hi
Hi! How can I help you today?
Bile leak with drain photo. search best ones. search books and images..
Reading File
Finding Sources
Finding Sources
Searching Images
bile leak drain surgical abdominal
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of bile leak with drain — combining the best textbook content and clinical images found.
Bile Leak with Drain — Clinical Overview
1. What Is a Bile Leak?
A bile leak occurs when bile escapes from the biliary tree — most commonly after cholecystectomy (from the cystic duct stump or a duct of Luschka), hepatic resection, or biliary reconstruction. When a drain was placed in the operative bed, bilious output from the drain is often the earliest sign.
Clinical features:
- Fevers, chills, right upper quadrant pain
- Jaundice or leakage of bile from an incision
- Bilious fluid in a surgically placed drain
- Persistent anorexia or bloating
"Leakage of bile from an incision or into a drain … are common signs and symptoms." — Sabiston Textbook of Surgery
2. Imaging — CT & ERCP
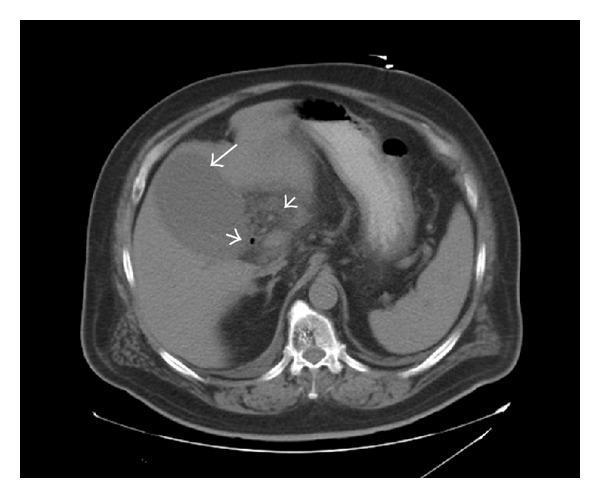
CT Scan — Bile Leak After Cholecystectomy
(Schwartz's Principles of Surgery, 11e)
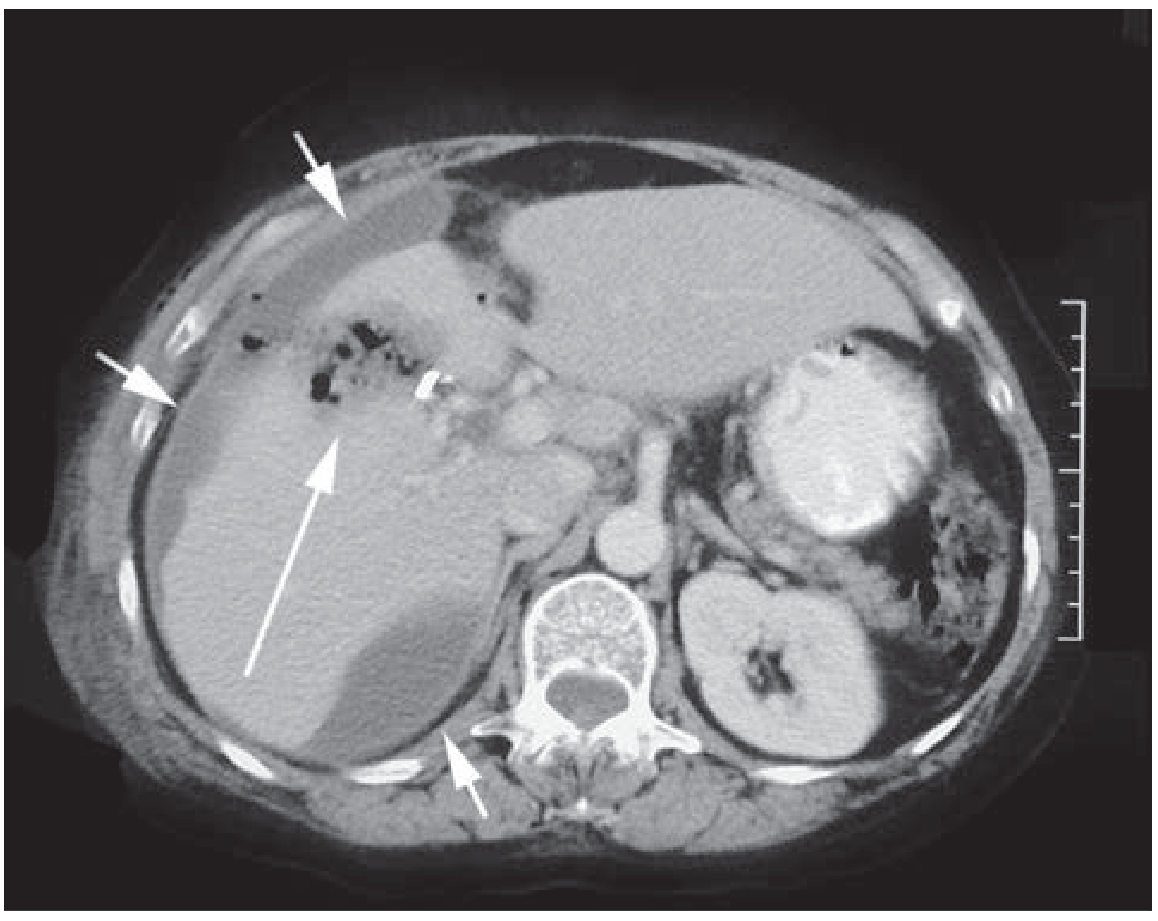
Figure A — CT abdomen: Short arrows indicate intraperitoneal fluid collections (biloma); the long arrow points to air and bile in the gallbladder bed, along with a surgical clip. This is the classic post-cholecystectomy bile leak appearance.
ERCP — Contrast Extravasation from Cystic Duct Stump
