Status epilepticus managment
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, high-quality content from multiple authoritative sources. Here is a structured, evidence-based summary of status epilepticus management.
Status Epilepticus: Management
Definition & Time-Based Classification
Status epilepticus (SE) is defined as:
- A single seizure ≥5 minutes, OR
- Two or more seizures without recovery of consciousness between them
The old 30-minute threshold has been replaced clinically because seizures persisting >5 minutes are unlikely to self-terminate, are harder to treat, and begin causing neuronal injury. Operationally:
| Phase | Duration | Action |
|---|---|---|
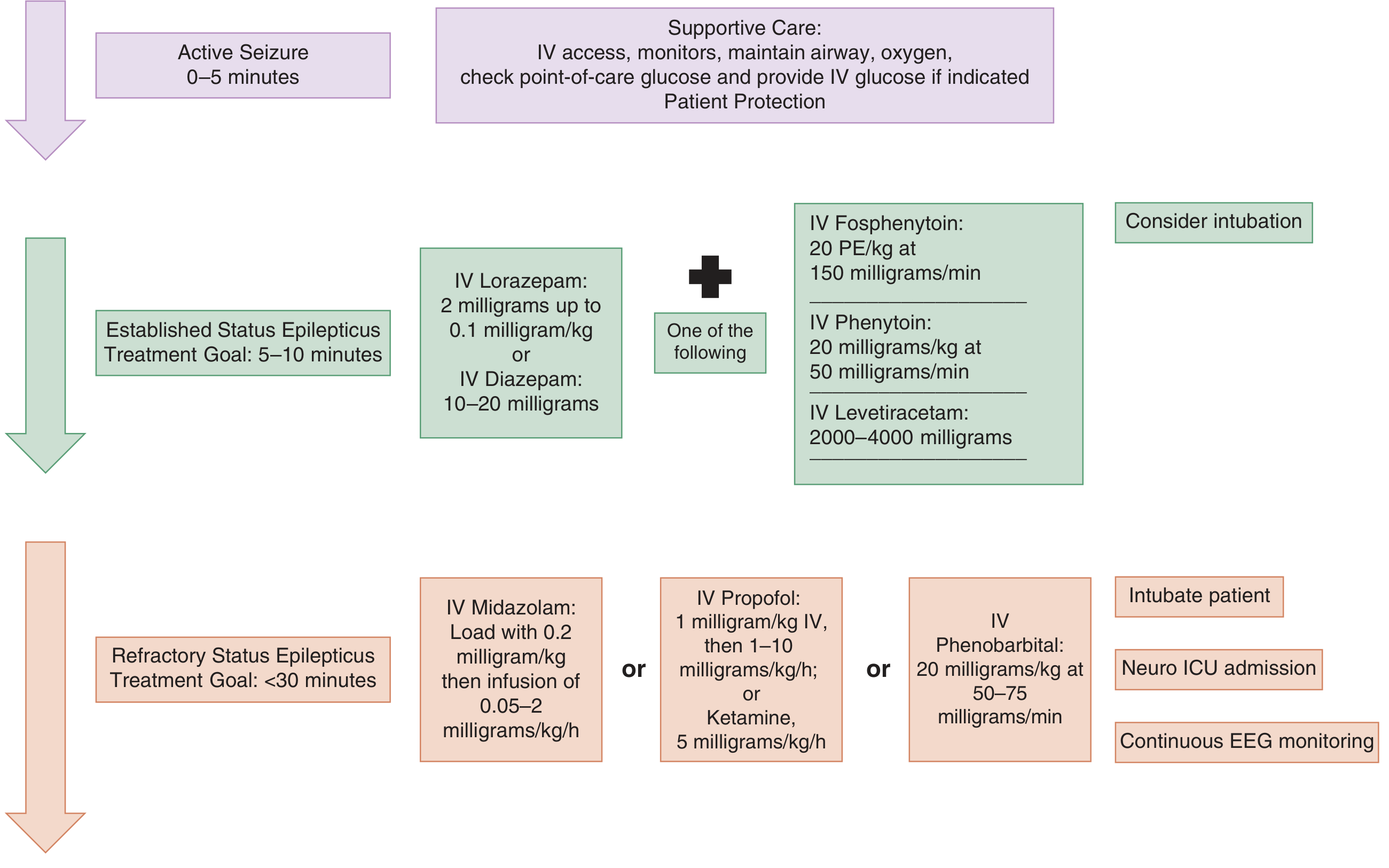
| Active seizure | 0–5 min | Supportive care, IV access, glucose check |
| Established SE | 5–30 min | 1st-line (BZDs) + 2nd-line agents simultaneously |
| Refractory SE (RSE) | >30 min despite 1st + 2nd line | 3rd-line: anesthetic infusions + intubation |
| Super-refractory SE | >24 h despite 3rd-line | Escalate: ketamine, inhaled anesthetics, non-pharmacologic |
Convulsive SE: Bilateral rhythmic jerking + impaired consciousness — immediate life threat.
