoregulation
- The most important mechanism for matching blood flow to metabolic activity
- During active absorption and secretion, metabolic rate increases → local accumulation of vasodilator metabolites:
- **Adenosine** (most important)
- CO₂
- H⁺ (decreased pH)
- K⁺
- Decreased O₂
- These cause local arteriolar vasodilation → increased blood flow
#### b. Myogenic Response (Bayliss Effect)
- Increased perfusion pressure → stretch of arteriolar smooth muscle → reflex vasoconstriction (attempts to maintain constant flow)
- Decreased pressure → vasodilation
- Helps autoregulate blood flow during changes in systemic blood pressure
- **GI autoregulation is relatively poor** compared to cerebral or renal circulation → GI blood flow is more dependent on systemic pressure
#### c. Mucosal Hyperemia (Functional Hyperemia)
- After a meal, blood flow to the GI mucosa and submucosa increases dramatically (up to 8-fold!)
- **Postprandial hyperemia** begins within minutes and lasts for hours
- Mechanisms:
- Local metabolic factors (as above)
- GI hormones: **CCK, gastrin, secretin** all increase mesenteric blood flow
- **VIP** is a potent vasodilator in the GI tract
- Parasympathetic (vagal) stimulation → VIP and NO release → vasodilation
- Products of digestion (glucose, fatty acids, amino acids) in the mucosa stimulate vasodilation
- Kinins (bradykinin, kallidin) – released during active secretion → vasodilation
> **CLINICAL: Postprandial (Intestinal) Angina**
> - Chronic mesenteric ischemia: Atherosclerotic narrowing of mesenteric arteries (usually ≥2 of 3 major vessels: celiac, SMA, IMA)
> - Postprandial abdominal pain (30 min to 1 hour after eating) – because the narrowed arteries cannot meet the increased oxygen demand during digestion
> - Food avoidance → **"food fear"** → significant weight loss
> - Abdominal bruit may be present
> - Diagnosis: CTA or MRA; mesenteric angiography (gold standard)
> - Treatment: Angioplasty/stenting or surgical revascularization
### 2. Extrinsic (Neural) Regulation
#### a. Sympathetic Innervation
- Primary extrinsic controller of GI blood flow
- Norepinephrine → **α₁-adrenergic receptors** on arteriolar smooth muscle → **vasoconstriction**
- During the "fight or flight" response, sympathetic activation diverts blood AWAY from the GI tract to skeletal muscles, heart, and brain
- **Autoregulatory escape**: During sustained sympathetic stimulation, the initial vasoconstriction is followed by a gradual return toward normal blood flow
- Mechanism: Accumulated local vasodilator metabolites override the sympathetic vasoconstriction
