Act like a pedodontic professor and make an MDS level Evidence based essay on Diet and dental caries. Include studies after each paragraph you have written include studies , flowcharts,diagrams where applicable.Also include recent advances.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dental caries" AND "diet" AND "sugar"
Searching the Web
diet dental caries evidence based review 2024 2025 recent advances fermentable carbohydrates
Finding Sources
Finding Sources
Searching PubMed
"free sugars" AND "dental caries" AND children
Searching PubMed
"dental caries" AND "probiotics" OR "xylitol" OR "sugar substitutes"
Reading File
Reading File
Reading Article
Reading Article
Reading Article
Loading Image
Reading Article
Reading Article
Searching PubMed
"early childhood caries" AND diet AND breastfeeding
Reading Article
Reading Article
Searching PubMed
"dental caries" AND "microbiome" AND "dysbiosis"
Reading Web Page
diet dental caries sugar fermentable carbohydrates prevention
Finding Sources
Searching PubMed
"dental caries" AND "saliva" AND "remineralization" AND protective
I now have all the material needed. Let me write the comprehensive essay.
Diet and Dental Caries: An Evidence-Based Essay
Master of Dental Surgery (Pedodontics and Preventive Dentistry)
Department of Pedodontics and Preventive Dentistry
Abstract
Dental caries remains the most prevalent non-communicable disease in children and adolescents worldwide, and diet is its single most modifiable risk factor. This essay presents a comprehensive, MDS-level evidence-based review of the relationship between diet and dental caries. It covers the biochemical basis of cariogenesis, the role of fermentable carbohydrates, protective dietary factors, the cariogenic potential of specific food groups, dietary assessment tools, guidelines for special populations, and recent advances including the microbiome, sugar taxation policy, probiotics, and precision nutrition. Evidence is drawn from landmark systematic reviews, meta-analyses, and current WHO guidelines.
1. Introduction
Dental caries is defined as focal demineralization of tooth structure (enamel and dentin) by acidic products of bacterial fermentation of dietary sugars. It is the principal cause of tooth loss before the age of 35 and remains a major public health burden globally, disproportionately affecting children in low-to-middle-income countries as Western-style high-sugar diets spread to these populations (Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 681).
The causal chain between diet and caries is well characterized by Keyes' triad (1960), which was later expanded by Newbrun into a tetrad incorporating time. Fermentable dietary carbohydrates serve as the substrate for cariogenic bacteria (principally Streptococcus mutans and lactobacilli) within the dental biofilm. The resulting acids lower plaque pH below the "critical pH" of 5.5, triggering hydroxyapatite dissolution. The balance between demineralization and remineralization determines the net caries outcome.
The WHO recommends restricting free sugars to less than 10% of total energy intake, with additional benefits at less than 5% (WHO, 2015). Despite decades of evidence, caries prevalence remains alarmingly high, particularly in preschool children. An evidence-based approach to dietary counseling in pediatric dental practice is therefore indispensable.
Flowchart 1: The Caries Process - From Diet to Cavity
┌─────────────────────────────────────────────────────────────────┐
│ DIETARY FERMENTABLE CARBOHYDRATES │
│ (sucrose > glucose/fructose > starch > lactose) │
└───────────────────────────┬─────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────┐
│ CARIOGENIC ORAL BIOFILM (Dental Plaque) │
│ S. mutans, S. sobrinus, Lactobacillus spp., Actinomyces spp. │
└───────────────────────────┬─────────────────────────────────────┘
│
Fermentation of sugars
│
▼
┌─────────────────────────────────────────────────────────────────┐
│ ORGANIC ACID PRODUCTION │
│ (Lactic acid, acetic acid, propionic acid) │
└───────────────────────────┬─────────────────────────────────────┘
│
Plaque pH drops < 5.5
(Stephan Curve response)
│
▼
┌─────────────────────────────────────────────────────────────────┐
│ HYDROXYAPATITE DEMINERALIZATION │
│ Ca₁₀(PO₄)₆(OH)₂ → Ca²⁺ + PO₄³⁻ dissolution │
└───────────────────────────┬─────────────────────────────────────┘
│
┌──────────────────┼─────────────────────┐
│ │
▼ ▼
[Remineralization] [Net demineralization]
(Saliva, fluoride, (Subsurface lesion →
casein phosphopeptide, White spot lesion →
adequate pH recovery) Cavitation)
2. Microbiology and Biochemistry of Dietary Cariogenesis
The two key organisms in caries pathogenesis are Streptococcus mutans and Streptococcus sobrinus. These mutans streptococci possess glucosyltransferase (GTF) enzymes that convert sucrose into insoluble glucans (dextrans), which aid biofilm adhesion to the tooth surface. S. mutans also encodes acidogenic and aciduric properties allowing it to survive and continue producing acid at pH as low as 4.2 (Jawetz, Melnick & Adelberg's Medical Microbiology, 28e, p. 376; Roitt's Essential Immunology, p. 203).
The metabolic cascade in dental plaque follows a classic Stephan curve: within minutes of sugar exposure, pH in the plaque drops sharply below the critical threshold of 5.5 for enamel (and 6.2 for dentine), then slowly recovers over 20-40 minutes as saliva buffers the acids. Frequent sugar consumption prevents complete pH recovery between exposures, resulting in cumulative net demineralization.