Non-convulsive SE (NCSE): Fluctuating mental status, confusion, subtle motor signs (twitching, eye deviation) without overt convulsions — diagnosed by EEG.
Pathophysiology (Why Speed Matters)
After 5 minutes of seizure activity:
- GABA-A receptors are internalized (reduced expression)
- Glutamate / NMDA receptors are upregulated
- Blood-brain barrier breakdown → influx of K⁺ and albumin (both hyperexcitatory)
After 20 minutes: hypotension, hypoxia, metabolic acidosis, hyperthermia, hypoglycemia, cardiac arrhythmias, and pulmonary edema develop. Standard therapies become progressively less effective.
— Tintinalli's Emergency Medicine, p. 1199
Phase 1 — Immediate Stabilization (0–5 minutes)
- Airway: Position, suction, nasopharyngeal airway; avoid oral airway (risk of vomiting post-seizure)
- Breathing: Supplemental O₂; bag-valve mask if ventilation inadequate
- Circulation: Cardiac monitor, pulse oximetry, end-tidal CO₂
- IV/IO access: Large-bore IV or IO if IV unobtainable within 1–2 minutes
- Glucose: Bedside glucose immediately; give IV dextrose if hypoglycemic or uncertain
- Labs: BMP (Ca²⁺, Mg²⁺), CBC, LFTs, lactate, drug levels, toxicology screen, pregnancy test (if applicable)
- Treat hyperthermia: Antipyretics + cooling blankets
- Fluid: Normal saline — avoid dextrose-containing solutions (incompatible with phenytoin)
Phase 2 — First-Line Treatment: Benzodiazepines (5–10 minutes)
Benzodiazepines terminate seizures in ~70% of cases and are universally first-line.
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Lorazepam | IV | 0.1 mg/kg (up to 4–8 mg) at 2 mg/min | Preferred IV agent; less redistribution than diazepam |
| Midazolam | IM | 10 mg (adults) | Preferred if no IV — as effective as IV lorazepam in prehospital setting |
| Diazepam | IV | 0.2 mg/kg (5–10 mg) at 5 mg/min | Faster onset; shorter brain duration due to redistribution |
| Midazolam | Intranasal/buccal | Per weight | Alternative when IV/IO unavailable |
| Diazepam | Rectal | Per weight | Acceptable prehospital alternative |
If seizures persist after 5 minutes: give a second dose of benzodiazepine. Delays >10 minutes in starting BZDs are independently associated with higher mortality and longer seizure duration.