- This is a protective mechanism against prolonged ischemia
- However, veins do NOT show autoregulatory escape → sustained venoconstriction → increased venous return to heart
#### b. Parasympathetic Innervation
- NOT a major direct regulator of GI blood flow
- Indirectly increases blood flow by:
- Stimulating motility and secretion → increased metabolic activity → metabolic vasodilation
- Releasing VIP from nerve endings → direct vasodilation
### 3. Hormonal Regulation
| Hormone/Factor | Effect on GI Blood Flow |
|---|---|
| Gastrin | ↑ (vasodilation of gastric mucosa) |
| CCK | ↑ (vasodilation of intestinal mucosa) |
| Secretin | ↑ |
| VIP | ↑ (potent vasodilation) |
| Histamine | ↑ (vasodilation via H₂ receptors on mucosal vessels) |
| Nitric oxide (NO) | ↑ (vasodilation – important tonic vasodilator) |
| Prostaglandins (PGE₂, PGI₂) | ↑ (vasodilation, also cytoprotective) |
| Somatostatin | ↓ (vasoconstriction – used therapeutically) |
| Vasopressin (ADH) | ↓ (potent vasoconstriction – used for variceal bleeding) |
| Angiotensin II | ↓ (vasoconstriction) |
| Endothelin | ↓ (vasoconstriction) |
> **CLINICAL: NSAIDs and GI Blood Flow**
> - NSAIDs inhibit cyclooxygenase (COX) → decreased prostaglandin synthesis
> - Prostaglandins (especially PGE₂ and PGI₂) maintain mucosal blood flow, stimulate mucus and HCO₃⁻ secretion, promote mucosal cell proliferation
> - NSAID use → decreased mucosal blood flow → mucosal ischemia → peptic ulcers
> - This is why **misoprostol** (PGE₁ analog) is used to prevent NSAID-induced ulcers
> - COX-2 selective inhibitors (celecoxib) have less GI toxicity but NOT zero risk
> **CLINICAL: Acute Mesenteric Ischemia**
> - **Embolic** (50%): Usually SMA embolism from cardiac source (atrial fibrillation, MI, valvular disease)
> - **Thrombotic** (25%): Atherosclerosis of mesenteric vessels
> - **NOMI** (20%): Low cardiac output states, vasopressors, cocaine
> - **Mesenteric venous thrombosis** (5%): Hypercoagulable states, portal hypertension, malignancy
> - Presentation: Severe periumbilical abdominal pain "out of proportion to physical examination" (classic!), nausea, vomiting, bloody diarrhea later
> - Elevated lactate, metabolic acidosis, leukocytosis
> - Diagnosis: CT angiography (gold standard for initial evaluation), mesenteric angiography (diagnostic and therapeutic)
> - Treatment: Emergent surgery (embolectomy, bowel resection of necrotic segments), anticoagulation, papaverine infusion (vasodilator) for NOMI
> - High mortality (60-80% if delayed)
> **CLINICAL: Ischemic Colitis**
