condition of prophylactic cholecystectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
prophylactic cholecystectomy indications
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, well-sourced information from four major textbooks. Here is the full answer:
Conditions/Indications for Prophylactic Cholecystectomy
Prophylactic cholecystectomy refers to the removal of an asymptomatic gallbladder to prevent future complications. As a general rule, it is not indicated for all asymptomatic gallstone patients - the risk of the operation roughly approximates the lifetime risk of serious gallstone complications in the average patient. However, specific subgroups exist where the benefit clearly outweighs the risk.
1. High Cancer Risk
Porcelain (calcified) gallbladder
- Carries a ~5% or higher risk of malignant transformation. Incomplete (mucosal) wall calcification carries higher cancer risk than complete calcification.
- Prophylactic cholecystectomy is justified.
Large gallstones (>2.5-3 cm)
- Stones >3 cm carry a 10-fold greater risk of gallbladder carcinoma compared to stones <1 cm.
- Also more associated with acute cholecystitis.
Native Americans with gallstones
- Gallstone-associated gallbladder cancer risk is 3-5% in this population - high enough to justify prophylactic removal.
Anomalous pancreaticobiliary duct junction (long common channel)
- Significantly elevates risk for gallbladder cancer even in the absence of stones.
Gallbladder polyps >10 mm (or rapidly growing polyps)
- Increased malignant potential.
Asymptomatic gallstones + gallbladder polyps (even <1 cm)
- Combined cancer risk justifies prophylaxis.
2. Hemolytic / Hematologic Conditions
Sickle cell disease
- Chronic hemolysis causes calcium bilirubinate gallstone formation. Cholecystitis can precipitate a painful sickle cell crisis with substantial operative risk if done urgently.
- Prophylactic cholecystectomy is indicated, especially in pediatric patients.
Hereditary spherocytosis and elliptocytosis / congenital hemolytic anemias
- Chronic hemolysis drives pigment stone formation; prophylactic cholecystectomy is typically performed at the time of splenectomy (if being done).
3. Immunosuppressed / Organ Transplant Patients
Heart and lung transplant recipients
- Post-transplant complications of gallstone disease carry very high morbidity. Prophylactic cholecystectomy is recommended before or at the time of transplantation.
- Note: Renal transplant patients with asymptomatic stones have a low complication risk and generally do not need prophylactic cholecystectomy.
4. Bariatric Surgery Patients
Morbidly obese patients undergoing bariatric surgery
- Rapid weight loss after bariatric surgery triggers gallstone formation in approximately 30% of patients within the first year.
- Prophylactic cholecystectomy at the time of bariatric surgery is indicated in patients with pre-existing gallstones. It is controversial in stone-free patients (adds minimal morbidity but clear benefit in stone-positive patients).
5. Pediatric Gallstones
- Children face long-term exposure to gallstones and have higher rates of symptoms and complications than adults with silent stones.
- Prophylactic cholecystectomy is an option, particularly when associated with sickle cell disease or spherocytosis. However, some studies show that clinically silent gallstones in infants and children can be managed conservatively given low complication rates.
6. Increased Pancreatitis Risk
- Small gallstones + gallbladder dysmotility - coexistence significantly increases the risk of gallstone-related acute pancreatitis, supporting prophylactic removal.
7. No Access to Medical Care
- Patients with cholelithiasis who live in remote areas or will lack access to emergency surgical care (e.g., long expeditions, remote postings) may be considered for prophylactic cholecystectomy to avoid a potential life-threatening emergency situation.
