Causes of different murmers and their features
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is a full synthesis:
Heart Murmurs: Causes and Features
What Produces a Murmur?
Murmurs arise from audible turbulence due to:
- Accelerated flow through normal or abnormal orifices
- Flow through a narrowed/irregular orifice into a dilated vessel/chamber
- Backward (regurgitant) flow through an incompetent valve, VSD, or PDA
Grading (I–VI): Grade 1 = barely audible; Grade 3+ = loud (structurally significant); Grade 4+ = palpable thrill; Grade 5 = heard with stethoscope edge only; Grade 6 = heard off chest.
Murmur Timing Diagrams
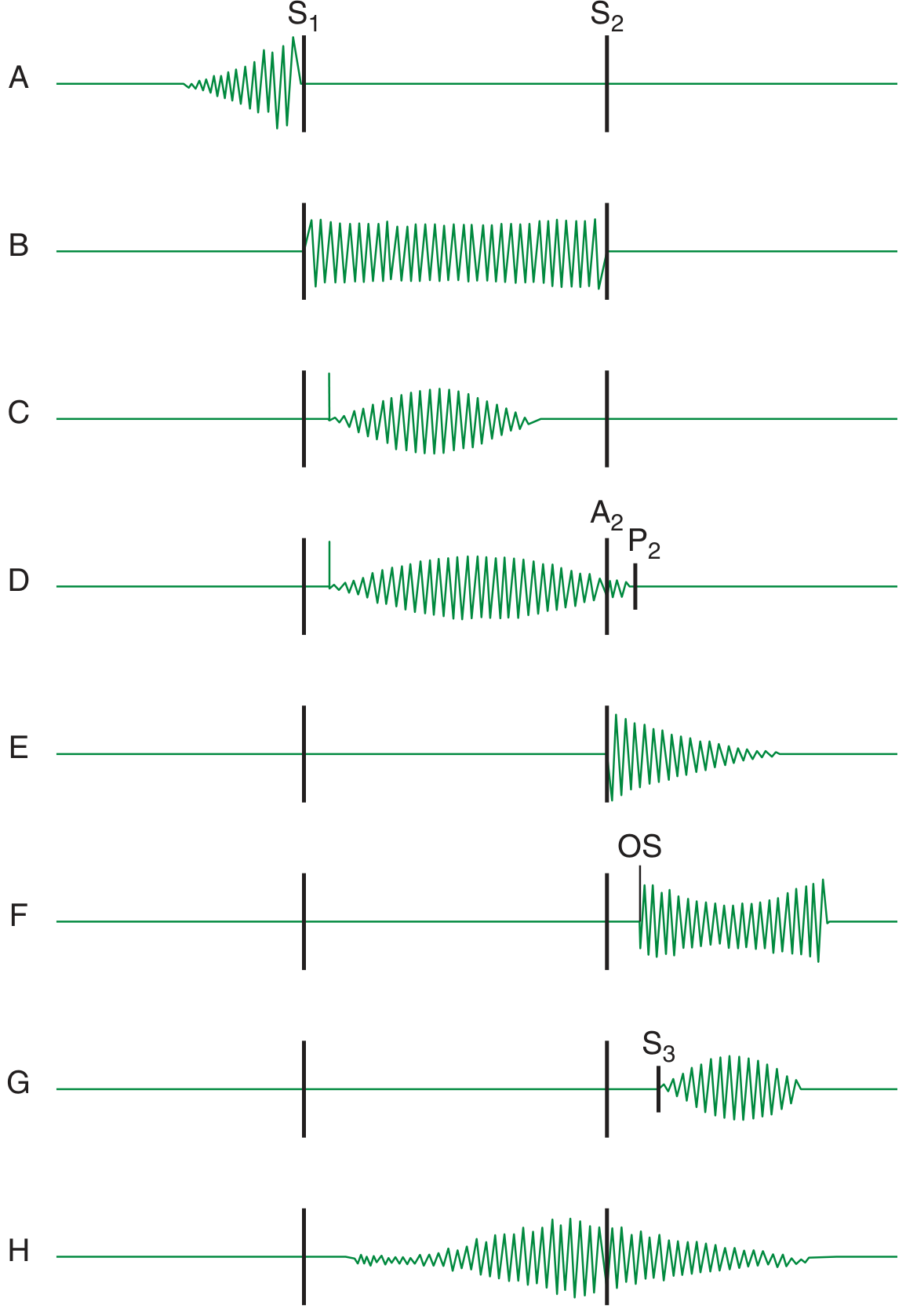
A = presystolic (MS/TS in sinus rhythm); B = holosystolic (MR/TR/VSD); C = ejection murmur with ejection click (AS); D = PS murmur spilling past A2; E = AR diastolic murmur; F = MS after opening snap; G = short mid-diastolic after S3; H = continuous murmur (PDA)
SYSTOLIC MURMURS
Mechanism Comparison
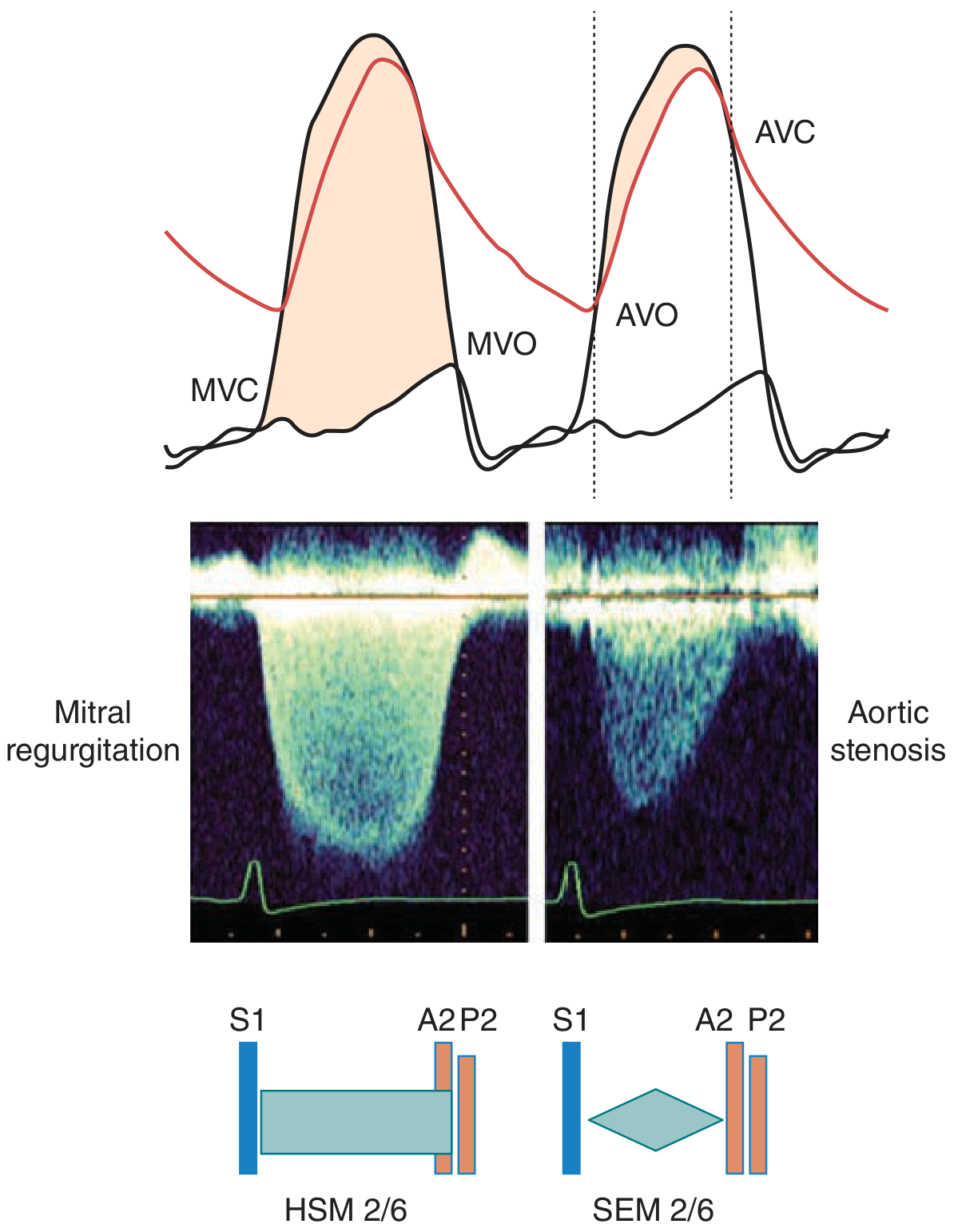
AV regurgitation (MR) → holosystolic plateau murmur from MVC to MVO. Semilunar valve obstruction (AS) → ejection murmur from AVO to AVC, with crescendo-decrescendo (diamond) shape.