(Schwartz's Principles of Surgery, 11e)
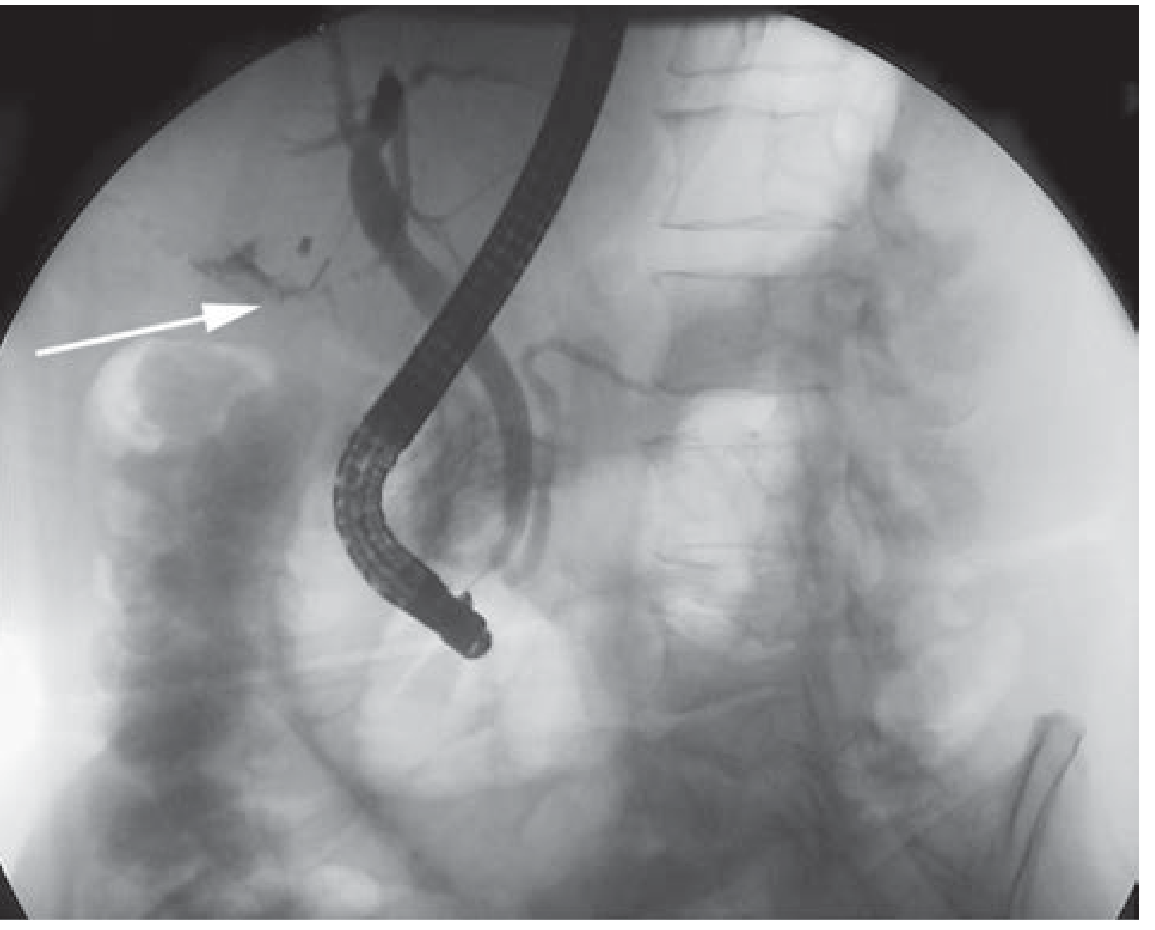
Figure B — Same patient as CT above. ERCP demonstrates contrast extravasation from the cystic duct stump (white arrow). ERCP with sphincterotomy ± stenting is the primary treatment for high-output leaks.
Fluoroscopic Cholangiogram — Active Bile Leak with Drain
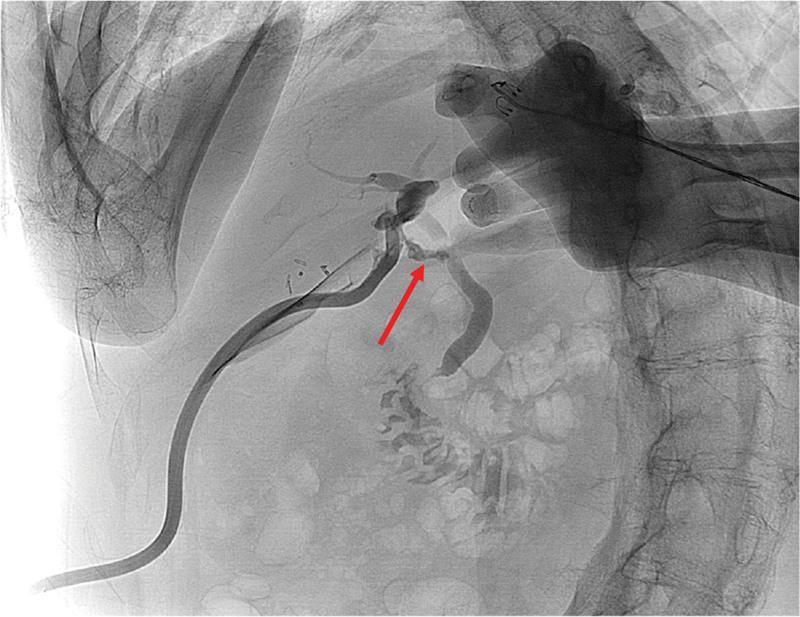
Cholangiogram — Red arrow marks active contrast extravasation at the mid-CBD. An external surgical drain enters from the lower-left, with its tip positioned at the leak site to facilitate biliary decompression. Surgical clips are visible in the right upper quadrant. This is the classic image of a bile leak managed with percutaneous drainage.