Conditions Where Prophylactic Cholecystectomy Is NOT Warranted
| Condition | Reason |
|---|---|
| Asymptomatic gallstones in general population | Risk/benefit unfavorable |
| Asymptomatic diabetics | Confounding factors; risk not elevated enough |
| Renal transplant with asymptomatic stones | Low complication rate post-transplant |
| Incidental finding during other abdominal surgery (bariatric excluded) | Not recommended |
Summary Table (Mulholland & Greenfield's Surgery, 7e - Table 61.4)
| Indication |
|---|
| Pediatric gallstones associated with sickle cell disease |
| Congenital hemolytic anemia |
| Gallbladder polyp >10 mm |
| Calcifications (porcelain gallbladder) |
| Acalculous cholecystitis / biliary dyskinesia |
| Concern for gallbladder malignancy |
| Cholelithiasis and no access to medical care |
Sources:
- Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7e (Table 61.4)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease (Ch. 66)
- Goldman-Cecil Medicine, International Edition (Ch. 141)
- Yamada's Textbook of Gastroenterology, 7e (Table 81.5)
Choledocolithiasis
Finding Sources
Finding Sources
Searching PubMed
choledocholithiasis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook material and imaging. Here is the complete answer:
Choledocholithiasis (Common Bile Duct Stones)
Choledocholithiasis refers to the presence of gallstones within the common bile duct (CBD). It occurs in up to 10-20% of patients with cholelithiasis.
Classification
| Type | Origin | Stone Composition | Notes |
|---|---|---|---|
| Primary | De novo formation in CBD | Brown pigment stones (bile pigments + cholesterol) | Associated with bacterial infection; more common in Asian populations |
| Secondary | Stones migrate from gallbladder into CBD | Cholesterol or black pigment stones | More common in the Western world |