> - Most common form of intestinal ischemia
> - Usually affects the "watershed areas":
> - **Splenic flexure** (Griffith's point): Junction of SMA and IMA territories
> - **Rectosigmoid junction** (Sudeck's point): Junction of IMA and internal iliac artery territories
> - Typically in elderly patients with atherosclerosis or after aortic surgery
> - Presents with sudden onset crampy abdominal pain + bloody diarrhea
> - Usually transient and self-limiting (mucosal ischemia); can progress to gangrene (transmural)
> - "Thumbprinting" on CT/X-ray (submucosal edema and hemorrhage)
---
## C. The Hepatic Circulation
**Special features:**
- **Dual blood supply**: Hepatic artery (25% of blood, 50% of O₂) + Portal vein (75% of blood, 50% of O₂)
- **Hepatic arterial buffer response**: When portal flow decreases, hepatic arterial flow increases to compensate (mediated by adenosine washout mechanism)
- Normally, portal flow washes away adenosine → keeps hepatic artery somewhat constricted
- When portal flow decreases → adenosine accumulates → hepatic artery dilates
- **Low-resistance sinusoidal system**: Hepatic sinusoids are fenestrated, allowing direct contact between blood and hepatocytes
- Blood exits via hepatic veins → IVC
---
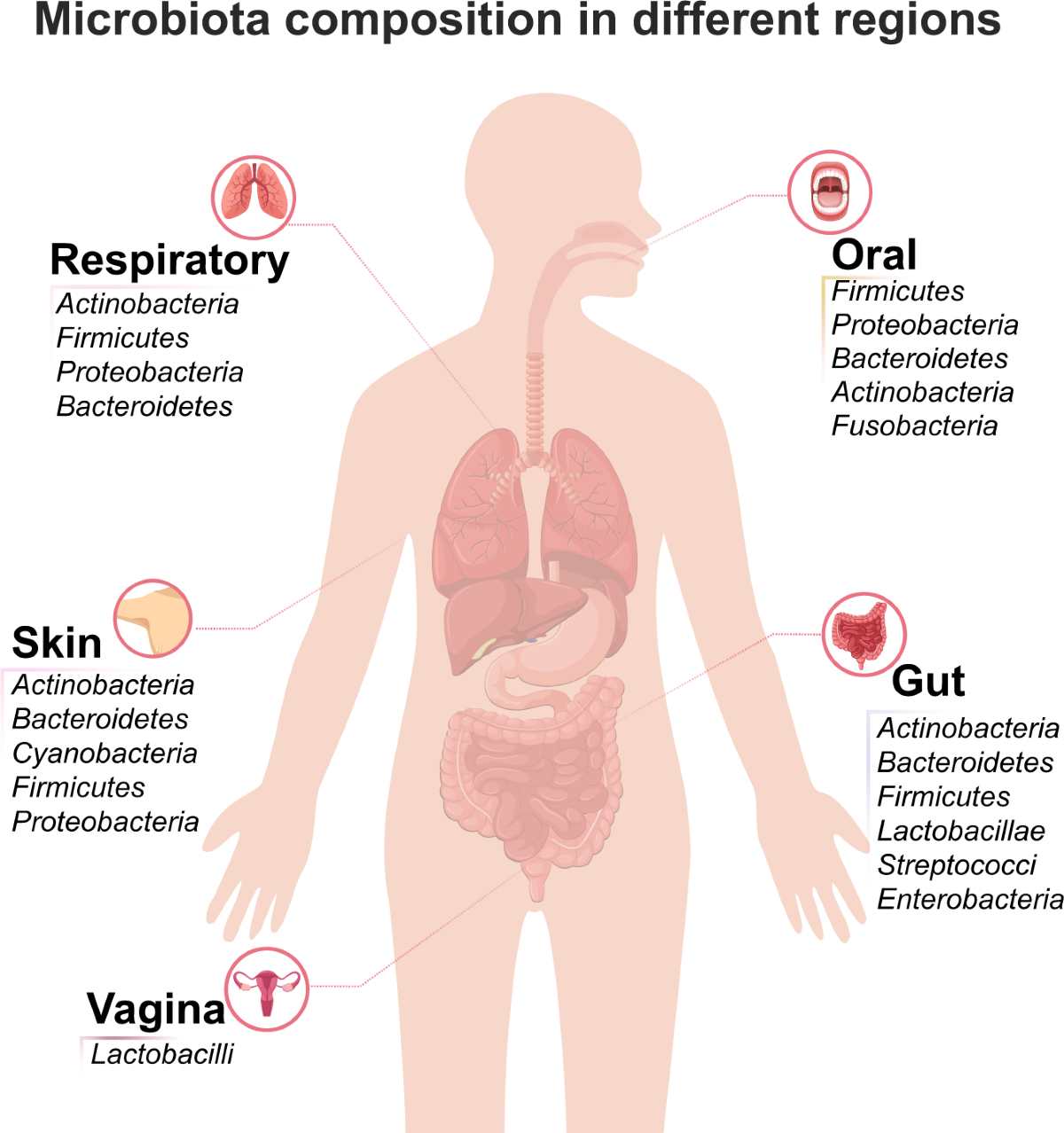
# PART 6: GASTROINTESTINAL MICROBIOTA
## A. Overview
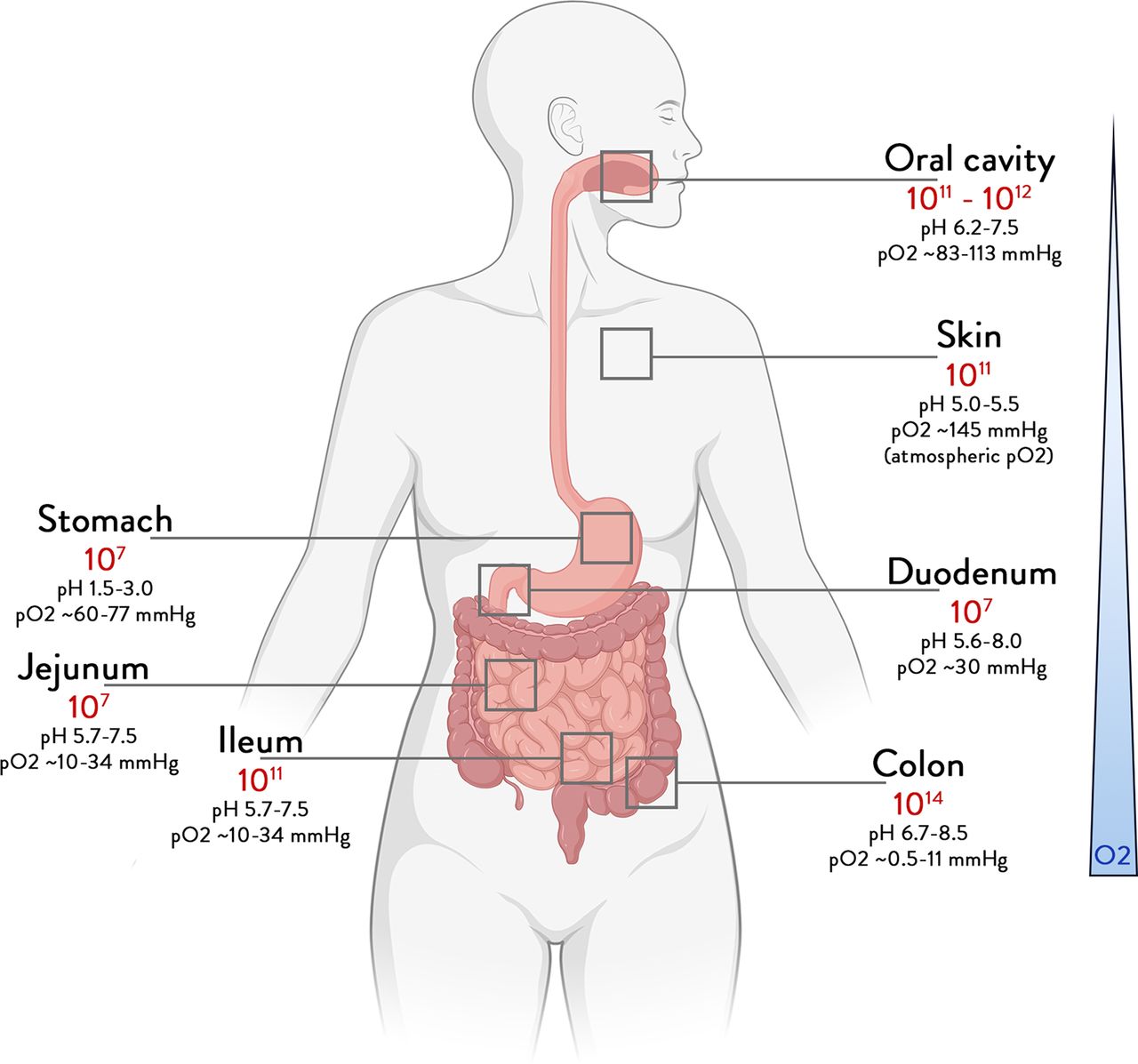
The human GI tract harbors approximately **10¹³–10¹⁴ microorganisms** (roughly equal to the number of human cells in the body). The collective genome of these microorganisms (**microbiome**) contains ~3 million genes (150× more than the human genome). This microbial ecosystem has co-evolved with humans and is essential for health.
### Terminology
- **Microbiota**: The community of living microorganisms in a particular environment
- **Microbiome**: The collective genomes of all the microorganisms
- **Dysbiosis**: An imbalance in the microbial community associated with disease
## B. Composition
### Distribution Along the GI Tract
The number and type of microorganisms vary dramatically along the GI tract:
| Region | Microbial Density (CFU/mL) | Key Factors Limiting Growth |
|---|---|---|
| Oral cavity | 10⁸–10¹⁰ | Saliva (lysozyme, IgA) |
| Stomach | 10¹–10³ | **Gastric acid** (pH 1-2 kills most bacteria) |
| Duodenum | 10¹–10³ | Acid, bile salts, rapid transit |
| Jejunum | 10³–10⁴ | Bile salts, rapid transit, MMC |
| Ileum | 10⁷–10⁸ | Transition zone; bile salts decrease |
| Colon | **10¹¹–10¹²** | **Highest density!** Slow transit, fermentable substrates, neutral pH |
