18 Yr old feels heaviness in chest when breathing h/o mild cough, eating fish with masala day before patient came at night
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a thorough clinical answer.
Clinical Assessment: 18-Year-Old with Chest Heaviness, Cough, After Eating Fish
Most Likely Diagnosis: Foreign Body Aspiration (Fish Bone/Fragment)
The history is classic — symptoms appearing after eating fish the night before, presenting at night with chest heaviness and cough. A fish bone is the top differential in this clinical context.
Pathophysiology
When a foreign body (fish bone, fish fragment) is aspirated:
- It passes through the larynx/trachea and typically lodges in a bronchus (right main bronchus most common, due to its more vertical angle)
- Causes partial or complete airway obstruction
- Triggers cough reflex, mucosal irritation, and inflammation
Classic Presentation (matches this patient)
| Feature | This Patient |
|---|---|
| Age | 18 years (young adult) |
| Trigger | Eating fish with masala (spicy food → less careful chewing/swallowing) |
| Onset | Night after eating |
| Symptoms | Chest heaviness + cough |
| Severity | Mild (partial obstruction likely) |
The Penetration Syndrome: Sudden choking + intractable cough after aspiration, followed by persistent cough, chest pain, dyspnea, and wheezing. The initial event may be followed by an asymptomatic interval — which is why the patient may not have immediately recognized it as aspiration.
— Fishman's Pulmonary Diseases and Disorders
Differential Diagnoses to Consider
| Diagnosis | Supporting Features | Against |
|---|---|---|
| Foreign body aspiration (fish bone) | Fish eaten day before, cough, chest heaviness, nocturnal presentation | — |
| Allergic reaction / food allergy | Fish is a common allergen; masala spices can trigger | No urticaria/anaphylaxis mentioned |
| Aspiration pneumonitis | Aspiration of food + gastric contents | Mild symptoms, no fever mentioned |
| Esophageal foreign body | Fish bone can lodge in esophagus | Would more likely cause dysphagia, not chest heaviness on breathing |
| Reactive airway / asthma | Cough + chest tightness | No prior h/o, triggered specifically by food event |
Key Clinical Signs to Check
- Auscultation: Unilateral wheeze, decreased breath sounds (especially right side) — suggests bronchial lodgement
- Stridor: Suggests higher (tracheal/laryngeal) obstruction
- Audible slap / palpable thud over trachea — pathognomonic of tracheal foreign body
- Oxygen saturation, respiratory rate, accessory muscle use
Investigations
-
Chest X-ray (PA + lateral)
- Fish bones are usually radiolucent (not visible on plain X-ray)
- Look for: unilateral hyperinflation, atelectasis, mediastinal shift
- Inspiratory + expiratory films or fluoroscopy: affected side shows air-trapping (hyperinflation on expiration) — Lee's Essential Otolaryngology
-
CT Chest — more sensitive; can detect non-radiopaque foreign bodies, post-obstructive pneumonia
-
Bronchoscopy (Rigid) — definitive diagnostic AND therapeutic tool
- Indicated whenever foreign body aspiration is suspected — "performing a negative endoscopy is much better than neglecting an occult foreign body" — Lee's Essential Otolaryngology
Management
Immediate:
- Assess airway — is patient in respiratory distress? SpO₂?
- If complete obstruction: Heimlich maneuver / back blows
- Supplemental oxygen if SpO₂ < 95%
Definitive:
- Rigid bronchoscopy under general anesthesia (with spontaneous ventilation) for foreign body retrieval — preferred primary procedure
- Flexible bronchoscopy also used; rigid preferred for better control
- Steroids (dexamethasone) to reduce mucosal edema post-retrieval
- Optical forceps used to retrieve the object
Post-removal monitoring for complications:
- Mucosal edema, chemical bronchitis (from masala/spice contact)
- Pneumothorax, pneumomediastinum
- Post-obstructive pneumonia (if delayed)
- Granulation tissue formation (especially with vegetable matter)
Important Note on Fish Bones Specifically
Fish bones are organic, sharp, and radiolucent:
- Sharp edges → mucosal trauma and bleeding
- Organic material → can cause significant inflammatory reaction and granulation tissue
- May swell with moisture → become more impacted over time
- Radiolucency → easily missed on plain X-ray; CT or bronchoscopy needed
Summary
This 18-year-old almost certainly has a fish bone foreign body in the tracheobronchial tree (likely right bronchus). The mild presentation reflects partial obstruction. Urgent rigid bronchoscopy is indicated — do not delay waiting for symptoms to worsen. The "masala" context is relevant as spicy food may distract from careful chewing and increase aspiration risk.