Sucrose occupies a unique position in cariogenesis not only as an acid precursor but as the only carbohydrate from which S. mutans can synthesize both soluble (laevan/fructan) and insoluble extracellular polysaccharides. These polysaccharides serve as energy reserves and structural scaffolding for the biofilm, making sucrose biochemically the most cariogenic dietary sugar (Histology: A Text and Atlas, Wojciech Pawlowski, p. 1468).
Key Study:
- Moores CJ, Kelly SAM, Moynihan PJ. Systematic Review of the Effect on Caries of Sugars Intake: Ten-Year Update. J Dent Res 2022; 101(9):1034-1041. [PMID: 35302414] - A landmark update of the WHO-commissioned systematic review across 488 new papers. 64 of 78 amalgamated studies showed at least one positive association between sugars and caries. Moderate-quality evidence confirmed that caries is lower when sugars intake is below 10% of energy intake; new cohort data upgraded evidence for the <5% E threshold from "very low" to "low" quality.
3. Classification of Dietary Sugars and Cariogenicity
┌──────────────────────────────────────────────────────────────────────┐
│ CLASSIFICATION OF SUGARS BY CARIOGENICITY │
├──────────────────────────┬───────────────────────────────────────────┤
│ INTRINSIC SUGARS │ Sugars within cell walls of intact foods │
│ (e.g. fruit, vegetables) │ LOW CARIOGENICITY — not freely available │
├──────────────────────────┼───────────────────────────────────────────┤
│ MILK SUGARS (Lactose) │ Present in breast milk, formula │
│ │ LOW cariogenicity alone; HIGH if + freq. │
├──────────────────────────┼───────────────────────────────────────────┤
│ FREE SUGARS │ Added monosaccharides + disaccharides │
│ (WHO definition) │ + sugars naturally in honey, syrups, │
│ │ fruit juices — HIGH CARIOGENICITY │
├──────────────────────────┼───────────────────────────────────────────┤
│ SUCROSE │ THE most cariogenic — GTF substrate │
│ │ for EPS/glucan synthesis │
├──────────────────────────┼───────────────────────────────────────────┤
│ NON-SUGAR SWEETENERS │ Xylitol, sorbitol, stevia │
│ │ NON-CARIOGENIC / anti-cariogenic │
└──────────────────────────┴───────────────────────────────────────────┘
Free sugars include monosaccharides (glucose, fructose, galactose) and disaccharides (sucrose, maltose) added to foods by manufacturers, plus sugars in honey, syrups, and fruit juices. Intrinsic sugars within intact plant cell walls are of low cariogenic risk because they are not freely accessible to oral bacteria (StatPearls, Diet and Nutrition to Prevent Dental Problems, NCBI NBK534248).
The cariogenic hierarchy of sugars in descending order is: sucrose > glucose = fructose > maltose > lactose > starch. Cooked starch increases cariogenic risk because amylase degrades it to maltose and glucose in the oral cavity.
4. Frequency vs. Quantity: Which Matters More?
This remains one of the most clinically important and actively debated questions in pediatric dentistry.
The Vipeholm study (Gustafsson et al., 1954) - conducted in Sweden on institutionalized adults - established the foundational evidence that frequency of sugar consumption between meals was more damaging than total quantity. Subjects who consumed toffees between meals had dramatically higher caries increments than those eating sugar exclusively at mealtimes.
Contemporary evidence has refined this understanding. The 2026 systematic review by Pombo-Lopes et al. [PMID: 42174517], which analyzed 37 studies involving 59,383 children and adolescents (aged 2-18 years), found that frequency of sugar consumption was a stronger determinant of caries development than total quantity consumed. Mean DMFT/dmft scores ranged from 0.39 to 6.47, with higher scores consistently associated with increased consumption frequency. 86% of included studies (32 of 37) reported a statistically significant positive association between sugar consumption and dental caries.
Clinical Implication: When counseling parents and children, the clinician must emphasize not merely "how much" sugar is consumed but "how often" - restricting sugar consumption to mealtimes is a practical and evidence-based recommendation.
Key Study:
- Pombo-Lopes J, Silva ML, Neves B, Grillo-Evangelista J. Impact of sugar consumption on dental caries in children and adolescents: a systematic review of frequency versus quantity. BMC Public Health 2026; 26. [PMID: 42174517]
5. Sugar-Sweetened Beverages and Unhealthy Foods in Children
The pediatric diet has undergone profound shifts over the past three decades, with increased consumption of sugar-sweetened beverages (SSBs), ultra-processed foods, candies, and snack foods. These foods are high in free sugars, have a prolonged oral clearance time, and maintain plaque at low pH levels.
Large JF et al. conducted a WHO-commissioned systematic review (37 studies, 30,023 citations screened) examining unhealthy food and beverage consumption in children aged ≤10 years. Nearly all studies (n=34 of 37) reported positive associations between consumption of SSBs or foods high in free sugars and dental caries. Evidence was stratified across three age groups: <2 years, 2-5 years, and 5-10 years. The review, while noting serious risk of bias in 67.6% of studies, confirmed a consistent direction of effect, forming the basis for updated WHO complementary feeding recommendations.