**The colon is the primary site of microbial colonization**, containing >70% of all microorganisms in the body.
### Major Phyla
The gut microbiota is dominated by 4 phyla (of the ~50+ known bacterial phyla):
1. **Firmicutes** (~60-80% of gut bacteria)
- Includes: *Lactobacillus*, *Clostridium*, *Ruminococcus*, *Enterococcus*, *Staphylococcus*, *Faecalibacterium*, *Roseburia*, *Eubacterium*
- Many are Gram-positive
- Important for short-chain fatty acid (SCFA) production (especially butyrate)
2. **Bacteroidetes** (~20-30%)
- Includes: *Bacteroides*, *Prevotella*
- Gram-negative
- Important for complex carbohydrate metabolism
3. **Actinobacteria** (~3-10%)
- Includes: *Bifidobacterium*, *Collinsella*
- Some beneficial (probiotics)
4. **Proteobacteria** (~1-5%)
- Includes: *Escherichia coli*, *Klebsiella*, *Helicobacter*
- Gram-negative
- Increased abundance often associated with **dysbiosis**
5. **Verrucomicrobia** (~1-3%)
- Includes: *Akkermansia muciniphila* (mucin-degrading; associated with lean phenotype and improved metabolic health)
6. Other: **Fusobacteria**, **Euryarchaeota** (methanogens like *Methanobrevibacter smithii*)
### The Firmicutes/Bacteroidetes (F/B) Ratio
- Often cited as a marker of gut health
- **Increased F/B ratio** associated with obesity (more efficient energy extraction from food)
- **Decreased F/B ratio** may be seen in inflammatory conditions
- However, this concept is oversimplified and the clinical utility is debated
### Other Microorganisms
- **Fungi (Mycobiome)**: *Candida*, *Saccharomyces*, *Malassezia*, *Aspergillus* – typically <0.1% of gut microbiota
- **Viruses (Virome)**: Bacteriophages (viruses that infect bacteria) are the most numerous; also eukaryotic viruses
- **Archaea**: *Methanobrevibacter smithii* – produces methane; may contribute to constipation and IBS-C
- **Protozoa**: Rare in healthy individuals
## C. Development and Establishment
### Neonatal Colonization
1. **In utero**: Previously thought sterile; emerging evidence suggests limited microbial exposure via placenta and amniotic fluid (controversial)
2. **Birth**: Major colonization event
- **Vaginal delivery**: Baby colonized with maternal vaginal/fecal flora (*Lactobacillus*, *Prevotella*, *Bacteroides*, *E. coli*)
- **Cesarean delivery**: Colonized with skin/hospital flora (*Staphylococcus*, *Corynebacterium*, *Propionibacterium*) → delayed Bacteroidetes colonization
> **CLINICAL: C-section and Disease Risk**
> - C-section delivery associated with:
> - Delayed and altered microbiota establishment
> - Increased risk of asthma, allergies, atopic disease, obesity, Type 1 DM, celiac disease
> - This supports the "hygiene hypothesis" / "microbial deprivation hypothesis"
> - "Vaginal seeding" (swabbing C-section babies with vaginal fluid) is being studied but not yet standard practice
3. **Breastfeeding vs. Formula feeding**:
- **Breast milk** contains:
- **Human milk oligosaccharides (HMOs)**: >200 complex sugars that are NOT digestible by the infant but serve as **prebiotics** selectively feeding *Bifidobacterium*
- IgA, lysozyme, lactoferrin (immune factors)
- Live bacteria (including *Lactobacillus*, *Bifidobacterium*, *Staphylococcus*)
- Breastfed infants have microbiota dominated by *Bifidobacterium*
- Formula-fed infants have more diverse but less "beneficial" flora (more *Clostridium*, *Bacteroides*)
4. **Weaning and introduction of solid food**: Major diversification event; by age 2-3 years, the microbiota resembles adult composition
5. **Adult microbiota**: Relatively stable but influenced by diet, antibiotics, illness, aging
### Factors Affecting Microbiota Composition
| Factor | Effect |
|---|---|
| Diet | Largest modifiable influence; high-fiber → ↑ Bacteroidetes, SCFA production; Western diet → ↑ Firmicutes, ↓ diversity |
| Antibiotics | Rapid disruption; loss of diversity; can persist for months-years |
| Age | Diversity decreases in elderly; ↑ Proteobacteria |
| Geography | Different populations have distinct microbiota profiles |
| Genetics | Twin studies show heritability of certain taxa |
| Stress | Alters composition via brain-gut-microbiota axis |
| Exercise | Increases diversity and SCFA-producing bacteria |
| Medications | PPIs, metformin, NSAIDs all alter microbiota |
| Disease | IBD, obesity, diabetes, cirrhosis all associated with dysbiosis |
## D. Functions of the Gut Microbiota
### 1. Metabolic Functions
#### a. Fermentation of Non-digestible Carbohydrates
- Dietary fiber, resistant starch, and oligosaccharides that escape digestion in the small intestine reach the colon
- Bacterial fermentation produces **short-chain fatty acids (SCFAs)**:
| SCFA | Producer Bacteria | Proportion | Key Functions |
|---|---|---|---|
| **Acetate** (C2) | Many species | 60% | Energy source for peripheral tissues; lipogenesis substrate; crosses BBB |
| **Propionate** (C3) | *Bacteroides*, *Prevotella* | 20% | Gluconeogenesis in liver; cholesterol synthesis inhibition; satiety signaling |
| **Butyrate** (C4) | *Faecalibacterium prausnitzii*, *Roseburia*, *Eubacterium rectale* | 20% | **Primary energy source for colonocytes** (provides 60-70% of their energy!); anti-inflammatory; promotes epithelial barrier integrity; inhibits histone deacetylase (HDAC) → epigenetic regulation; anti-cancer properties (promotes apoptosis of neoplastic cells) |
- SCFAs also stimulate water and sodium absorption in the colon
- SCFAs lower colonic pH → inhibits growth of pathogenic bacteria
