SLR test
Reading File
Finding Sources
Searching PubMed
"straight leg raise" test diagnostic accuracy lumbar
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive textbook content. Here is the full answer:
Straight Leg Raise (SLR) Test
Overview
The SLR test (also called Lasègue's test) is a provocative maneuver used to detect nerve root irritation in the lumbosacral spine - most commonly from a herniated intervertebral disc at L4-L5 or L5-S1 compressing the L4, L5, or S1 nerve roots.
Technique (Supine SLR)
- Position the patient supine with legs passively extended. Confirm the quadriceps are relaxed - the patella should move freely side-to-side.
- Cradle the heel in one hand while placing the other hand on the knee to maintain extension.
- Slowly raise the leg by flexing at the hip, keeping the knee fully extended.
- Observe and ask about pain throughout the arc of motion.
Positive result: Radicular pain (sciatica) that radiates below the knee of the raised leg, reproduced at 30-70 degrees of elevation.
Pain limited to the posterior knee, hamstring area, or gluteal region alone is not a positive result - this is a nonspecific finding.
Sensitivity enhancer: Dorsiflexing the ankle (Bragard's test) at the angle of pain reproduction - if pain worsens, it increases sensitivity for nerve root tension. Pain relief with ankle plantarflexion or decreasing elevation further confirms the test.
Variants
Crossed (Contralateral) SLR
- Performed identically, but a positive result occurs when raising the asymptomatic leg reproduces radicular pain in the symptomatic (contralateral) leg.
- More specific for an axillary (medial) disc herniation (disc pushing the nerve root toward the midline).
- If SLR is positive AND crossed SLR is positive: confirms disc impingement.
- If SLR is negative BUT crossed SLR is positive: disc herniation is still highly likely.
Seated (Sitting) SLR
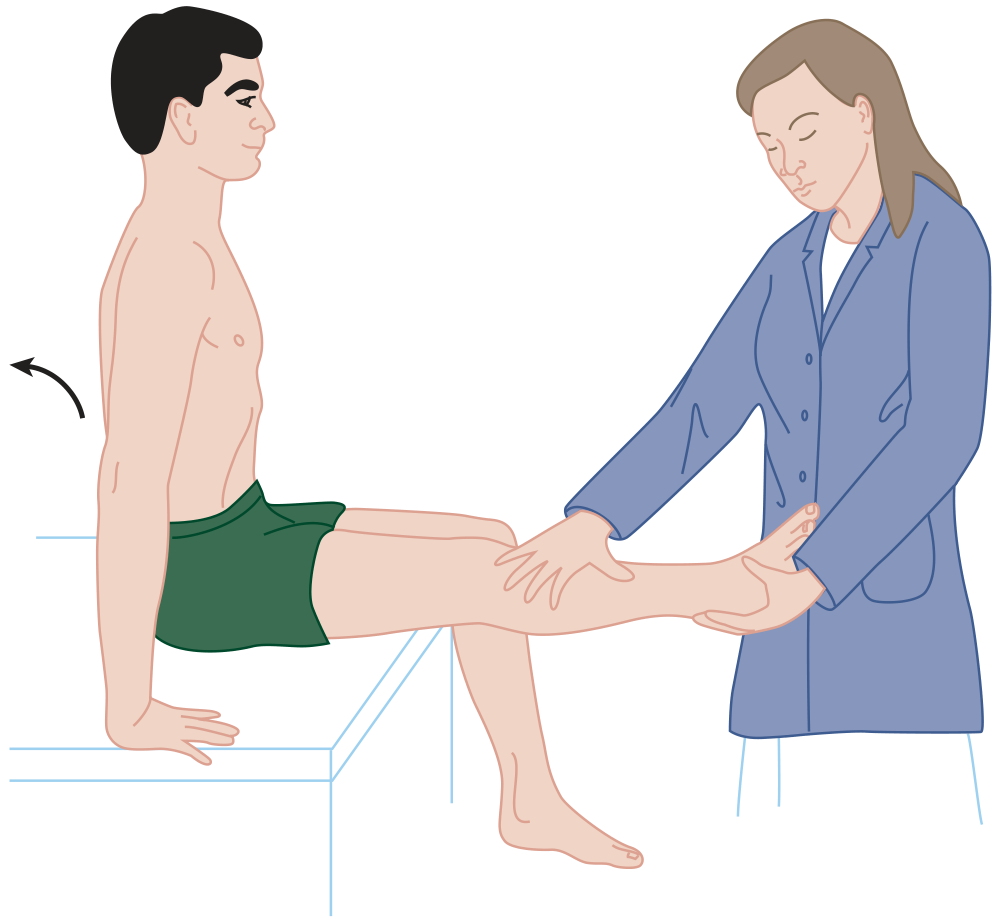
- Patient sits on the table with hips and knees at 90°.
- The examiner slowly extends the knee as if examining the patella or foot.
- A positive result reproduces radiating leg pain.
- This stretches the nerve roots comparably to moderate-degree supine SLR (~65°).
- Less sensitive than the supine SLR.
- One-third of patients with a positive supine SLR but negative seated SLR still have an MRI-proven herniated disc.
Reverse SLR (Femoral Stretch Test)
- Patient is prone; examiner maximally flexes the knee with the hip extended.
- Positive if anterior thigh pain is reproduced.
- Sensitive for L2, L3, and L4 nerve root irritation (upper lumbar/femoral nerve territory), but not very specific.
Lasègue Sign
- Relief of radiating leg symptoms when the knee is flexed while the hip is already flexed - this relaxes the sciatic nerve tension and confirms the SLR was truly positive.
Diagnostic Accuracy (for lumbar disc herniation)
| Finding | Sensitivity | Specificity | LR+ | LR- |
|---|---|---|---|---|
| Positive ipsilateral SLR | 85-91% | 26-50% | 1.2-1.8 | 0.18-0.3 |
| Positive crossed SLR | 25% | 90% | 2.5 | 0.83 |
| Sciatica (symptom) | 95% | 88% | 7.9 | 0.06 |
(Source: Symptom to Diagnosis, 4th Ed.)
Key takeaways:
- Ipsilateral SLR is a good rule-out test (high sensitivity, low LR-) - a negative SLR argues against lumbar disc herniation.
- Crossed SLR is a good rule-in test (high specificity) - a positive crossed SLR strongly confirms the diagnosis.
- The SLR is 68-80% sensitive for L4-L5 or L5-S1 herniated disc.
Nerve Roots Tested
| Nerve Root | Clinical Clues |
|---|---|
| L4 | Foot dorsiflexion weakness, medial ankle/foot sensory loss, diminished patellar reflex |
| L5 | Great toe extensor weakness (EHL), lateral calf/dorsum of foot sensory loss, no reflex change |
| S1 | Plantarflexion weakness, lateral foot/5th toe sensory loss, diminished Achilles reflex |
Clinical Interpretation
- A positive SLR should prompt neurologic testing: patellar and Achilles reflexes, plantar reflex (Babinski), perineal sensation, and anal tone.
- Hyperreflexia, clonus, or a positive Babinski indicates upper motor neuron (cord) pathology rather than simple nerve root compression.
- Bilateral symptoms, saddle anesthesia, or bowel/bladder dysfunction require emergent evaluation for cauda equina syndrome.
Sources: Rosen's Emergency Medicine 9th Ed. - Goldman-Cecil Medicine - Tintinalli's Emergency Medicine - Miller's Review of Orthopaedics 9th Ed. - Symptom to Diagnosis 4th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.