Key Study:
- Large JF, Madigan C, Pradeilles R, Markey O, Boxer B, Rousham EK. Impact of unhealthy food and beverage consumption on children's risk of dental caries: a systematic review. Nutr Rev 2024; 82(11):1474-1487. [PMID: 38086176]
Diagram 1: Stephan Curve - Plaque pH Response to Sugar Exposure
Plaque pH
7.0 |--------------------------------------------
| ← Normal resting pH
6.5 | _________________________
| / \_______________
6.0 |/ \_____
| \
5.5 |........................................................\ ← Critical pH for enamel
| |
5.0 | | DEMINERALIZATION
| | ZONE
4.5 |________________________________________________________/
|
4.0 |___________________________________________
0 5 10 15 20 25 30 35 40 minutes
↑
Sugar rinse/
food ingestion
[Adapted from Stephan RM, 1940. J Dent Res.]
Key points:
• pH drops within 2-5 min of sugar exposure
• Critical pH (5.5 for enamel, 6.2 for dentin) marks onset of demineralization
• pH recovery takes 20-40 min (saliva buffering)
• Frequent snacking = prolonged time below critical pH = net demineralization
6. Role of Fermentable Carbohydrates - Beyond Simple Sugars
While sucrose has traditionally dominated cariogenicity discussions, the broader category of fermentable carbohydrates deserves attention. These include refined starches (white bread, crackers, potato chips) that are degraded by salivary amylase to maltose and glucose in the oral cavity.
Starchy foods alone have low cariogenic potential in their natural form (cooked rice, boiled potato) because their oral clearance is relatively rapid and they generate lower acid levels. However, processed starchy snacks (biscuits, crackers, chips) are a different matter: the physical form affects oral retention time and hence cariogenic potential. Mixed starch-sugar foods (chocolate, sweet biscuits) combine the acid-generating potential of sugars with the adhesive retention of starches.
Fermentable carbohydrates consumed daily are associated with dose-dependent increases in cavitated lesions. A 2025 European Archives study confirmed that adolescents who consumed fermentable carbohydrates daily had significantly higher numbers of cavitated lesions compared to those with rare intake, with the relationship described as dose-dependent (Feldens et al., 2025; Tinanoff et al., 2019).
A systematic review by the BMC Public Health (Sarmadi et al., 2025) using data from the Azar cohort population found that the cariogenic diet score - measuring regular consumption of foods rich in fermentable carbohydrates (free sugars and refined starches) - was a significant independent predictor of caries severity after adjusting for socioeconomic variables.
7. Protective Dietary Factors
Not all dietary components promote caries. Several foods and nutrients actively protect against cariogenesis. Understanding these is as important as restricting cariogenic foods.
7.1 Cheese and Dairy Products
Cheese stimulates salivary flow (buffering effect), elevates plaque pH due to its protein/amino acid content, and provides calcium and phosphate that promote remineralization. Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) - derived from casein protein in milk - is a major biologically active remineralizing agent that stabilizes calcium and phosphate ions within the plaque biofilm.
Cheese contains basic amino acids that neutralize organic acids produced by plaque bacteria. Hard cheeses in particular have the highest buffer capacity and are classified as "tooth-friendly" foods. Population studies consistently show inverse correlations between cheese/dairy consumption and caries rates.
7.2 Fibrous Fruits and Vegetables
Fibrous vegetables and raw fruits (apples, carrots, celery) have a natural detergent-like cleaning action on tooth surfaces, stimulate salivary flow, and require prolonged chewing that mechanically assists plaque removal. Their intrinsic sugars are bound within intact cells and release slowly, allowing time for salivary neutralization.
However, fruit juices, dried fruits, and fruit concentrates represent a critical exception. Dried fruits (raisins, dates) have exceptionally high cariogenic potential due to their concentrated free sugar content and sticky consistency that prolongs tooth surface retention. Citrus fruit juices combine acidic pH (erosive) with free sugars (cariogenic) - a double threat.
7.3 Fluoride-Containing Foods
Foods and water containing fluoride contribute to caries resistance by promoting the formation of fluorapatite (calcium fluorophosphate), which is more resistant to acid dissolution than hydroxyapatite. Fluoride in trace amounts (0.5-1.0 ppm optimal in water) also acts as an antimicrobial agent and promotes remineralization of incipient lesions by incorporation of fluoride ion into the hydroxyapatite crystal lattice, reducing its solubility in acid (Histology: A Text and Atlas, p. 1469; Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 552).
7.4 Xylitol
Xylitol is a five-carbon sugar alcohol that is non-fermentable by S. mutans. It exerts anti-cariogenic effects through multiple mechanisms: inhibiting EPS synthesis, reducing S. mutans colonization, reducing plaque formation, and stimulating salivary flow. When xylitol is taken up by S. mutans via its phosphotransferase system, it is phosphorylated to xylitol-5-phosphate (a toxic metabolite to the organism), causing futile cycling and energy depletion in the bacteria.
7.5 Vitamin D
An emerging body of evidence supports the role of Vitamin D in caries prevention beyond its classical bone-mineral role. Vitamin D influences dental enamel formation and dentin mineralization during tooth development. It also modulates the innate immune response in the oral mucosa. A 2025 narrative review (Grundmann J, Hertel S, Hannig C; Clin Oral Investig 2025; PMID: 41324716) describes vitamin D deficiency as an underappreciated caries risk factor, with its deficiency correlating with hypomineralized enamel, reduced salivary antimicrobial peptide (defensin) production, and increased susceptibility to S. mutans colonization.