- Total SCFA production: ~500 mmol/day, contributing ~10% of daily caloric intake
> **CLINICAL: Butyrate and Colorectal Cancer**
> - The "butyrate paradox": Butyrate promotes normal colonocyte proliferation at the base of crypts but promotes apoptosis and differentiation in cancer cells
> - High-fiber diets → more butyrate → may explain the reduced CRC risk with high-fiber diets
> - Low-fiber diets → reduced butyrate → impaired colonocyte barrier function → may promote inflammation and carcinogenesis
> - *Fusobacterium nucleatum* (enriched in CRC) may promote carcinogenesis
#### b. Bile Acid Metabolism
- Primary bile acids (cholic acid, chenodeoxycholic acid) synthesized in the liver from cholesterol
- Conjugated with glycine or taurine
- Secreted into duodenum, mostly reabsorbed in terminal ileum (enterohepatic circulation – 95% recycled)
- The ~5% that reaches the colon → bacteria deconjugate and transform them:
- **Bile salt hydrolase (BSH)** enzymes: Deconjugate bile acids
- **7α-dehydroxylase**: Converts primary bile acids to **secondary bile acids**:
- Cholic acid → **deoxycholic acid (DCA)**
- Chenodeoxycholic acid → **lithocholic acid (LCA)**
- Secondary bile acids have important signaling functions:
- Activate **FXR** (farnesoid X receptor) → regulates bile acid synthesis, glucose metabolism, lipid metabolism
- Activate **TGR5** (G-protein coupled bile acid receptor) → stimulates GLP-1 release from L cells, increases energy expenditure in brown adipose tissue
- This is a mechanism by which gut microbiota influence whole-body metabolism
> **CLINICAL: C. difficile and Bile Acids**
> - Normal gut microbiota convert primary bile acids to secondary bile acids
> - Secondary bile acids (especially DCA) **inhibit** C. difficile germination and growth
> - Antibiotics → kill normal flora → decreased secondary bile acid production → accumulation of primary bile acids → primary bile acids (especially taurocholate) **promote** C. difficile spore germination
> - This explains why antibiotic use predisposes to C. difficile infection
> - Fecal microbiota transplantation (FMT) restores secondary bile acid production → inhibits C. difficile
#### c. Vitamin Synthesis
Gut bacteria synthesize several vitamins:
- **Vitamin K₂** (menaquinone): By *Bacteroides*, *E. coli*, *Enterococcus* – contributes to host vitamin K needs
- **B vitamins**: Including biotin (B7), folate (B9), riboflavin (B2), cobalamin (B12), thiamine (B1), pyridoxine (B6), niacin (B3), pantothenate (B5)
- However, most bacterially produced vitamins in the colon are poorly absorbed (most B-vitamin absorption occurs in the small intestine)
> **CLINICAL: Vitamin K Deficiency in Neonates**
> - Newborns have a sterile gut and lack vitamin K-producing bacteria
> - Low vitamin K stores at birth → risk of **hemorrhagic disease of the newborn** (vitamin K deficiency bleeding, VKDB)
> - This is why all newborns receive intramuscular vitamin K at birth
#### d. Drug Metabolism
- Gut microbiota metabolize many drugs:
- **Digoxin**: Inactivated by *Eggerthella lenta* (formerly *Eubacterium lentum*)
- **Sulfasalazine**: Cleaved by colonic bacteria to 5-ASA (active) + sulfapyridine
- **Levodopa**: Can be decarboxylated to dopamine by gut bacteria before absorption → reduced bioavailability
- **Irinotecan (CPT-11)**: Bacterial β-glucuronidase reactivates its toxic metabolite SN-38 in the colon → severe diarrhea
#### e. Gas Production
- Bacterial fermentation produces gases:
- **H₂** (hydrogen)
- **CO₂** (carbon dioxide)
- **CH₄** (methane) – produced only by methanogenic archaea
- **H₂S** (hydrogen sulfide) – by sulfate-reducing bacteria; may be toxic to colonocytes at high concentrations
- Total gas production: ~200 mL/day; some is absorbed into blood and exhaled via lungs; rest is expelled as flatus
> **CLINICAL: Hydrogen and Methane Breath Tests**
> - Used to diagnose:
> - **Lactose intolerance**: Undigested lactose fermented → ↑ H₂ in breath
> - **SIBO**: Early rise in H₂ (or CH₄) after glucose or lactulose ingestion
> - **Fructose malabsorption**: Similar principle
> - **Methane-predominant**: Associated with constipation (methane slows intestinal transit)
> - Methane producers tend to have IBS-C; hydrogen producers tend to have IBS-D
### 2. Barrier and Protective Functions
#### a. Colonization Resistance
- Commensal bacteria prevent pathogen colonization through:
- **Competition for nutrients** (niche competition)
- **Competition for attachment sites** on the epithelium
- **Production of antimicrobial substances**: Bacteriocins, organic acids (SCFAs, lactic acid), hydrogen peroxide
- **Lowering luminal pH** (SCFAs create an acidic environment inhospitable to many pathogens)
- **Stimulation of the mucosal immune system**
> **CLINICAL: Antibiotic-Associated Diarrhea and C. difficile Infection**
> - Antibiotics disrupt colonization resistance → pathogen overgrowth
> - **Clostridioides difficile** infection:
> - Most common cause of hospital-acquired diarrhea
> - Risk factors: Antibiotics (especially fluoroquinolones, clindamycin, cephalosporins, carbapenems), hospitalization, age >65, PPI use
> - Produces toxins A (enterotoxin) and B (cytotoxin) → mucosal damage → diarrhea, pseudomembranous colitis
> - Pseudomembranes: Yellow-white plaques of fibrin, mucus, inflammatory cells, and debris on colonic mucosa
> - Diagnosis: Stool PCR for toxin gene, GDH antigen + toxin EIA (two-step algorithm)
> - Treatment: Oral vancomycin (first-line for initial non-severe and severe), fidaxomicin (lower recurrence), IV metronidazole (if PO not possible)