Phase 3 — Second-Line Agents (Established SE, ~10–30 minutes)
If seizures persist after adequate BZD dosing, load one of the following simultaneously:
| Drug | IV Dose | Rate | Notes |
|---|---|---|---|
| Levetiracetam | 30–60 mg/kg (up to 4,500 mg) | Over 10 min | Favored: fewest interactions, safe in liver disease |
| Fosphenytoin | 15–20 mg PE/kg | 150 mg PE/min | Water-soluble, can give IM; less cardiotoxic than phenytoin |
| Valproic acid | 30–40 mg/kg | 5 mg/kg/min | Avoid in liver disease, thrombocytopenia, metabolic disorders, pregnancy |
| Phenytoin | 20 mg/kg | 50 mg/min (max) | Cardiotoxic; requires cardiac monitoring; incompatible with dextrose |
| Phenobarbital | 10–20 mg/kg | 100 mg/min | Highly effective; severe sedation + respiratory depression limit use |
| Lacosamide | Variable | IV infusion | Newer option; ECG monitoring needed (PR prolongation/arrhythmia risk) |
Evidence note: Multiple RCTs (ESETT, ConSEPT, EcLiPSE) found levetiracetam, fosphenytoin/phenytoin, and valproate are equally effective (~45–50% seizure cessation) after BZD failure, with similar adverse effect profiles. Levetiracetam is increasingly preferred due to its safety profile. — Katzung's Basic & Clinical Pharmacology, 16e; Rosen's Emergency Medicine; Goldman-Cecil Medicine
Phase 4 — Refractory SE (>30 minutes, failed 1st + 2nd line)
RSE occurs in 20–30% of patients. Requires ICU admission, intubation, and continuous EEG monitoring.
Initiate anesthetic infusions — intubate first (use short-acting paralytic, e.g. succinylcholine, to allow seizure monitoring):
| Agent | Loading Dose | Maintenance Infusion |
|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05–2 mg/kg/h |
| Propofol | 1 mg/kg IV | 1–10 mg/kg/h |
| Pentobarbital | 20 mg/kg at 50–75 mg/min | 0.5–3 mg/kg/h |
| Thiopental | 3–5 mg/kg | Infusion |
| Ketamine | 1.5–4.5 mg/kg bolus | 2.2–5 mg/kg/h |
Titrate to burst suppression on continuous EEG. Avoid long-term paralytics — they mask ongoing electrical seizures.
Phase 5 — Super-Refractory SE (>24 h despite 3rd-line)
- Ketamine infusion (NMDA antagonist — mechanistically advantageous at this stage when NMDA receptors are upregulated)
- Inhaled anesthetics (isoflurane)
- Non-pharmacologic options: Vagal nerve stimulation (VNS), electroconvulsive therapy (ECT) — limited evidence
- Investigate for rare/autoimmune etiologies (anti-NMDA, anti-LGI1 encephalitis — up to 50% cryptogenic even after full workup) — Goldman-Cecil Medicine, 2024
Flowchart
Non-Convulsive SE
- Suspect when: prolonged postictal period, subtle motor signs (twitching, eye deviation, blinking), unexplained stupor/fluctuating confusion
- Diagnose with EEG
- Treatment follows same ladder but with less urgency — lower initial doses, more cautious titration
- Still requires treatment promptly; untreated NCSE causes neuronal injury
Systemic Complications to Monitor
| Complication | Action |
|---|---|
| Hyperthermia | Antipyretics + cooling blankets |
| Rhabdomyolysis | Monitor CK, creatinine; IV fluids |
| Metabolic acidosis | Correct underlying cause |
| Aspiration / respiratory failure | Early airway management |
| Hypoglycemia | IV dextrose |
| Cardiac arrhythmias (esp. with phenytoin) | Continuous cardiac monitoring |
| Raised ICP | Head of bed 30°, avoid hypotension |
Common Precipitants
- Subtherapeutic antiepileptic drug levels (most common in known epileptics)
- Acute stroke / hypoxia / anoxia
- CNS infection (meningitis, encephalitis — including autoimmune)
- Metabolic: hypo/hypernatremia, hypocalcemia, hypoglycemia
- Alcohol/drug withdrawal or intoxication
- Traumatic brain injury
- Fever in children (febrile SE)
Recent Evidence (2024–2025)
- Clinical Practice Guidelines on SE Management in Adults — Vignatelli et al., Epilepsia 2024 (PMID 38606469): Systematic review of adult CPGs confirming the BZD → second-line → anesthetic escalation framework.
- Ketamine in Pediatric SE — Chiriboga et al., Epilepsia 2024 (PMID 38881333): Meta-analysis supporting ketamine as an effective option in pediatric RSE.
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology 16e; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.