1. Holosystolic (Pansystolic) Murmurs
Extend from S1 to S2 — caused by a sustained pressure gradient between two chambers throughout systole.
| Condition | Cause | Best Heard | Key Features |
|---|---|---|---|
| Mitral regurgitation (MR) | Mitral prolapse, rheumatic, flail leaflet, ischemia, dilated CMP | Apex | High-pitched, blowing, plateau quality; radiates to axilla (posterior jet) or LSB (anterior jet). "Honking" quality in MVP. |
| Tricuspid regurgitation (TR) | Functional RV dilation, endocarditis, carcinoid | Lower LSB | Increases with inspiration (Carvallo's sign); regurgitant CV waves in JVP |
| VSD (large) | Congenital / acquired | LSB 3rd–4th ICS | Harsh; loud (grade 4–5) in small restrictive VSDs; becomes limited to early systole if pulmonary HTN develops |
2. Early Systolic Murmurs
Begin at S1, end before midsystole.
| Condition | Cause | Features |
|---|---|---|
| Acute severe MR | Papillary muscle rupture, chordal tear | Early decrescendo; into a normal-sized, non-compliant LA; best heard medial to apex |
| Small muscular VSD | Congenital; defect closes during contraction | Localized to LSB, grade 4–5; absent signs of pulmonary HTN |
| TR with normal PA pressure | Infective endocarditis | Soft (grade 1–2), LSB, increases with inspiration; no right heart failure signs |
3. Midsystolic (Ejection) Murmurs
Begin after S1, end before S2 — crescendo-decrescendo shape.
| Condition | Cause | Best Heard | Key Features |
|---|---|---|---|
| Aortic stenosis (AS) | Calcific (elderly), bicuspid AV, rheumatic | Right 2nd ICS → carotids | Harsh, radiates to carotids; Gallavardin effect (purer/higher at apex); associated with slow-rising pulse, narrow PP, absent A2 in severe disease |
| Pulmonic stenosis (PS) | Congenital | Left 2nd ICS | Preceded by ejection click; murmur peaks later and spills past A2; wide split S2; P2 delayed/soft |
| HOCM | Dynamic LV outflow obstruction | LSB / apex | Increases with Valsalva and standing (reduced preload); decreases with squatting; does NOT radiate to carotids |
| Aortic sclerosis | Thickened non-obstructive AV leaflets | Right 2nd ICS | Grade 1–2; normal A2; no carotid radiation; normal carotid upstroke |
| High-flow states | Anemia, fever, pregnancy, hyperthyroidism, AV fistula | Variable | Soft, grade 1–2, no associated abnormal heart sounds |
| ASD | Increased flow across PV | Left 2nd ICS | Fixed wide split S2 is the key finding; murmur itself is often soft |
4. Late Systolic Murmurs
| Condition | Cause | Features |
|---|---|---|
| Mitral valve prolapse (MVP) | Myxomatous degeneration | Preceded by a mid-systolic click; murmur moves earlier with standing/Valsalva (reduces preload, earlier prolapse); moves later with squatting |
DIASTOLIC MURMURS
1. Diastolic Rumbles (Low-pitched, best with bell)
| Condition | Cause | Best Heard | Key Features |
|---|---|---|---|
| Mitral stenosis (MS) | Rheumatic fever (most common) | Apex (left lateral decubitus) | Low-pitched, rumbling; opening snap (OS) precedes it; presystolic accentuation in sinus rhythm; duration ∝ severity |
| Tricuspid stenosis (TS) | Rheumatic (usually with MS), carcinoid | Lower LSB | Rare; increases with inspiration |
| Austin-Flint murmur | Aortic regurgitation jet strikes anterior MV leaflet | Apex | Mid-diastolic rumble; mimics MS but no opening snap, no loud S1 |
| Flow rumble | Increased AV valve flow (severe MR/TR, ASD, VSD) | Apex or LSB | Due to volume overload causing relative stenosis across AV valve |
2. Diastolic Decrescendo Murmurs (High-pitched, use diaphragm)
| Condition | Cause | Best Heard | Key Features |
|---|---|---|---|