> - **Fecal Microbiota Transplantation (FMT)**: ~90% cure rate for recurrent C. difficile; restores normal microbiota and colonization resistance; donor stool delivered via colonoscopy, nasogastric tube, or capsules
> - **Bezlotoxumab**: Monoclonal antibody against toxin B; used to prevent recurrence
#### b. Enhancement of Epithelial Barrier
- SCFAs (especially butyrate) enhance tight junction protein expression (claudins, occludin, ZO-1)
- Bacteria stimulate mucus production by goblet cells
- *Akkermansia muciniphila* – while it degrades mucin, it also stimulates mucin production → net maintenance of mucus layer
- Commensal bacteria stimulate production of **trefoil factors** and **antimicrobial peptides** (defensins, cathelicidins, RegIII)
#### c. Stimulation of Intestinal Epithelial Renewal
- Bacterial products stimulate epithelial cell proliferation and turnover
- Germ-free animals have thinner intestinal walls, fewer and smaller Peyer's patches, and slower epithelial cell turnover
### 3. Immune Functions
#### a. Development and Maturation of the Immune System
- **GALT (Gut-Associated Lymphoid Tissue)**: The largest immune organ in the body
- Includes: **Peyer's patches** (organized lymphoid follicles in the ileum), isolated lymphoid follicles, lamina propria lymphocytes, intraepithelial lymphocytes, mesenteric lymph nodes
- Contains ~70% of the body's immune cells
- The microbiota is ESSENTIAL for normal immune development:
- **Germ-free (gnotobiotic) animals** have:
- Underdeveloped GALT
- Fewer and smaller Peyer's patches
- Reduced IgA production
- Impaired T-cell responses
- Deficient Th17 and Treg cell populations
- Colonization restores these deficits
#### b. Immune Training and Tolerance
**Segmented Filamentous Bacteria (SFB)**:
- Induce **Th17 cells** in the small intestine → important for mucosal defense against extracellular pathogens
- Also important for IgA induction
**Bacteroides fragilis (PSA – polysaccharide A)**:
- Promotes **Treg (regulatory T cell)** development → immune tolerance → anti-inflammatory
- Induces IL-10 production
**Clostridia (Clusters IV and XIVa)**:
- Major inducers of **colonic Treg cells** → immune homeostasis
- *Faecalibacterium prausnitzii* – considered a key anti-inflammatory commensal
**IgA Production**:
- Microbiota drives massive secretory IgA (sIgA) production – ~3-5 grams/day!
- sIgA: "Immune exclusion" – coats bacteria, prevents adhesion to epithelium, neutralizes toxins
- Does NOT activate complement → non-inflammatory defense
#### c. Hygiene Hypothesis / "Old Friends" Hypothesis
- Reduced microbial exposure in modern society → impaired immune regulation → increased autoimmune and allergic diseases
- Early-life microbial diversity is protective against atopic diseases
- Supporting evidence: Children raised on farms, with pets, or in developing countries have lower rates of asthma and allergies
> **CLINICAL: Inflammatory Bowel Disease (IBD) and Microbiota**
> - IBD (Crohn's disease and ulcerative colitis) associated with:
> - **Decreased microbial diversity** (especially reduced Firmicutes)
> - **Decreased** *Faecalibacterium prausnitzii* (anti-inflammatory, butyrate-producing)
> - **Increased** *Escherichia coli* (especially adherent-invasive E. coli, AIEC, in Crohn's disease)
> - **Increased** Proteobacteria overall
> - Loss of the normal mucus layer
> - Dysregulated immune response to commensal bacteria (loss of tolerance)
> - However, it's unclear if dysbiosis causes IBD or is a consequence
> - Antibiotics (metronidazole, ciprofloxacin) can help in some IBD subtypes (e.g., perianal Crohn's, pouchitis)
> - FMT for IBD: Under investigation; some benefit shown in UC, less clear in Crohn's
> - Probiotics: VSL#3 shown to help maintain remission in pouchitis
### 4. Neuromodulatory Functions – The Microbiota-Gut-Brain Axis
This is an emerging and rapidly growing field.
#### Pathways of Communication
The gut microbiota can influence brain function through:
1. **Vagus nerve**: Bacterial metabolites and products activate vagal afferents → signal to NTS → modulate brain function
- Cutting the vagus (vagotomy) blocks many of the behavioral effects of probiotics in animal studies
2. **Neuroactive metabolites produced by bacteria**:
- **GABA**: Produced by *Lactobacillus*, *Bifidobacterium*
- **Serotonin (5-HT)**: Bacteria promote 5-HT production by enterochromaffin cells (gut bacteria produce tryptophan hydroxylase activators); some bacteria produce 5-HT directly
- **Dopamine**: Produced by *Bacillus*, *Serratia*
- **Norepinephrine**: Produced by *Bacillus*, *Escherichia*
- **Acetylcholine**: Produced by *Lactobacillus*
- **Tryptophan metabolism**: Bacteria can shunt tryptophan to:
- Serotonin pathway
- Kynurenine pathway (→ quinolinic acid – neurotoxic; kynurenic acid – neuroprotective)
- Indole pathway (→ indole, indole-3-propionic acid – neuroprotective, anti-inflammatory)
3. **Immune mediators**: Bacterial products (LPS, peptidoglycan, SCFAs) modulate systemic cytokine levels that affect brain function
4. **HPA axis**: Microbiota influences stress response; germ-free animals show exaggerated cortisol/corticosterone response to stress
5. **SCFAs**: Cross the blood-brain barrier; influence microglia (brain's immune cells) maturation and function; modulate BBB integrity
> **CLINICAL: Microbiota and Neuropsychiatric Disorders**
> - Depression: Altered microbiota composition; decreased Lactobacillus and Bifidobacterium; FMT from depressed patients to germ-free rats can induce depressive-like behavior