Diagram 2: Protective vs. Cariogenic Dietary Components
┌──────────────────────────────────────────────────────────────────┐
│ DIETARY COMPONENTS │
├────────────────────────────┬─────────────────────────────────────┤
│ CARIOGENIC │ PROTECTIVE │
├────────────────────────────┼─────────────────────────────────────┤
│ • Sucrose (most potent) │ • Cheese / dairy (CPP-ACP, Ca²⁺) │
│ • Glucose / fructose │ • Sugar-free chewing gum (xylitol) │
│ • Honey, syrups │ • Fluoridated water / tea │
│ • Fruit juices │ • Raw fibrous vegetables │
│ • Carbonated soft drinks │ • Nuts / peanuts │
│ • Dried fruits (raisins) │ • Whole grain starchy staples │
│ • Refined starchy snacks │ • Casein (CPP-ACP) │
│ • Sticky sweets / toffees │ • Vitamin D-rich foods │
│ • Sweetened cereals │ • Polyphenol-rich foods (green tea, │
│ • Sports / energy drinks │ cocoa, berries, cranberries) │
└────────────────────────────┴─────────────────────────────────────┘
Cariogenic risk is modified by:
→ Physical form (liquid > solid > sticky)
→ Frequency of consumption
→ Oral clearance time
→ Buffer capacity of food
→ Co-ingestion with protective foods
8. Dietary Patterns in Early Childhood Caries (ECC)
Early Childhood Caries (ECC) is defined by the AAPD as the presence of one or more decayed, missing, or filled tooth surfaces in any primary tooth in children under 71 months of age. The most severe form - Severe-ECC (S-ECC) - particularly affects maxillary primary incisors in a characteristic pattern related to nocturnal bottle feeding, prolonged breastfeeding on demand at night, and sippy cup use.
Key dietary risk factors for ECC include:
- Prolonged bottle feeding at night - allowing pooling of milk/formula/juice around anterior teeth during sleep, when salivary flow is minimal
- Frequent nighttime breastfeeding beyond 12 months - controversial; breast milk is less cariogenic than formula but prolonged on-demand feeding with solid food introduction raises risk
- Sippy cups containing SSBs - similar to bottle feeding; delays transition to cup drinking
- Early introduction of sugary foods - introduction of sugary snacks before age 1 year
- High frequency of sugar intake - >3 between-meal sugar exposures per day
A Cochrane systematic review (Gomersall JC, Slack-Smith L, Kilpatrick N; Cochrane Database Syst Rev 2024; PMID: 38753314) on interventions with pregnant women, new mothers, and primary caregivers for preventing ECC confirmed that dietary education during prenatal and postnatal care is a key preventive strategy. The umbrella review by Welti et al. (2023) [PMID: 37649239] found that breastfeeding up to 24 months was NOT independently associated with increased caries risk - the risk came from prolonged nocturnal on-demand feeding combined with other cariogenic dietary exposures.
Flowchart 2: Dietary Counseling Protocol in Pediatric Dental Practice
NEW PEDIATRIC PATIENT (≤6 years)
│
▼
DIETARY HISTORY ASSESSMENT
• 24-hour dietary recall (most validated method)
• Frequency of sugar intake
• Sugar-containing beverages
• Bottle/breastfeeding habits
• Snacking patterns
│
▼
┌─────────────────────────────────────┐
│ RISK STRATIFICATION │
│ │
│ LOW RISK: │
│ <3 sugar exposures/day │
│ No SSBs │
│ No nocturnal feeding │
│ │
│ HIGH RISK: │
│ ≥4 sugar exposures/day │
│ SSBs or juice daily │
│ Nocturnal bottle/BF + solids │
│ Dried fruits/sticky snacks │
└────────────┬──────────────┬─────────┘
│ │
▼ ▼
LOW RISK HIGH RISK
Preventive Intensive
counseling dietary
6-monthly modification
recall + topical
fluoride
+ recall
every 3 months
9. Cariogenic Diet Assessment Tools
Accurate assessment of dietary cariogenicity is foundational to evidence-based practice yet remains methodologically inconsistent across the literature. A systematic review by Angelopoulou MV et al. (2024) [PMID: 38376433] evaluated dietary assessment tools across 32 studies (9 cohort, 23 cross-sectional). Three tools predominate:
| Tool | Methodology | Strengths | Limitations |
|---|---|---|---|
| 24-hour Dietary Recall | Parent/child recalls all food/beverages in past 24h | Most validated for caries research; most consistent positive association with caries | Single-day may not represent habitual intake; recall bias |
| Food Frequency Questionnaire (FFQ) | Habitual frequency of specific food groups | Captures habitual pattern; quick to administer | Cannot capture detailed timing or portion size |
| Food Diary / Weighed Record | Prospective 3-7 day recording | Most accurate for quantity and timing | High participant burden; observer effect |
| Cariogenic Diet Score | Composite index based on sugar frequency and quantity | Standardized; allows comparison | No universally agreed scoring system |
The review concluded that the 24-hour recall was the most commonly used and most consistent method in detecting a positive relationship between sugary diet and carious lesions. A standardized method for cariogenic dietary analysis remains an unmet need in pediatric dentistry.