| Aortic regurgitation (AR) | Bicuspid AV, rheumatic, endocarditis, aortic root dilation, aortitis | Left sternal border (3rd ICS) | High-pitched blowing; heard leaning forward + breath held; murmur at right 2nd ICS → root dilation; duration and intensity ∝ severity. Wide pulse pressure, collapsing pulse, Corrigan's, water-hammer signs |
| Pulmonary regurgitation (PR) | Functional (pulmonary HTN) — Graham Steell murmur | Left 2nd ICS | Low-pitched (primary PR); high-pitched in Graham Steell (follows loud P2); increases with inspiration (differentiates from AR) |
CONTINUOUS MURMURS
Begin in systole, continue through S2 into diastole — caused by a persistent pressure gradient across both phases of the cardiac cycle.
| Condition | Notes |
|---|---|
| Patent ductus arteriosus (PDA) | Classic "machinery" murmur; loudest at left infraclavicular/2nd ICS; peaks at S2 |
| Ruptured sinus of Valsalva aneurysm | Sudden onset; aorta → RV/RA |
| Coronary/systemic AV fistula | Continuous over affected area |
| Cervical venous hum | Benign; disappears with neck compression or supine position |
| Mammary souffle of pregnancy | Benign; disappears with pressure on stethoscope |
| Aortopulmonary septal defect | Rare congenital |
| Pulmonary artery branch stenosis | Peripheral; radiates to both lung fields |
Summary: Key Differentiating Maneuvers
| Maneuver | Effect | Use |
|---|---|---|
| Valsalva / Standing | ↓ preload → louder HOCM/MVP; softer AS/MR | HOCM vs AS |
| Squatting | ↑ preload → softer HOCM/MVP; louder AS/MR | HOCM vs AS |
| Inspiration | ↑ right heart filling → louder TR, PR, TS | Right-sided murmurs |
| Handgrip | ↑ afterload → louder MR, AR; softer HOCM | MR vs HOCM |
| Leaning forward | Better transmission of AR | AR detection |
| Left lateral decubitus | Better MS detection | MS |
Sources: Harrison's Principles of Internal Medicine 22E, pp. 326–334; Fuster & Hurst's The Heart 15th Ed., pp. 95–100
Examination findings in aortic regurgitation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent — this is the key physical examination section. Now I have all the content needed. Let me compile the comprehensive answer:
Examination Findings in Aortic Regurgitation
Causes (for context)
| Valvular | Aortic Root | Combined |
|---|---|---|
| Bicuspid AV, rheumatic, infective endocarditis, calcific degeneration | Hypertension, Marfan syndrome, aortic dissection, syphilitic aortitis, Ehlers-Danlos, Takayasu, giant cell aortitis, atherosclerotic aneurysm | Bicuspid AV + root dilation, ankylosing spondylitis |
General Inspection
| Sign | Description |
|---|---|
| de Musset's sign | Head nodding/bobbing with each heartbeat — from large stroke volume |
| Awareness of heartbeat | Patient notices pounding in chest, especially supine on left side |
Pulse & Blood Pressure
| Sign | Description |
|---|---|
| Corrigan's pulse (water-hammer pulse) | Abrupt distension then rapid collapse of the arterial pulse; best felt by elevating the patient's arm and palpating the radial artery |
| Bisferiens pulse | Double-peak systolic pulse; best appreciated in the brachial and femoral arteries |
| Wide pulse pressure | Elevated systolic (increased stroke volume) + reduced diastolic (runoff into LV); e.g. 160/40 mmHg |
| Hill's sign | Popliteal systolic BP exceeds brachial by >20 mmHg in moderate AR, >60 mmHg in severe AR |
| Duroziez's sign | Systolic and diastolic bruit heard over the femoral artery when partially compressed with stethoscope |
| Müller's sign | Pulsation of the uvula |
| Quincke's sign | Capillary pulsation visible at the nail bed on gentle pressure |
| Traube's sign | "Pistol-shot" (booming systolic and diastolic sounds) over the femoral artery |
Note: Diastolic BP measured at phase IV Korotkoff (muffling), not disappearance, as sounds may persist to zero in severe AR.