> - Anxiety: Probiotic supplementation (especially L. rhamnosus, B. longum) reduces anxiety in animal models and some human trials ("psychobiotics")
> - Autism Spectrum Disorder (ASD): Altered microbiota; GI symptoms common; increased Clostridium species; FMT trials showing some improvement
> - Parkinson's Disease: α-synuclein pathology may begin in the gut; altered microbiota; constipation precedes motor symptoms by years; bacterial amyloid (curli fibers from E. coli) may promote α-synuclein misfolding
> - Hepatic encephalopathy: Gut bacteria produce ammonia; dysbiosis contributes to hyperammonemia; **Lactulose** is used to treat HE (acts as osmotic laxative + prebiotic → acidifies colonic contents → converts NH₃ to NH₄⁺ which cannot be absorbed + promotes growth of Lactobacillus → decreases ammonia-producing bacteria)
> - **Rifaximin**: Non-absorbable antibiotic used for prevention of HE recurrence; modulates gut microbiota rather than sterilizing it
### 5. Metabolic Functions (Systemic)
#### a. Obesity
- Obese individuals tend to have:
- Increased Firmicutes/Bacteroidetes ratio
- Decreased microbial diversity
- Enhanced capacity for energy harvest from food
- Germ-free mice colonized with obese human microbiota gain more weight than those colonized with lean microbiota
- Mechanisms: Increased SCFA production (more caloric extraction), increased intestinal permeability → metabolic endotoxemia (LPS) → low-grade inflammation → insulin resistance
#### b. Type 2 Diabetes
- Dysbiosis associated with decreased butyrate producers, increased Proteobacteria
- Metabolic endotoxemia: Increased intestinal permeability → LPS enters blood → activates TLR4 on immune cells → chronic low-grade inflammation → insulin resistance
- **Metformin** (first-line diabetes drug) alters gut microbiota → increases *Akkermansia muciniphila* → improved glucose metabolism; some of metformin's therapeutic effect may be mediated through the microbiota
- Gut microbiota also influence bile acid signaling (FXR, TGR5) which affects glucose homeostasis
#### c. Cardiovascular Disease
- **TMAO (Trimethylamine-N-Oxide) pathway**:
- Dietary choline, L-carnitine, and betaine (found in red meat, eggs, fish) → gut bacteria produce **TMA (trimethylamine)**
- TMA absorbed → liver oxidizes it to **TMAO** (by flavin monooxygenase 3, FMO3)
- TMAO promotes:
- Atherosclerosis (increased cholesterol uptake by macrophages → foam cells)
- Platelet hyperreactivity → thrombosis
- Inflammatory cytokine production
- Elevated TMAO levels associated with increased risk of MI, stroke, and death
- This is a mechanism linking dietary habits, gut microbiota, and cardiovascular disease
> **CLINICAL: TMAO and Diet**
> - Vegans/vegetarians have significantly lower TMAO levels (fewer TMA-producing bacteria due to low carnitine/choline intake)
> - Even when given L-carnitine, vegans produce very little TMA (because their microbiota lacks the necessary metabolic capacity)
> - This partly explains the cardiovascular benefit of plant-based diets
### 6. Cancer
- **Colorectal Cancer**:
- *Fusobacterium nucleatum*: Enriched in CRC tissue; promotes tumorigenesis via FadA adhesin → activates β-catenin signaling; recruits tumor-infiltrating myeloid cells → immunosuppressive microenvironment
- *Bacteroides fragilis* (enterotoxigenic strains, ETBF): Produces fragilysin (metalloproteinase) → cleaves E-cadherin → β-catenin signaling → promotes proliferation
- **Butyrate** from fiber-fermenting bacteria is generally protective (see above)
- Secondary bile acids (DCA) in excess may promote CRC by causing DNA damage and proliferative signaling
- **Gastric Cancer**:
- *Helicobacter pylori*: Class I carcinogen; causes chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → adenocarcinoma (Correa cascade)
- Also causes gastric MALT lymphoma
> **CLINICAL: H. pylori and GI Physiology**
> - Infects ~50% of the world's population
> - Produces **urease** → converts urea to ammonia + CO₂ → creates alkaline microenvironment → neutralizes gastric acid locally → survives in the stomach
> - Infection of the antrum: ↑ gastrin release (by reducing somatostatin from D cells) → ↑ acid secretion → duodenal ulcers
> - Pangastritis: Destruction of parietal cells → ↓ acid secretion → atrophic gastritis → gastric ulcers and gastric cancer risk
> - Diagnosis: Urea breath test (¹³C or ¹⁴C), stool antigen test, histology with special stains, rapid urease test (CLO test)
> - Treatment: Triple therapy (PPI + clarithromycin + amoxicillin or metronidazole) × 14 days; quadruple therapy (PPI + bismuth + metronidazole + tetracycline) for resistant strains
### 7. Other Functions
#### a. Oxalate Metabolism
- *Oxalobacter formigenes* degrades dietary oxalate in the colon
- Reduces oxalate absorption → reduces urinary oxalate → reduces kidney stone risk
- Antibiotic use can eliminate *O. formigenes* → increased oxalate absorption → hyperoxaluria → calcium oxalate kidney stones
#### b. Bilirubin Metabolism
- Bilirubin is conjugated in the liver and excreted in bile
- Colonic bacteria deconjugate and reduce bilirubin → **urobilinogen**
- Urobilinogen → **stercobilin** (gives stool brown color)
- Some urobilinogen reabsorbed → excreted by kidneys → **urobilin** (gives urine yellow color)
> **CLINICAL: Neonatal Jaundice and Microbiota**
> - Neonates have limited gut bacteria → reduced bilirubin metabolism → unconjugated bilirubin reabsorbed (enterohepatic circulation of bilirubin) → contributes to physiological jaundice