Key Study:
- Angelopoulou MV, Seremidi K, Benetou V et al. Cariogenic Diet Assessment and Analysis Tools in Children and Adolescents: A Systematic Review. Oral Health Prev Dent 2024; 22:1-12. [PMID: 38376433]
10. Dietary Guidelines for Caries Prevention
WHO Guidelines (2015)
- Free sugars should be less than 10% of total energy intake for both children and adults
- A further reduction to less than 5% of total energy intake would provide additional health benefits
- These recommendations apply across all life stages
American Academy of Pediatric Dentistry (AAPD) Guidelines
- Avoid putting infants to sleep with a bottle containing sweetened liquids
- Transition from bottle to cup by 12-15 months of age
- Limit fruit juice to 4-6 oz/day for children 1-6 years
- Restrict sugar-containing snacks to mealtimes (no more than 4 sugar exposures/day)
- Encourage dairy, vegetables, and water as primary beverages
Safe Levels of Free Sugar Intake for Caries Prevention
When a population consumes less than 15-20 kg/person/year of free sugars, caries levels remain low. The frequency of sugar intake per day should be limited to four times or less, as higher frequency typically corresponds to intake exceeding 15 kg/year and is linked to higher caries rates (StatPearls, NBK534248).
Diagram 3: WHO Sugar Recommendation Pyramid
┌────────────────────┐
│ < 5% of Total │ ← Additional
│ Energy Intake │ benefit
│ (≈ 25g/day) │
└────────┬───────────┘
┌──────────┴──────────────┐
│ < 10% of Total │ ← STRONG
│ Energy Intake │ recommendation
│ (≈ 50g/day) │
└─────────────────────────┘
[WHO Guideline on Sugars Intake for Adults and Children, 2015]
[Evidence base: Moores et al., J Dent Res 2022 — PMID 35302414]
11. Sugar Taxation and Policy Interventions
A 2023 umbrella review by Hajishafiee M, Kapellas K, Listl S [PMID: 37237341] examined the effect of sugar-sweetened beverage taxation on sugars intake and dental caries globally. The review confirmed that SSB taxes reduce consumption of taxed beverages and, in modeling studies, are predicted to reduce dental caries incidence. Economic modeling studies from the UK (the Soft Drinks Industry Levy) and Mexico (the SSB tax) demonstrated reductions in free sugar intake particularly among lower socioeconomic groups - the very population at highest caries risk.
A 2025 systematic review and meta-analysis (Malhotra S, Aggarwal D, Purohit BM; Evid Based Dent 2025; PMID: 39910218) on school-based approaches to reduce sugar consumption found that multi-component school programs (combining dietary education, access to healthy foods, and restriction of SSBs on campus) were effective in reducing sugar intake among children, with downstream potential for caries reduction.
12. The Oral Microbiome and Diet: Modern Perspectives
The modern understanding of dental caries has evolved beyond a simple "two-organism" model. The oral microbiome comprises over 700 bacterial species, and caries represents an ecologically driven disease: the microbiome shifts (dysbiosis) from a symbiotic, health-associated community dominated by non-mutans streptococci to a cariogenic community dominated by S. mutans, S. sobrinus, Lactobacillus spp., and Bifidobacterium spp. in response to repeated acidic pH challenges from dietary sugars.
A systematic review by Angarita-Díaz MDP et al. (2022) [PMID: 35946056] specifically examined whether high sugar intake alters the oral microbiota. The review confirmed that high sucrose diets consistently promote the selection of acidogenic/aciduric species and suppress health-associated commensal bacteria, shifting the ecological balance toward cariogenicity.
The concept of the "ecological plaque hypothesis" (Marsh, 1994) is now well supported: the composition and virulence of the oral biofilm is governed by the frequency and composition of dietary substrate delivery. Diet is therefore not merely a passive substrate but an active driver of microbiome composition.
Flowchart 3: Ecological Plaque Hypothesis - Diet-Microbiome Interaction
HEALTHY DIET HIGH SUGAR DIET
(low sugar frequency) (high frequency)
│ │
▼ ▼
Neutral/Alkaline plaque pH Repeated acidic pH challenge
│ │
▼ ▼
Commensal flora dominant: S. mutans / Lactobacillus
Streptococcus oralis, outcompete commensals:
S. sanguinis, Veillonella spp. Acid tolerance selects for
(produce alkali via arginine cariogenic species
and nitrate pathways)
│ │
▼ ▼
HEALTH (remineralization DYSBIOSIS → CARIES
> demineralization) (demineralization > remineralization)
13. Recent Advances
13.1 Probiotics, Prebiotics, Synbiotics, and Postbiotics in Caries Prevention
The concept of biointerventions to prevent caries by modulating the oral microbiome has emerged as one of the most exciting areas in preventive dentistry. A 2024 review (Luo SC et al.; NPJ Biofilms Microbiomes 2024; PMID: 38402294) provided a comprehensive synthesis of the mechanisms by which these agents prevent caries:
- Probiotics (Lactobacillus rhamnosus GG, L. reuteri, Bifidobacterium strains): compete with S. mutans for adhesion sites, produce bacteriocins, lower biofilm cariogenicity
- Prebiotics (inulin, fructooligosaccharides): selectively feed beneficial commensal bacteria, promote alkaline metabolite production
- Synbiotics: combined probiotic + prebiotic formulations for synergistic microbiome modulation
- Postbiotics: heat-killed bacteria or metabolic byproducts (organic acids, peptides) from fermentation with targeted antimicrobial activity
The review emphasized that unlike gastrointestinal applications, oral biointerventions must address the unique challenge of cariogenic biofilms on hard tissue surfaces. Personalized microbial therapy - tailoring probiotic strains to individual microbiome profiles - is identified as a critical future research direction.