Precordium
| Finding | Description |
|---|---|
| Displaced apex beat | Laterally and inferiorly displaced — reflecting LV dilation (cor bovinum in severe chronic disease) |
| Hyperdynamic apex | Diffuse, forceful, volume-overloaded character |
| Palpable rapid filling wave | Felt at apex |
| Systolic thrill | At the base of heart or suprasternal notch due to augmented stroke volume |
| Carotid shudder | Palpable vibratory sensation in the carotid arteries |
Auscultation
The Murmur
- Character: High-pitched, blowing, decrescendo diastolic murmur beginning immediately after A2
- Best heard: Sitting forward, leaning forward, breath held in deep expiration, using the diaphragm firmly at the left sternal border (3rd–4th ICS)
- Location clue:
- Left sternal border → primary valvular disease
- Right sternal border (upper) → aortic root dilation
- Severity correlates with duration (not intensity):
- Mild AR → early diastolic only, soft, high-pitched blowing
- Severe AR → holodiastolic, may have rough/musical quality
- "Cooing dove" or musical quality → eversion or perforation of an aortic cusp
- In severe AR with LV decompensation: late diastolic component disappears as LV and aortic pressures equalize
Other Auscultatory Findings
| Finding | Significance |
|---|---|
| Austin Flint murmur | Mid-diastolic/pre-systolic low-pitched apical rumble in severe AR — AR jet strikes anterior MV leaflet causing it to vibrate; mimics MS but without opening snap |
| Systolic ejection murmur (harsh, at base, radiating to carotids) | Due to greatly increased LV stroke volume and ejection rate — does not indicate concurrent AS; carotid palpation differentiates |
| S3 gallop | Indicates elevated LV end-diastolic volume; suggests impaired LV function in severe AR |
| Soft or absent A2 | Severe valvular AR (leaflet destruction) |
Summary: Key Named Signs
| Eponym | Sign |
|---|---|
| Corrigan's / water-hammer pulse | Collapsing pulse |
| de Musset's sign | Head bobbing |
| Duroziez's sign | Femoral double bruit |
| Hill's sign | Popliteal BP > brachial BP |
| Traube's sign | Pistol-shot femorals |
| Quincke's sign | Nail-bed capillary pulsation |
| Müller's sign | Uvular pulsation |
| Austin Flint murmur | Apical diastolic rumble (no MS) |
| Gallavardin effect (if concurrent AS) | Systolic murmur sounds purer at apex |
Acute vs Chronic AR — Key Differences on Exam
| Feature | Chronic AR | Acute AR (e.g. endocarditis, dissection) |
|---|---|---|
| Pulse pressure | Wide | May be normal/only mildly elevated |
| Apex beat | Displaced, hyperdynamic | Not displaced (LV not yet dilated) |
| Diastolic murmur | Long, holodiastolic | Short, early diastolic only (rapid LV/Ao pressure equalization) |
| S1 | Normal | Soft or absent (premature mitral valve closure) |
| Signs of LV failure | Late | Early and prominent (pulmonary oedema, shock) |
| Wide pulse pressure signs (Corrigan etc.) | Present | May be absent |
Sources: Braunwald's Heart Disease 11E, pp. 718–720; Fuster & Hurst's The Heart 15th Ed., pp. 97–98; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.