Respiratory failure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of respiratory failure drawn from authoritative pulmonary and critical care textbooks.
Respiratory Failure
Definition
Respiratory failure is characterized by inadequate blood oxygenation or carbon dioxide removal — specifically the failure of the respiratory system to meet tissue requirements for oxygen uptake and CO₂ elimination. Clinically, it is defined by arterial blood gas values. — Fishman's Pulmonary Diseases and Disorders
Classification
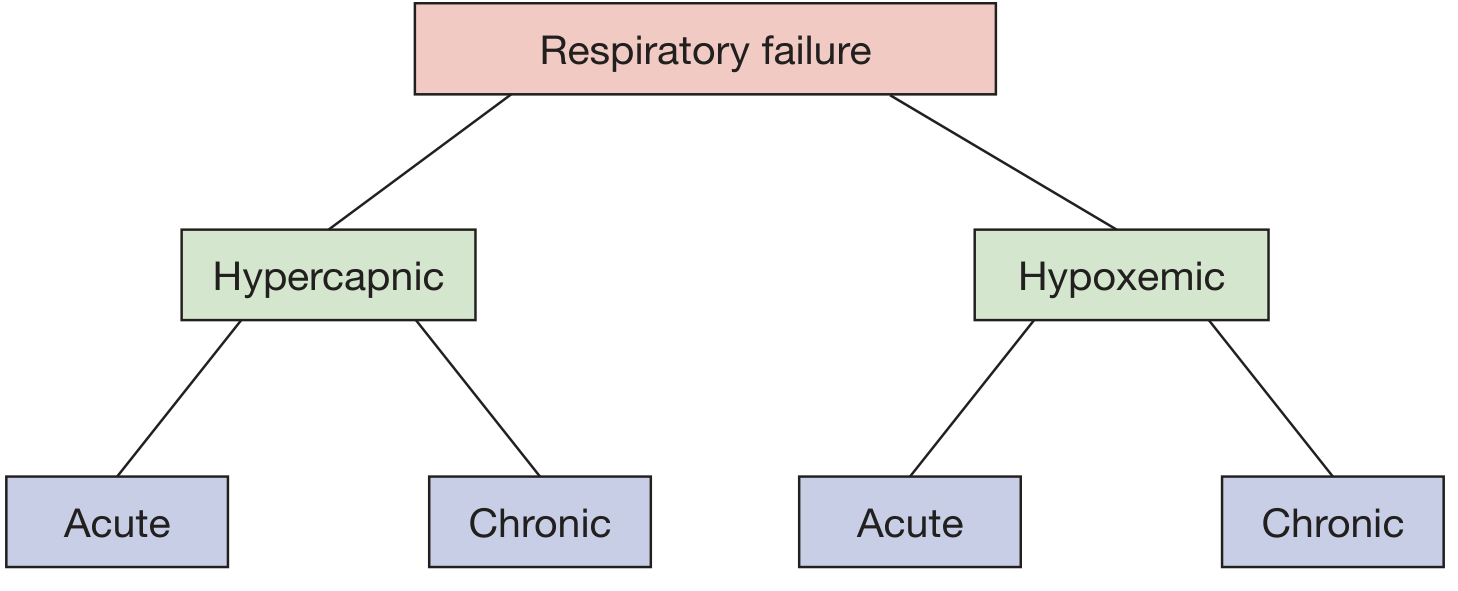
Respiratory failure is classified along two axes:
By Gas Exchange Abnormality
| Type | Definition | Key ABG Finding |
|---|---|---|
| Hypoxemic (Type 1) | Failure to oxygenate | PaO₂ < 60 mm Hg on room air |
| Hypercapnic (Type 2) | Failure to ventilate | PaCO₂ > 45–50 mm Hg |
| Postoperative (Type 3) | Atelectasis-driven; subset of Type 1/2 | Occurs post-surgery from pain/sedation |
| Shock-related (Type 4) | Metabolic demand exceeds respiratory capacity | e.g., sepsis, fever |
The two types frequently coexist — disorders initially causing hypoxemia may progress to pump failure and hypercapnia. — Washington Manual of Medical Therapeutics
By Time Course
| Acute | Chronic | |
|---|---|---|
| Hypercapnic | PaCO₂ >45 mmHg + acidemia (pH <7.30); develops in minutes to hours | Long-standing CO₂ retention with renal HCO₃⁻ compensation |
| Hypoxemic | Abrupt change in mental status; develops rapidly | Polycythemia, cor pulmonale as clues |
Pathophysiology
Respiratory failure can arise from any component of the respiratory pump or the alveoli:
Central Nervous System → Peripheral Nerves → Respiratory Muscles/Chest Wall → Airways → Alveoli
Defects in the first four (the "respiratory pump") tend to cause combined hypercapnia and hypoxemia; alveolar disorders initially cause predominantly hypoxemia. — Fishman's Pulmonary Diseases and Disorders
Mechanisms of Hypoxemia (Type 1)
| Mechanism | Examples | A-a Gradient | O₂ Response |
|---|---|---|---|
| V/Q Mismatch | COPD, pneumonia, PE, pulmonary edema | Elevated | Responds to O₂ |
| Shunt | Atelectasis, ARDS, ASD/VSD, pneumonia | Elevated | Minimal/no response |
| Diffusion limitation | Pulmonary fibrosis, pulmonary hypertension | Elevated | Responds to O₂ |
| Hypoventilation | CNS depression, neuromuscular disease | Normal | Responds to O₂ |
| Low inspired O₂ | High altitude | Normal | Responds to O₂ |
Causes of Hypercapnia (Type 2)
Hypercapnia follows the equation: PaCO₂ ∝ VCO₂ / VA — any decrease in alveolar ventilation (VA) or increase in dead space raises PaCO₂.