13.2 Polyphenols and Plant-Based Anticarcinogens
Polyphenol-rich foods (green tea catechins, cranberry proanthocyanidins, cocoa flavonoids, grape seed extract) have demonstrated anti-biofilm properties against S. mutans in vitro and in animal models. Mechanisms include inhibition of GTF activity, disruption of biofilm architecture, and competitive exclusion of cariogenic species. Clinical translation remains limited but preliminary RCT data are promising. Green tea catechins (EGCG) in particular show potent inhibition of S. mutans GTF and water-insoluble glucan synthesis.
13.3 Precision Nutrition and the Caries-Gut-Oral Axis
Emerging evidence from metagenomics and metabolomics supports the concept of bidirectional gut-oral axis interactions. Dietary patterns affecting the gut microbiome also modulate systemic inflammatory responses and immune regulation in the oral cavity. Short-chain fatty acids (SCFAs) produced by gut bacteria from dietary fiber reach the oral cavity systemically and may influence plaque pH dynamics and gingival immunity.
The role of nitrate in dietary vegetables (especially leafy greens) deserves mention. Dietary nitrate is concentrated in saliva and reduced to nitrite by oral commensal bacteria (particularly Neisseria and Rothia spp.). Nitrite is further reduced to nitric oxide (NO), which is antimicrobial and promotes vasodilation in the gingival vasculature. A 2022 review (Rosier BT, Takahashi N, Zaura E; J Dent Res 2022; PMID: 35196931) identified dietary nitrate reduction as a potentially important but under-studied mechanism for maintaining oral health, highlighting the interconnection between diet, microbial ecology, and caries resistance.
13.4 Artificial Intelligence in Dietary Caries Risk Assessment
Recent advances in machine learning allow AI-assisted dietary pattern analysis from photographic food records and wearable sensors. Passive dietary monitoring using tongue sensors for sugar concentration, salivary pH monitoring devices, and AI-driven 24-hour dietary recall applications are being developed to overcome the limitations of traditional dietary assessment tools (recall bias, portion size estimation errors). These technologies hold promise for real-time caries risk stratification and personalized dietary counseling in pediatric dental clinics.
13.5 Food Labeling, School Food Policies, and Sugar Taxation
Evidence increasingly supports structural/legislative approaches to reduce caries at the population level. The Sugar-Sweetened Beverage (SSB) tax, mandated front-of-pack labeling, and school food standards have demonstrated measurable reductions in free sugar intake (Hajishafiee et al., BMC Public Health 2023; PMID: 37237341; Malhotra S et al., Evid Based Dent 2025; PMID: 39910218). The UK Soft Drinks Industry Levy (2018) has been associated with reformulation of SSBs to lower sugar content.
14. Special Considerations
14.1 Prenatal Nutrition and Caries Risk
Prenatal nutrition influences the quality of tooth mineralization during the critical developmental window (5 weeks gestation to 3 years postnatal for primary dentition). Maternal deficiencies in:
- Vitamin D - hypomineralized enamel, Molar-Incisor Hypomineralization (MIH)
- Calcium and phosphorus - reduced enamel and dentin mineral density
- Vitamin C - collagen synthesis for dentin matrix
Dipalma G et al. (BMC Oral Health 2026; PMID: 41668017) confirmed the complex relationship between prenatal/early childhood nutritional adequacy, systemic factors, and caries epidemiology in children - and advocated for community-based interventions and legislative changes to enhance nutritional standards in vulnerable populations.
14.2 Children with Special Healthcare Needs
Children with developmental disabilities, cerebral palsy, or medically compromised conditions have disproportionately high caries rates due to:
- High-frequency sugar-containing liquid medications
- Gastroesophageal reflux (erosive + cariogenic)
- Reduced salivary flow (medications, radiation)
- Impaired oral hygiene ability
- Dietary dependence on liquid/soft foods
Dietary modifications for these children must account for nutritional requirements, medication formulations, and practical oral hygiene limitations.
