Neonatal resuscitation
Reading File
Finding Sources
Searching PubMed
"neonatal resuscitation" guidelines
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content for a thorough answer. Let me compile it all.
Neonatal Resuscitation
Approximately 10% of newborns require some assistance at birth, and fewer than 1% need advanced resuscitative measures. The vast majority respond to the initial steps alone.
Pre-Birth Preparation
Before every delivery, a team briefing and equipment check should be completed. Key equipment includes:
- Radiant warmer, warm blankets, plastic wrap (for preterm)
- Bulb syringe, suction catheter (sizes 5, 8, 10 Fr) at ~100 mmHg
- Self-inflating bag (450/750 mL) + age-appropriate masks
- Laryngoscope with straight blades (00, 0, 1)
- ETT sizes 2.5-4.0 mm (uncuffed), stylets, CO2 detector
- Umbilical catheters (3.5 and 5 Fr) for vascular access
Key maternal history questions: gestational age, multiple gestation, meconium presence, medications/drugs, maternal fever, prenatal anomalies.
The NRP Algorithm (Step by Step)
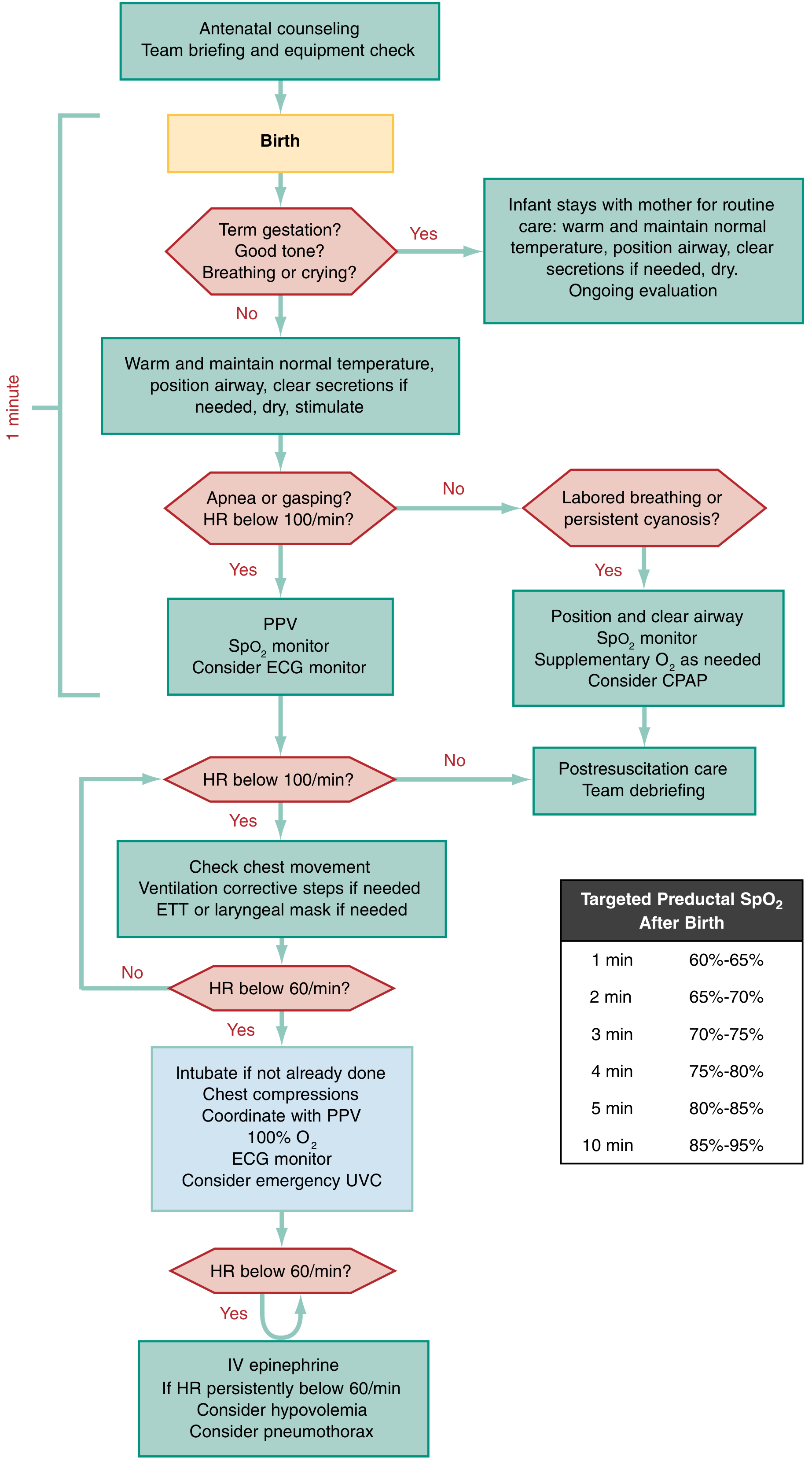
AHA Neonatal Resuscitation Algorithm - ROSEN's Emergency Medicine
Step 1 - Initial Assessment (within 60 seconds - "The Golden Minute")
Ask three questions simultaneously:
- Term gestation?