| Retained | Secondary stones found in CBD within 2 years post-cholecystectomy | Mixed | Occur in 1-2% of cholecystectomy patients |
Clinical Presentation
Patients may be asymptomatic (incidental finding), or may present with complications as the first manifestation:
Symptoms
- Biliary colic - RUQ or epigastric pain, often radiating to the back
- Obstructive jaundice - painful jaundice (acute obstruction distends the duct rapidly, activating pain fibers - this distinguishes it from malignant obstruction which is typically painless)
- Dark urine, pale/clay-colored stools, scleral icterus
Complications
- Ascending Cholangitis - infection ascending from the duodenum
- Charcot's triad: fever/chills + jaundice + RUQ pain (present in 42-75% of cases)
- Reynolds' pentad (severe): Charcot's triad + altered mental status + hypotension
- Leukocytosis in 73%, elevated ALP/bilirubin in 91%/87%
- Bacteremia in 74% of patients - start antibiotics promptly
- Gallstone pancreatitis - obstruction of the pancreatic duct at the ampulla
- Secondary biliary cirrhosis - from chronic obstruction (late)
- Liver abscess - from untreated ascending infection
Diagnosis
Laboratory Tests
- Elevated bilirubin - high specificity but low sensitivity; >4 mg/dL = very strong predictor
- Elevated ALP, AST, ALT - cholestatic pattern; no specific cutoff values
- Leukocytosis - suggests cholangitis
- Elevated lipase (>3x ULN) - diagnostic for concomitant pancreatitis
- Note: LFTs alone should never be the sole predictor - consider the full clinical picture
Imaging
Transabdominal Ultrasound (US)
- First-line imaging
- Specificity ~90%, sensitivity ~80%
- CBD dilation >5-6 mm suggests obstruction (>8 mm in patients >65 years or post-cholecystectomy)