3. Intraoperative Photos
Intraoperative Bile Duct Cannulation for Leak Testing (After Hepatic Resection)

A 12 Fr infant feeding tube (green) cannulated into the cystic duct stump for intraoperative saline injection — a technique used during hepatic resection to identify and ligate biliary leaks on the raw cut surface before closure.
Intraoperative — Bile Staining of Diaphragm (Chemical Peritonitis)
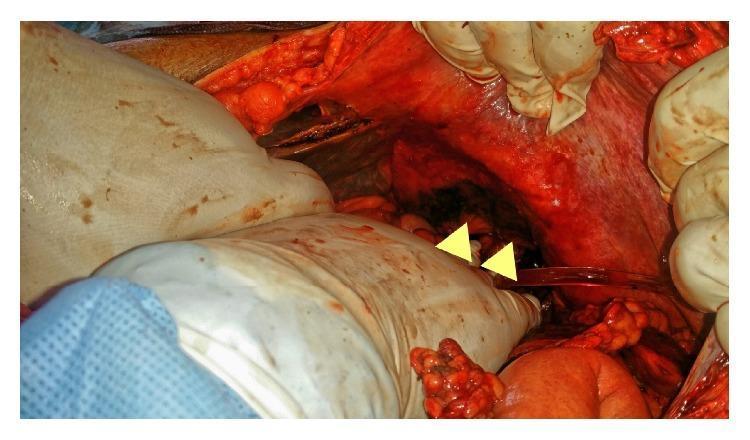
Yellow arrowheads point to brownish-green bile staining on the under-surface of the left diaphragm — indicating a prior bile leak causing chemical peritonitis. Surrounding tissues show inflammatory hyperemia with serosanguinous fluid pooling.
4. Clinical Photo — Skin Discoloration After Retroperitoneal Bile Leak

Post-ERCP stenting: receding yellow-brown skin pigmentation (icterus marginatus) from a retroperitoneal bile leak. Pen marks trace the previous extent of discoloration, showing improvement. Small adhesive dressings cover laparoscopic port/drain sites. A rare but dramatic clinical sign.
5. Management Summary
| Output | Management |
|---|---|
| Low output (<300 mL/day) | Drain in place → may dry up spontaneously |
| High output (>300–500 mL/day) | ERCP + sphincterotomy ± biliary stent |
| Peritonitis / non-localizable | Laparoscopic washout + subhepatic drain placement |
| Inaccessible percutaneously | Laparoscopic approach — do NOT attempt to repair the leak directly |
| Persistent >6 weeks | Suspect unrecognized bile duct injury; surgical reconstruction after inflammation resolves |
"No attempt should be made to fix the leak; any such intervention is almost always unsuccessful and risks further biliary tree injury." — Sabiston Textbook of Surgery, 20e
Sources:
- Sabiston Textbook of Surgery (20e) — Biliary Leak, p. 1847
- Schwartz's Principles of Surgery (11e) — Extrahepatic Bile Ducts, Fig. 32-29
- Current Surgical Therapy (14e) — Bile Leak & Postoperative Care
Diabetic / thickened gallbladder images
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Diabetic / thickened gallbladder images
Reading File
Finding Sources
Finding Sources
Searching Images
thickened gallbladder wall ultrasound diabetic cholecystitis
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Searching Images
emphysematous cholecystitis CT scan gas gallbladder diabetic
Loading Image
Loading Image
Here is a comprehensive visual and clinical overview of diabetic / thickened gallbladder findings.
Diabetic & Thickened Gallbladder — Imaging Overview
The Diabetes–Gallbladder Connection
Diabetes affects the gallbladder in several important ways:
- Acalculous cholecystitis — Diabetes is a direct risk factor. Increased bile viscosity from stasis causes functional cystic duct obstruction without stones.
- Emphysematous cholecystitis — ~50% of cases occur in diabetics. Gas-forming organisms (e.g. Clostridium, E. coli) infect the ischemic gallbladder wall.
- Diabetic neuropathy — Denervated gallbladders may present without a sonographic Murphy's sign, masking the diagnosis.