- Good tone?
- Breathing or crying?
If all three are YES → infant stays with mother for routine care (warm, dry, position airway, observe).
If ANY is NO → proceed to resuscitation steps.
Step 2 - Initial Steps (Warm, Dry, Stimulate)
- Place under radiant warmer
- Position airway (slight neck extension, "sniffing" position)
- Clear secretions only if obstructed (mouth first, then nose)
- Dry and stimulate (rub the back, flick soles of feet)
- Delayed cord clamping 1-3 minutes for vigorous term infants
Suction precautions: Overly vigorous/deep suctioning causes vagal stimulation, bradycardia, and apnea. Use only if obstruction is present, and keep suction <100 mmHg.
Step 3 - Re-assess: Labored Breathing or Persistent Cyanosis (HR >100)?
- Position and clear airway
- Monitor SpO2 (on right hand/wrist - preductal)
- Supplemental O2 as needed to reach targeted saturations
- Consider CPAP
Targeted Preductal SpO2 After Birth:
| Time | Target SpO2 |
|---|---|
| 1 min | 60-65% |
| 2 min | 65-70% |
| 3 min | 70-75% |
| 4 min | 75-80% |
| 5 min | 80-85% |
| 10 min | 85-95% |
Oxygen Note: Resuscitation with 100% O2 is no longer recommended. Start with room air (21%) for term infants and 21-30% FiO2 for preterm (<35 weeks). Titrate upward to achieve target SpO2. 100% O2 is reserved for HR <60 bpm after 90 seconds. Hyperoxia causes oxidative stress and cardiac/renal/neurologic injury. - ROSEN's Emergency Medicine
Step 4 - Apnea, Gasping, or HR <100 bpm → Positive Pressure Ventilation (PPV)
- Rate: 40-60 breaths/min
- Pressure: 30 cm H2O (term); 20-25 cm H2O (preterm)
- Best indicators of effectiveness: chest rise and increasing HR (usually within 5-10 breaths)
- Apply SpO2 monitor and consider ECG monitor (3-lead ECG is more accurate than pulse oximetry or umbilical palpation for HR)
APGAR Score (assessed at 1, 5, and 10 minutes):
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| Heart rate | Absent | <100/min | ≥100/min |
| Respiratory effort | Absent | Weak/irregular | Strong, crying |
| Muscle tone | Limp | Some flexion | Active motion |
| Reflex irritability | None | Grimace | Cry/cough/sneeze |
| Color | Blue/pale all over | Blue extremities | Completely pink |
The 1-minute score guides need for resuscitation; the 5-minute score assesses efficacy.
If PPV is not working - use MR SOPA:
- Mask - adjust seal
- Reposition the head
- Suction mouth then nose
- Open mouth with jaw thrust
- Pressure - increase (max 40 cm H2O)
- Airway - definitive (intubate)
Step 5 - HR Still <100 After PPV → Check Ventilation, Consider Intubation
Check chest movement and take ventilation corrective steps. If still no improvement, intubate or place LMA.
Intubation indications:
- Ineffective or prolonged bag-mask ventilation
- Tracheal suctioning for non-vigorous infant with meconium
- Chest compressions
- Extremely low birth weight or anatomic anomalies (e.g., diaphragmatic hernia)
ETT size by weight/gestational age:
| Gestational Age | Weight | ETT Size |
|---|---|---|
| <28 weeks | <1000 g | 2.5 mm |
| 28-34 weeks | 1000-2000 g | 3.0 mm |
| 34-38 weeks | 2000-3000 g | 3.5 mm |
| >38 weeks | >3000 g | 3.5-4.0 mm |
ETT confirmation: expired CO2 via capnography (gold standard: plain radiograph).