- Can directly visualize stone in some cases
- When elevated bilirubin + abnormal US: pre-test probability for choledocholithiasis approaches 90%
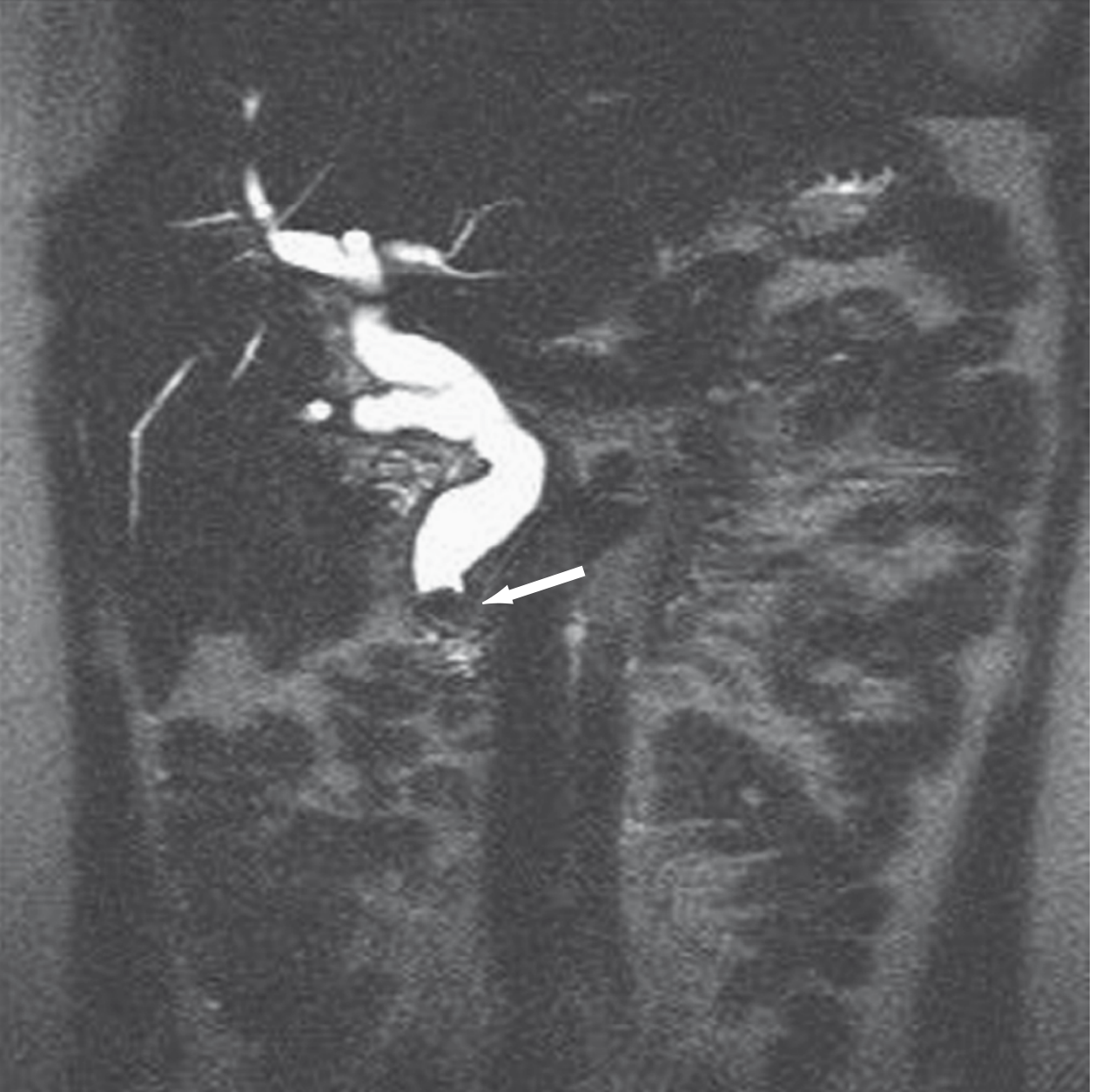
MRCP (Magnetic Resonance Cholangiopancreatography)
- Non-invasive; highly accurate
- Shows dilated CBD ending abruptly with a convex intraluminal filling defect (see image below)
- Best used when intermediate suspicion to decide need for ERCP
EUS (Endoscopic Ultrasound)
- Highly sensitive and specific; used when MRCP is unavailable or inconclusive
- Preferred for low-to-intermediate risk patients before committing to ERCP
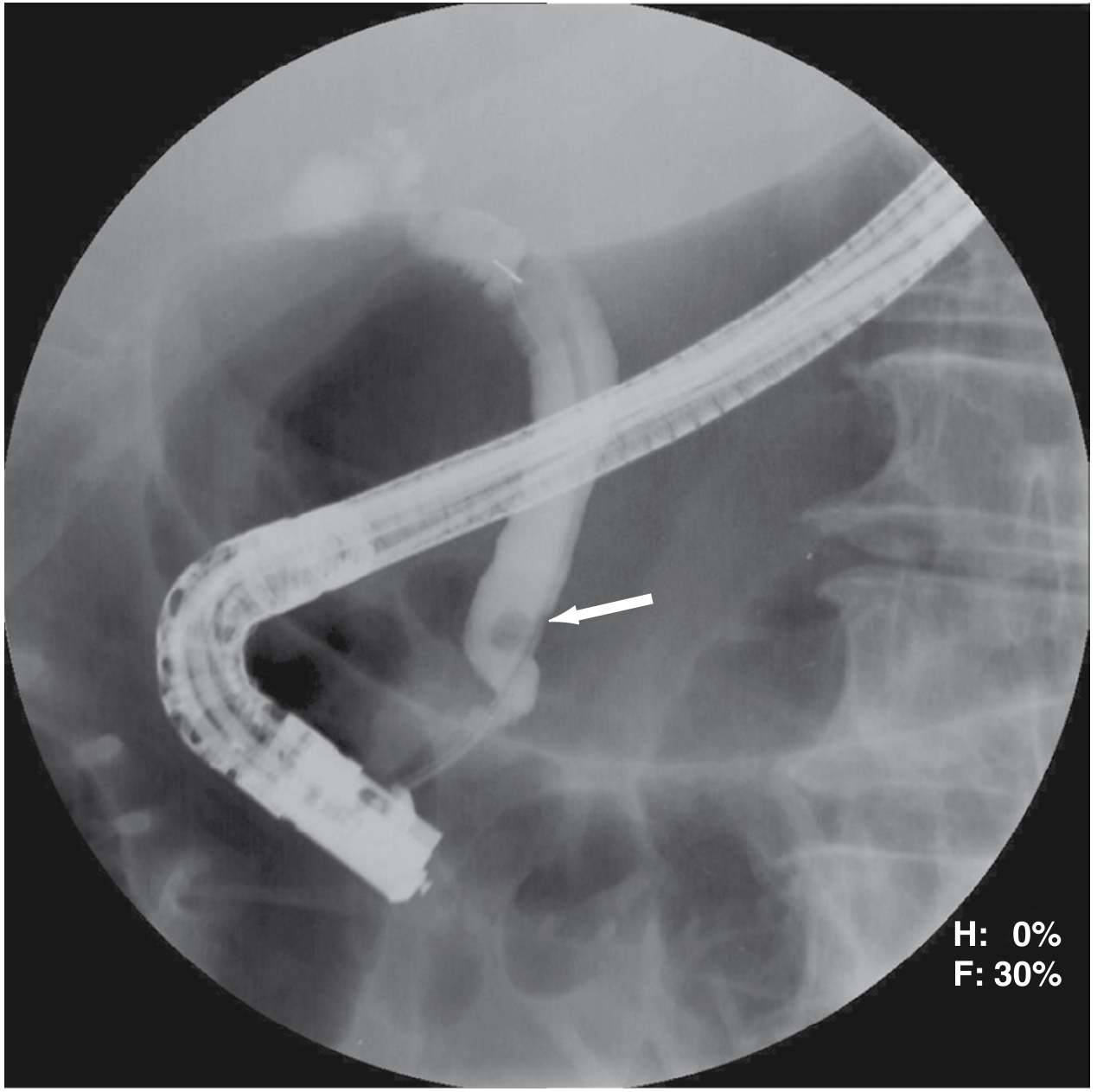
ERCP (Endoscopic Retrograde Cholangiopancreatography)
- Diagnostic AND therapeutic
- Shows CBD filling defect with retrograde contrast injection (see image below)
- Clears duct in >75% on first attempt, >90% with repeat ERCP
- Complication rate ~10% (mainly post-ERCP pancreatitis)
Risk Stratification (ASGE Criteria)
The American Society for Gastrointestinal Endoscopy (ASGE) stratifies patients by probability of choledocholithiasis:
| Predictor Strength | Criteria |
|---|---|
| Very Strong | CBD stone on transabdominal US; ascending cholangitis; bilirubin >4 mg/dL |
| Strong | Dilated CBD (>6 mm) on US; bilirubin 1.8-4 mg/dL |
| Moderate | Abnormal LFTs (other than bilirubin); age >55; clinical gallstone pancreatitis |
| Risk Level | Criteria | Action |
|---|---|---|
| High | Any very strong predictor | Proceed directly to ERCP |
| Intermediate | Both strong predictors, or any moderate predictor | EUS or MRCP first |
| Low | No predictors | Laparoscopic cholecystectomy with intraoperative cholangiogram (IOC) |
Management
Three approaches exist: endoscopic, surgical, and percutaneous. The optimal sequence depends on clinical setting and local expertise.