- Gangrenous cholecystitis — More common in diabetics due to vascular compromise.
"Patients with denervated gallbladders, either as a result of diabetes or gangrenous cholecystitis, can present without a sonographic Murphy's sign." — Yamada's Textbook of Gastroenterology, 7e
Section 1 — Ultrasound: Thickened Gallbladder Wall
Acalculous Cholecystitis — Wall Thickness 8.3 mm
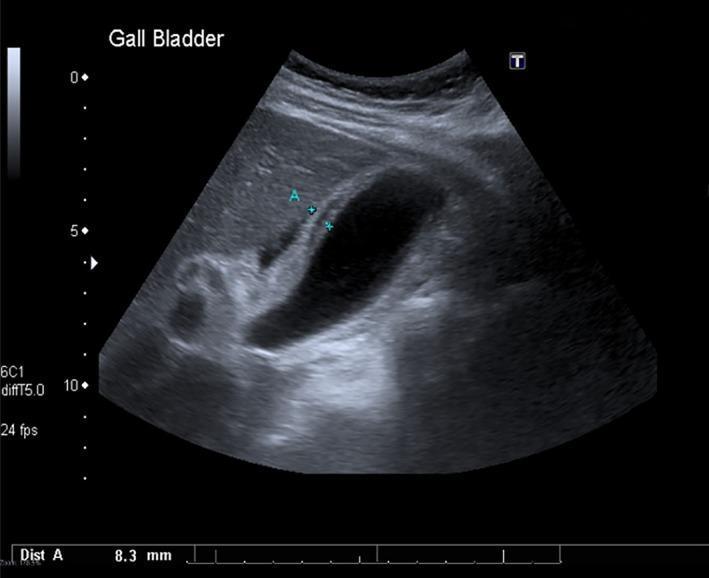
Ultrasound — Acute Acalculous Cholecystitis. Wall thickness measured at 8.3 mm (normal <3 mm). The lumen is anechoic — no stones. Pericholecystic fluid is present. This is the classical diabetic/ICU pattern: thickened wall, distended GB, no calculi.
Calculous Cholecystitis — Thickened Wall + Stone
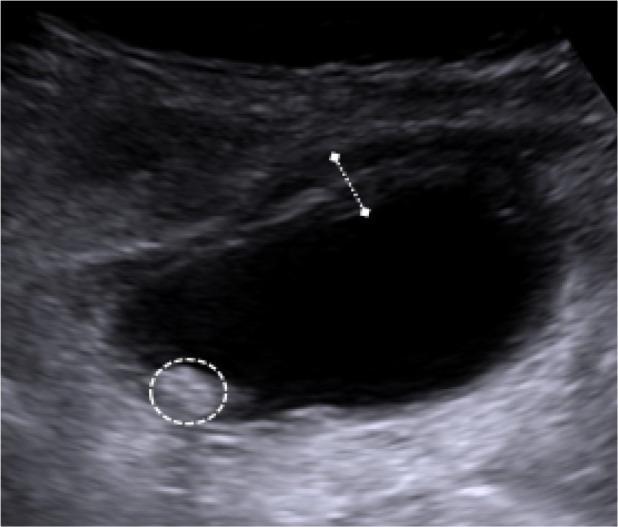
Acute Calculous Cholecystitis. Thickened, layered GB wall (measured by calipers). A hyperechoic stone (dashed circle) is visible in the dependent portion with posterior acoustic shadowing. Diabetic patients may present late or without typical Murphy's sign.
Acalculous Cholecystitis — Sludge + Wall Thickening
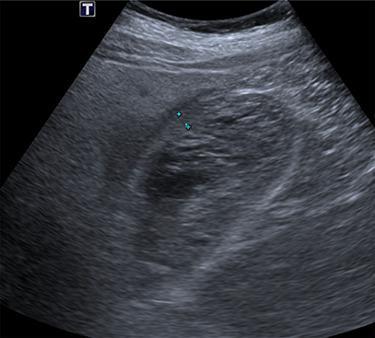
Acalculous / Hemorrhagic Cholecystitis. Thickened wall + intraluminal sludge/debris (no shadowing stone). Pericholecystic fluid layer. No gallstones. This pattern is typical in critically ill diabetic patients.