CNS ("won't breathe"): Opiate overdose, CNS infection, metabolic alkalosis, obesity-hypoventilation syndrome, meningoencephalitis, stroke
Neuromuscular ("can't breathe"): Guillain-Barré syndrome, myasthenia gravis, ALS, muscular dystrophies, spinal cord injury, pharmacologic paralysis
Chest wall/thoracic: Kyphoscoliosis, flail chest, morbid obesity, massive ascites, abdominal distension
Airway obstruction: COPD (most common), acute asthma, cystic fibrosis, epiglottitis, foreign body, tracheal tumor, bronchiolitis obliterans
Alveolar/parenchymal: Severe ARDS, extensive pneumonia, pulmonary edema — through increased dead space and ventilatory demand exceeding supply
Hypermetabolic states (increased CO₂ production): Sepsis, fever, thyrotoxicosis, seizures, serotonin syndrome
Severity Classification (in COPD Exacerbation)
| Severity | RR | Work of Breathing | Mental Status | Hypoxemia | PaCO₂ / pH |
|---|---|---|---|---|---|
| No failure | 20–30/min | Normal | Baseline | Mild, responds to NC | Normal |
| Acute RF | >30/min | Increased, accessory muscles | Baseline | Responds to <35% FiO₂ | 50–60 mmHg, pH >7.25 |
| Severe RF | — | — | Altered | Requires >35% FiO₂ | PaCO₂ >60 mmHg or pH ≤7.25 |
— Rosen's Emergency Medicine
Management Overview
Non-invasive Oxygen Therapy
| Device | FiO₂ Range | Notes |
|---|---|---|
| Nasal cannula | ~24–44% | +4% per L/min; max 6 L/min |
| Simple face mask | 35–55% | Min 5 L/min to flush CO₂ |
| Venturi mask | 24–50% | Precise FiO₂ control |
| Non-rebreather mask | Up to 80% | Reservoir bag with one-way valve |
| HFNC | Up to 100%, up to 60 L/min | Flushes dead space, small PEEP effect; reduces intubation need in hypoxemic RF |
Non-invasive Positive Pressure Ventilation (NPPV)
- CPAP (5–15 cm H₂O): Prevents alveolar collapse; used in pulmonary edema, OSA
- BiPAP: Reduces work of breathing; first-line for COPD exacerbation with acute hypercapnic RF (if cooperative and hemodynamically stable)
- BiPAP starting settings: IPAP 5–10 cm H₂O above EPAP; EPAP 5 cm H₂O
Invasive Mechanical Ventilation
Indicated when:
- Non-invasive methods fail
- Patient cannot protect airway
- Altered mental status
- Hemodynamic instability
- Acute hypercapnic RF with pH ≤7.25
ECMO
- VV ECMO: Severe hypoxemic RF (e.g., refractory ARDS) with intact cardiac function
- VA ECMO: Combined cardiac and respiratory failure
- Reserved for cases where conventional ventilation fails
— Washington Manual of Medical Therapeutics; Sabiston Textbook of Surgery; Murray & Nadel's Textbook of Respiratory Medicine
Key Distinguishing Points
- Shunt is the one cause of hypoxemia that does not respond to supplemental oxygen — a critical clinical discriminator
- Acute hypercapnia raises PaCO₂ abruptly with acidosis; chronic hypercapnia has a compensated (higher) bicarbonate with near-normal pH
- HFNC has shown mortality benefit over standard O₂ in hypoxemic non-hypercapnic RF (90-day mortality improvement)
- Obesity hypoventilation syndrome causes hypercapnia on a central basis — distinct from obstructive sleep apnea alone
ECMO detailed review
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
This is a shared conversation. Sign in to Orris to start your own chat.