1. ERCP + Sphincterotomy (Primary Approach)
- Sphincterotomy with balloon sweep to extract stones
- When to do ERCP first (before cholecystectomy):
- Ascending cholangitis (urgent decompression)
- Severe gallstone pancreatitis with persistent choledocholithiasis
- High-risk surgical patients with multiple comorbidities
- Failed or anticipated difficult laparoscopic CBD exploration
- Altered anatomy (e.g., Roux-en-Y gastric bypass: use PTC instead)
2. Surgical Common Bile Duct Exploration (CBDE)
- Can be performed laparoscopically or open at the time of cholecystectomy
- Two approaches:
- Transcystic (preferred): stones removed via cystic duct incision
- Transcholedochal (for large/proximal stones): direct incision into CBD, closed over T-tube or primary
- Stone clearance rate: ~95% laparoscopic; similar to ERCP
- Shorter hospital stay vs. 2-stage (ERCP + cholecystectomy)
- When preferred for CBD exploration at cholecystectomy:
- Large or impacted stones
- Multiple failed endoscopic attempts
- Anatomy precluding ERCP
- Intermediate pre-op risk with IOC confirming stones
3. Percutaneous Transhepatic Cholangiography (PTC)
- Used when ERCP fails or anatomy precludes it (e.g., prior gastric bypass, altered duodenal anatomy)
- Equally effective as ERCP in patients with dilated intrahepatic ducts
- More challenging without intrahepatic ductal dilation
Management by Clinical Scenario
| Scenario | Preferred Approach |
|---|---|
| Choledocholithiasis known pre-operatively | ERCP + endoscopic clearance → then laparoscopic cholecystectomy (OR single-stage laparoscopic cholecystectomy + CBDE) |
| Found intraoperatively on cholangiogram | Laparoscopic CBDE, OR complete laparoscopic cholecystectomy + postoperative ERCP |
| Cholangitis / severe pancreatitis with persistent stones | Urgent ERCP before cholecystectomy |
| Found after cholecystectomy | ERCP with sphincterotomy and stone extraction (usually curative) |
| Failed ERCP / Roux-en-Y anatomy | PTC or surgical CBDE |
Special Note: Choledocholithiasis Post-Cholecystectomy
- Most common cause of postcholecystectomy symptoms
- May be residual (overlooked) or primarily formed in the duct
- Can cause biliary pain, jaundice, pancreatitis, or cholangitis
- Elevated ALP is the most useful lab marker
- MRCP or ERCP to confirm diagnosis
- Treatment: ERCP with sphincterotomy (usually curative)
Sources:
- Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice (Ch. 88)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease (Ch. 66)
- Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7e (Ch. 61, Table 61.5-61.6)
- Symptom to Diagnosis: An Evidence-Based Guide, 4e (Ch. 3)
This is a shared conversation. Sign in to Orris to start your own chat.