---
## E. Probiotics, Prebiotics, Synbiotics, and Postbiotics
### Definitions
| Term | Definition | Examples |
|---|---|---|
| **Probiotics** | Live microorganisms that confer a health benefit when administered in adequate amounts | *Lactobacillus rhamnosus GG*, *Saccharomyces boulardii*, *Bifidobacterium longum*, VSL#3 |
| **Prebiotics** | Non-digestible food ingredients that selectively stimulate growth/activity of beneficial bacteria | Inulin, fructooligosaccharides (FOS), galactooligosaccharides (GOS), lactulose, resistant starch, HMOs |
| **Synbiotics** | Combination of probiotics + prebiotics | Various commercial preparations |
| **Postbiotics** | Bioactive compounds produced by probiotics (metabolites, cell wall components) | SCFAs, bacteriocins, exopolysaccharides |
### Evidence-Based Uses of Probiotics
| Condition | Evidence Level |
|---|---|
| Antibiotic-associated diarrhea prevention | Strong (Lactobacillus, S. boulardii) |
| C. difficile prevention | Moderate |
| Acute infectious diarrhea (children) | Strong (LGG, S. boulardii) |
| Pouchitis maintenance | Strong (VSL#3) |
| Necrotizing enterocolitis prevention (preterm infants) | Strong |
| IBS symptoms | Moderate (strain-specific) |
| Ulcerative colitis maintenance | Moderate |
| Traveler's diarrhea prevention | Moderate |
| Hepatic encephalopathy | Moderate |
| Atopic dermatitis prevention | Moderate |
| H. pylori eradication (adjunct) | Moderate |
---
## F. Methods of Studying the Microbiota
Understanding how we study the microbiome is increasingly important:
1. **16S rRNA gene sequencing**: Amplifies and sequences the bacterial 16S ribosomal RNA gene → identifies bacteria to genus/species level
2. **Metagenomic shotgun sequencing**: Sequences all microbial DNA → provides functional information (what genes are present)
3. **Metatranscriptomics**: Studies which microbial genes are actively expressed
4. **Metabolomics**: Measures microbial metabolites (SCFAs, bile acids, TMAO, etc.)
5. **Culturomics**: Advanced culture techniques to grow previously "unculturable" bacteria
6. **Gnotobiotic (germ-free) animal models**: Animals raised in sterile conditions → can be colonized with specific bacteria to study their effects
---
# INTEGRATION AND SUMMARY
## How These Systems Interact
The four systems – **motility, nervous control, hormonal control, blood circulation, and microbiota** – do not function in isolation. They are deeply integrated:
1. **Nervous system → Motility**: ENS generates and coordinates motor patterns; extrinsic nerves modulate them
2. **Hormones → Motility**: CCK inhibits gastric emptying; motilin initiates MMC; gastrin enhances antral contractions
3. **Hormones → Blood flow**: CCK, gastrin, secretin increase mucosal blood flow; somatostatin decreases it
4. **Nervous system → Blood flow**: Sympathetic vasoconstriction; parasympathetic indirect vasodilation
5. **Blood flow → Motility/Secretion**: Adequate blood flow essential for sustained motility and secretion
6. **Motility → Microbiota**: MMC sweeps bacteria distally; disrupted motility → SIBO
7. **Microbiota → Nervous system**: Microbial metabolites affect ENS and CNS via vagus (microbiota-gut-brain axis)
8. **Microbiota → Hormones**: SCFAs stimulate PYY and GLP-1 from L cells; bile acid metabolism influences FXR/TGR5 signaling
9. **Microbiota → Blood flow**: Bacterial products (e.g., LPS) can cause inflammation → altered vascular function; SCFAs may promote vasodilation
10. **Microbiota → Motility**: SCFAs stimulate colonic motility; methane from archaea slows motility
---
## Master Clinical Correlation Summary
| Clinical Condition | Pathophysiology (Related to this chapter) |
|---|---|
| Hirschsprung's disease | Absent ENS ganglion cells → tonic contraction → obstruction |
| Achalasia | Loss of inhibitory neurons (VIP/NO) in LES → failure to relax |
| GERD | TLESRs, decreased LES tone → acid reflux |
| Peptic ulcer disease | H. pylori, NSAIDs → disrupted mucosal defense → ulceration |
| Zollinger-Ellison | Gastrinoma → excess gastrin → acid hypersecretion |
| Gastroparesis | ICC loss, vagal neuropathy → delayed gastric emptying |
| SIBO | Disrupted MMC → bacterial overgrowth → malabsorption |
| IBS | Altered motility, visceral hypersensitivity, dysbiosis, brain-gut dysfunction |
| C. difficile | Antibiotics → dysbiosis → loss of colonization resistance → toxin-mediated disease |
| IBD | Dysbiosis + loss of immune tolerance → chronic inflammation |
| Mesenteric ischemia | Reduced splanchnic blood flow → mucosal necrosis |
| Portal hypertension | Increased portal venous pressure → varices, ascites, encephalopathy |
| Dumping syndrome | Post-surgical loss of gastric reservoir/pyloric regulation → rapid emptying |
| Carcinoid syndrome | Excessive 5-HT → diarrhea, flushing |
| Obesity | Altered microbiota → increased energy harvest, metabolic endotoxemia |
| Short bowel syndrome | Loss of absorptive surface → malabsorption; treated with teduglutide (GLP-2 analog) |
---
This comprehensive overview covers the fundamental physiological principles of the GI system—from the electrical basis of smooth muscle contraction, through the intricate neural and hormonal regulatory networks, to the splanchnic circulation and the vast microbial ecosystem that inhabits our gut. Each of these systems is essential for normal GI function, and their disruption underlies many of the most common and important clinical conditions in gastroenterology and medicine.