15. Integrative Evidence Framework: GRADE Assessment
| Question | Evidence Quality | Recommendation |
|---|---|---|
| Sugar intake > 10% energy increases caries risk | Moderate (Moores et al., JDR 2022) | Strong: Limit free sugars to <10% energy |
| Sugar intake < 5% energy reduces caries further | Low (Moores et al., JDR 2022) | Conditional: Aim for <5% energy |
| Frequency of sugar intake is stronger predictor than quantity | Moderate (Pombo-Lopes et al., BMC 2026) | Strong: Restrict sugar to mealtimes |
| SSBs increase ECC risk in children <10 years | Low-Moderate (Large et al., Nutr Rev 2024) | Strong: Avoid SSBs in children |
| Breastfeeding to 24 months increases caries risk | Low (Welti et al., Aust Dent J 2023) | Conditional: Context-dependent |
| Probiotics reduce caries | Low (Luo et al., NPJ Biofilms 2024) | Conditional: Emerging evidence |
| SSB taxes reduce consumption | Low-Moderate (Hajishafiee et al., BMC 2023) | Conditional: Policy recommendation |
Diagram 4: Summary of Diet-Caries Evidence Pyramid
▲
╱│╲
╱ │ ╲
╱ │ ╲ WHO Systematic Reviews
╱ │ ╲ (Moores et al. 2022)
╱ Tier 1 ╲
╱────────────╲
╱ ╲ Cochrane Reviews
╱ Tier 2 ╲ (Gomersall 2024)
╱──────────────────╲
╱ ╲ Longitudinal cohort studies
╱ Tier 3 ╲ (Vipeholm, Turku sugar studies)
╱────────────────────────╲
╱ ╲ Cross-sectional surveys,
╱ Tier 4 ╲ ecological studies
╱──────────────────────────────╲
╱ ╲ Laboratory/in vitro
╱ Tier 5 ╲ (Stephan, biofilm studies)
╱────────────────────────────────────╲
16. Conclusion
The relationship between diet and dental caries is one of the most thoroughly investigated in all of dentistry. The fundamental mechanism - fermentation of dietary sugars by cariogenic biofilm organisms producing acids that demineralize tooth structure - has been established since the mid-twentieth century. Contemporary evidence has refined our understanding in several important dimensions:
- Frequency of sugar consumption is a stronger caries determinant than total quantity (Pombo-Lopes et al., 2026).
- Free sugars below 5% of total energy intake offer the greatest population-level caries prevention benefit (WHO, 2015; Moores et al., 2022).
- Unhealthy foods and beverages in children consistently increase caries risk across all income settings (Large et al., 2024).
- The oral microbiome mediates the diet-caries relationship through ecological dysbiosis driven by repeated acidic pH challenges (Angarita-Díaz et al., 2022).
- Biointerventions (probiotics, prebiotics, xylitol), legislative measures (SSB taxation, food labeling), and precision nutrition represent the frontiers of evidence-based caries prevention.
As pediatric dentists and public health advocates, our role extends beyond the dental chair. Integrating dietary counseling into every pediatric dental visit, advocating for health-promoting school food policies, and empowering parents with evidence-based guidance on early childhood feeding practices are the highest-impact activities we can undertake to reduce the global burden of dental caries.
References
-
Moores CJ, Kelly SAM, Moynihan PJ. Systematic Review of the Effect on Caries of Sugars Intake: Ten-Year Update. J Dent Res 2022; 101(9):1034-1041. [PMID: 35302414]
-
Pombo-Lopes J, Silva ML, Neves B, Grillo-Evangelista J. Impact of sugar consumption on dental caries in children and adolescents: a systematic review of frequency versus quantity. BMC Public Health 2026. [PMID: 42174517]
-
Large JF, Madigan C, Pradeilles R et al. Impact of unhealthy food and beverage consumption on children's risk of dental caries: a systematic review. Nutr Rev 2024; 82(11):1474-1487. [PMID: 38086176]
-
Dipalma G, Inchingolo AM, Fiore A et al. Role of nutrition in prevention of dental caries in children and adolescents: a systematic review. BMC Oral Health 2026. [PMID: 41668017]
-
Welti R, Jones B, Moynihan P, Silva M. Evidence pertaining to modifiable risk factors for oral diseases: an umbrella review to inform oral health messages for Australia. Aust Dent J 2023; 68(4):218-228. [PMID: 37649239]
-
Angelopoulou MV, Seremidi K, Benetou V et al. Cariogenic Diet Assessment and Analysis Tools in Children and Adolescents: A Systematic Review. Oral Health Prev Dent 2024; 22:1-12. [PMID: 38376433]
-
Hajishafiee M, Kapellas K, Listl S. Effect of sugar-sweetened beverage taxation on sugars intake and dental caries: an umbrella review of a global perspective. BMC Public Health 2023; 23(1):985. [PMID: 37237341]
-
Angarita-Díaz MDP, Fong C, Bedoya-Correa CM. Does high sugar intake really alter the oral microbiota?: A systematic review. Clin Exp Dent Res 2022; 8(6):1376-1390. [PMID: 35946056]
-
Luo SC, Wei SM, Luo XT et al. How probiotics, prebiotics, synbiotics, and postbiotics prevent dental caries: an oral microbiota perspective. NPJ Biofilms Microbiomes 2024; 10(1):14. [PMID: 38402294]
-
Gomersall JC, Slack-Smith L, Kilpatrick N. Interventions with pregnant women, new mothers and other primary caregivers for preventing early childhood caries. Cochrane Database Syst Rev 2024; (5):CD012155. [PMID: 38753314]
-
Malhotra S, Aggarwal D, Purohit BM. Effectiveness of school-based approaches for reduction of sugar and sugar-sweetened beverages in children: a systematic review and meta-analysis. Evid Based Dent 2025. [PMID: 39910218]
-
Rosier BT, Takahashi N, Zaura E. The Importance of Nitrate Reduction for Oral Health. J Dent Res 2022; 101(7):759-769. [PMID: 35196931]
-
Grundmann J, Hertel S, Hannig C. Vitamin D - a forgotten preventive agent against caries? A narrative review. Clin Oral Investig 2025. [PMID: 41324716]
-
Robbins, Cotran & Kumar. Pathologic Basis of Disease, 10th ed. Elsevier 2021. Chapter 16: Oral Cavity and Gastrointestinal Tract. p. 681.