Post-intubation deterioration - DOPE mnemonic:
- Dislodged tube
- Obstructed tube
- Pneumothorax
- Equipment failure
Step 6 - HR <60 bpm Despite Adequate Ventilation → Chest Compressions
- Begin compressions if HR <60 after 30 seconds of adequate ventilation
- Ratio: 3:1 compressions to ventilations (90 compressions + 30 breaths = 120 events/min)
- Technique: Thumb-encircling method (preferred) - both thumbs on lower 1/3 of sternum, fingers encircling the chest
- Depth: ~1/3 of AP chest diameter
- Escalate FiO2 to 100%
- Establish emergency umbilical vein catheter (UVC)
- ECG monitor essential
If cardiac arrest is known to be of primary cardiac etiology, a 15:2 ratio (as in pediatric CPR) may be more appropriate. - ROSEN's Emergency Medicine
Step 7 - HR Still <60 After Compressions → Epinephrine ± Volume Expansion
Epinephrine:
| Route | Concentration | Dose |
|---|---|---|
| IV/IO (preferred) | 1:10,000 | 0.01-0.03 mg/kg |
| Endotracheal (less reliable) | 1:10,000 | 0.05-0.1 mg/kg (higher dose) |
- Give IV/IO rapidly; repeat every 3-5 minutes if HR remains <60
- Endotracheal route has unreliable absorption and is a last resort
Volume expansion (if suspected blood loss/hypovolemia):
- Normal saline, lactated Ringer's, or PRBCs
- 10 mL/kg IV over 5-10 minutes
If HR persistently <60: consider pneumothorax, hypovolemia.
Special Situations
Meconium-Stained Amniotic Fluid
Current NRP guidelines no longer recommend routine intubation and tracheal suctioning for all meconium-stained deliveries. Tracheal suctioning via ETT is only indicated if:
- Meconium is present AND
- Infant has poor tone, poor respiratory effort, or HR <100 bpm after 1 minute of appropriate PPV
Vigorous infants with meconium-stained fluid should be treated like any other newborn. - ROSEN's Emergency Medicine
Preterm Infants
- Initiate resuscitation with 21-30% FiO2 (not room air alone, not 100% O2)
- Use plastic wrap/bag to prevent hypothermia (do not dry first for <32 weeks)
- Lower ventilation pressures (20-25 cm H2O)
- Higher risk of respiratory distress syndrome - early surfactant considerations
Threshold of Viability
Infants born at 22-25 weeks pose ethical challenges. Decisions about resuscitation should incorporate gestational age, birth weight, parental wishes, and institutional capability.
Discontinuing Resuscitation
- If no cardiac activity for >10 minutes despite adequate resuscitative efforts, discontinuing resuscitation is reasonable
- Decisions should be individualized, with input from the team and family - Tintinalli's Emergency Medicine
Post-Resuscitation Complications
Common complications to monitor for after resuscitation:
- Hypoglycemia (check glucose early)
- Transient tachypnea of the newborn
- Meconium aspiration syndrome
- Pneumothorax
- Electrolyte disturbances
- Severe hyperbilirubinemia
- Sepsis
- Intraventricular hemorrhage (in preterm)
For infants who required chest compressions/CPR at birth, therapeutic hypothermia should be considered if they meet criteria for hypoxic-ischemic encephalopathy (HIE).
2025 AHA/AAP Guideline Update
The 2025 AHA/American Academy of Pediatrics guidelines (PMID: 41122887, Circulation, October 2025) represent the most current update, superseding the 2020 guidelines. Key changes from earlier versions include refinements in oxygen management, ECG monitoring recommendations, and approaches to threshold-of-viability resuscitation.
Sources:
- ROSEN's Emergency Medicine, Ch. 159
- Tintinalli's Emergency Medicine, Ch. 108
- Barash Clinical Anesthesia, 9e, Ch. 41
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- AHA/AAP 2025 Neonatal Resuscitation Guidelines [PMID: 41122887]
This is a shared conversation. Sign in to Orris to start your own chat.