Xanthogranulomatous Cholecystitis — Focal Wall Thickening + Doppler

Xanthogranulomatous Cholecystitis. Panel A: focal wall thickening at the gallbladder base with layered texture. Panel B: Color Doppler shows absent flow (CDFI=0) — helps differentiate from carcinoma. Categorized GB-RADS 2 (low malignancy risk).
Cholecystitis — Stones + Sludge + Thickened Wall

Cholecystitis — Stones + Sludge. Thickened wall, internal biliary sludge, multiple small echogenic stones with posterior shadowing, and pericholecystic fluid. A common combined picture in diabetic patients.
Section 2 — CT Scan: Emphysematous Cholecystitis in Diabetics
"About 50% of patients with emphysematous cholecystitis are diabetics and stones are present in less than 50%." — Grainger & Allison's Diagnostic Radiology
Emphysematous Cholecystitis — Coronal CT (Diabetic Patient)
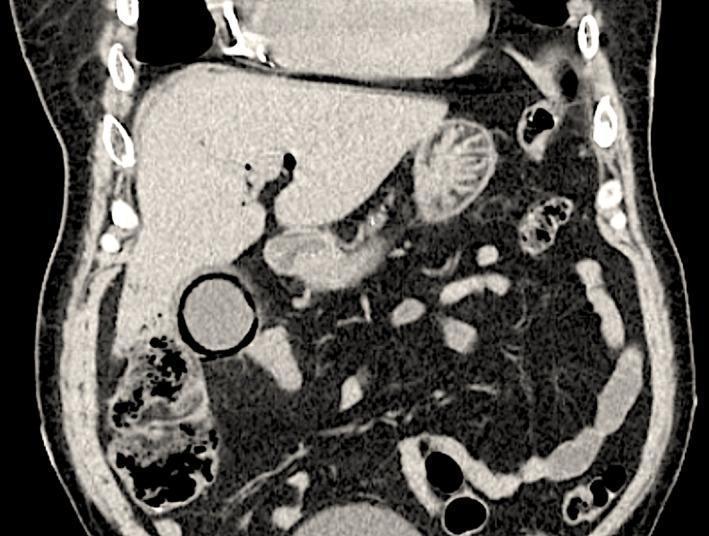
Emphysematous Cholecystitis — Diabetic Patient (Coronal CT). Circumferential intramural gas (dark ring) within the thickened GB wall — pathognomonic for emphysematous cholecystitis. Intraluminal gas also present. Incidental chronic calcific pancreatitis is visible. Surgical emergency.
Emphysematous Cholecystitis — Axial CT
Emphysematous Cholecystitis — Axial CT. Markedly distended GB (long arrow). Multiple focal air bubbles at the GB neck (short arrows) = intramural/intraluminal gas. Classic in elderly diabetic males; caused by gas-forming organisms. Requires urgent cholecystectomy or cholecystostomy.
Ultrasound Diagnostic Criteria Summary
| Feature | Normal | Cholecystitis |
|---|---|---|
| Wall thickness | <3 mm | >3 mm (often >5 mm) |
| Lumen | Clear, anechoic | Sludge, debris |
| Stones | Absent | Present (calculous) or absent (acalculous) |
| Pericholecystic fluid | Absent | Present |
| Murphy's sign | Negative | Positive (but may be absent in diabetics) |
| Intramural gas | Absent | Emphysematous type — surgical emergency |
Sources:
- Yamada's Textbook of Gastroenterology (7e) — Cholecystitis, p. 2663
- Grainger & Allison's Diagnostic Radiology — Emphysematous & Acalculous Cholecystitis
- Sabiston Textbook of Surgery — Acute Acalculous Cholecystitis
This is a shared conversation. Sign in to Orris to start your own chat.