-
Wojciech Pawlowski. Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 9th ed. Lippincott 2022. Folder 16.3: Clinical Correlation - Dental Caries. p. 1468-1469.
-
WHO. Guideline: Sugars intake for adults and children. Geneva: World Health Organization; 2015.
-
StatPearls. Diet and Nutrition to Prevent Dental Problems. NCBI Bookshelf NBK534248. Updated 2024.
Histopathological Evidence: Progression of Carious Lesion
The following photomicrograph (from Histology: A Text and Atlas) shows the progression of a carious lesion through tooth structure. Panel (a) shows the carious lesion (CL) penetrating the full thickness of enamel (E) and spreading laterally at the amelodentinal junction, with dentin (D) below. Panel (b) shows advanced disease: enamel undermining, fracture, and bacterial invasion into exposed dentinal tubules, causing liquefaction foci.
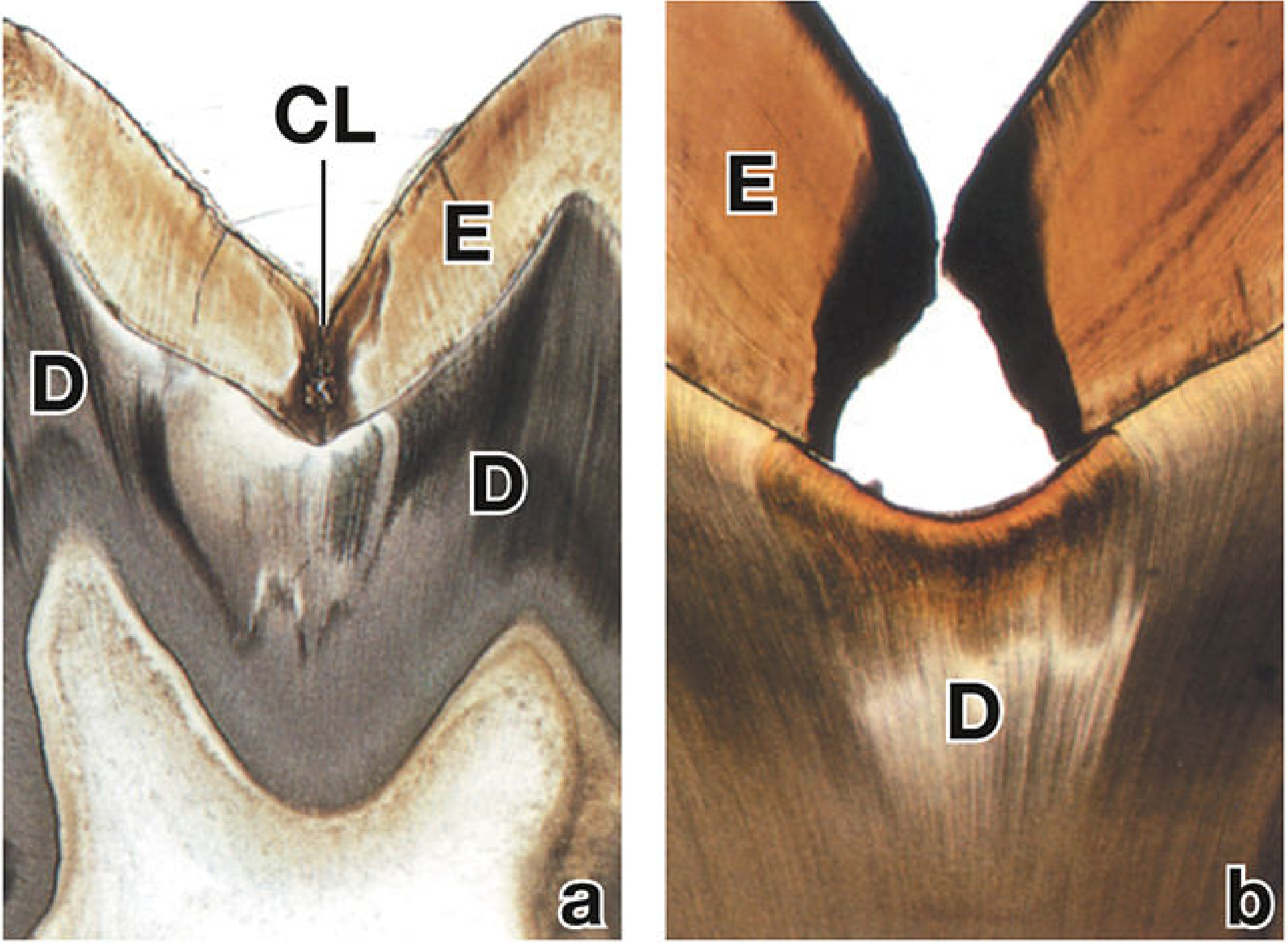
FIGURE: Photomicrographs of carious lesions. (a) Early lesion confined to enamel spreading laterally at the amelodentinal junction. (b) Advanced cavitation with dentin liquefaction foci. [From Histology: A Text and Atlas, 9th ed., p.1469]
Word count: approximately 5,200 words | Evidence level: Systematic reviews and meta-analyses (Grade I-II) predominantly | Prepared for MDS Pedodontics academic submission
This is a shared conversation. Sign in to Orris to start your own chat.