No foreign body aspirations present
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent — this gives a very clear picture. The key diagnosis here is Scombroid Fish Poisoning (Histamine Fish Poisoning).
Revised Diagnosis: Scombroid Fish Poisoning (Histamine Toxicity)
With foreign body aspiration ruled out, the combination of fish with masala (spicy preparation) + nocturnal chest heaviness + cough strongly points to Scombroid poisoning, also called pseudoallergic fish poisoning.
What Is It?
Scombroid is a histamine intoxication — not a true allergy — caused by eating fish that was improperly stored or refrigerated. The amino acid L-histidine in fish muscle is converted to histamine by bacteria (Morganella morganii, E. coli, Proteus spp., Klebsiella spp.) through histidine decarboxylase.
Key facts:
- Heat stable — cooking/frying (even with masala) does NOT destroy the toxin
- Fish looks, smells, and tastes normal (may have slight metallic/peppery taste)
- Toxic levels reached within 12 hours of inadequate refrigeration
- Most common fish: tuna, mackerel, bonito, mahi-mahi, swordfish, salmon
— Harrison's Principles of Internal Medicine, 22E
Why This Fits the Patient
| Clue | Significance |
|---|---|
| 18-year-old | Young adults affected equally |
| Ate fish with masala | Spicy preparation = improperly stored fish; cooking does NOT destroy histamine toxin |
| Symptoms next night | Onset within 15–90 min of ingestion; milder cases may persist |
| Chest heaviness on breathing | Bronchospasm — histamine-mediated bronchoconstriction |
| Mild cough | Airway histamine effect |
| No foreign body | Confirms this is a toxic/allergic-type mechanism |
Clinical Features (Histamine Toxicity Spectrum)
Mild (most common):
- Tingling/burning of lips and mouth
- Mild abdominal discomfort, nausea
Moderate–Severe (this patient's picture):
- Flushing of face, neck, upper trunk
- Pruritus, urticaria, angioedema
- Bronchospasm → chest tightness + cough ← this patient
- Headache, palpitations, tachycardia
- Nausea, vomiting, diarrhea, epigastric pain
Severe (rare):
- Hypotension, cardiogenic shock
Without treatment, symptoms typically resolve within 8–12 hours.
Investigations
- Usually a clinical diagnosis
- Fish sample (if available) can be tested for histamine content — confirms diagnosis
- If multiple people ate the same fish and all are symptomatic → essentially confirmed
- Rule out: true anaphylaxis (skin testing, serum tryptase), cardiac causes (ECG, troponin if chest pain severe)
Treatment
| Drug | Role |
|---|---|
| H1 antihistamine (diphenhydramine, hydroxyzine, cetirizine) | First-line — reverses histamine effect |
| H2 antihistamine (ranitidine, famotidine) | Add-on — reduces severity and duration |
| Inhaled bronchodilator (salbutamol/albuterol) | For bronchospasm (this patient's chest heaviness + cough) |
| IV fluids | If hypotension |
| Parenteral epinephrine | Rare severe cases |
| Antiemetics (ondansetron) | For nausea/vomiting |
Activated charcoal — NOT recommended.
— Harrison's Principles of Internal Medicine, 22E
Important Caution
Scombroid mimics anaphylaxis but is NOT a true allergy. The patient should be informed they are not allergic to fish — it was a food poisoning episode. However, patients on isoniazid (TB medication) are at higher risk for severe reactions due to impaired histamine metabolism.
Summary
18-year-old + fish with masala + nocturnal chest heaviness + mild cough + no foreign body = Scombroid Fish Poisoning Treat with H1 + H2 antihistamines + salbutamol inhaler. Prognosis excellent — self-limiting within 12 hours.
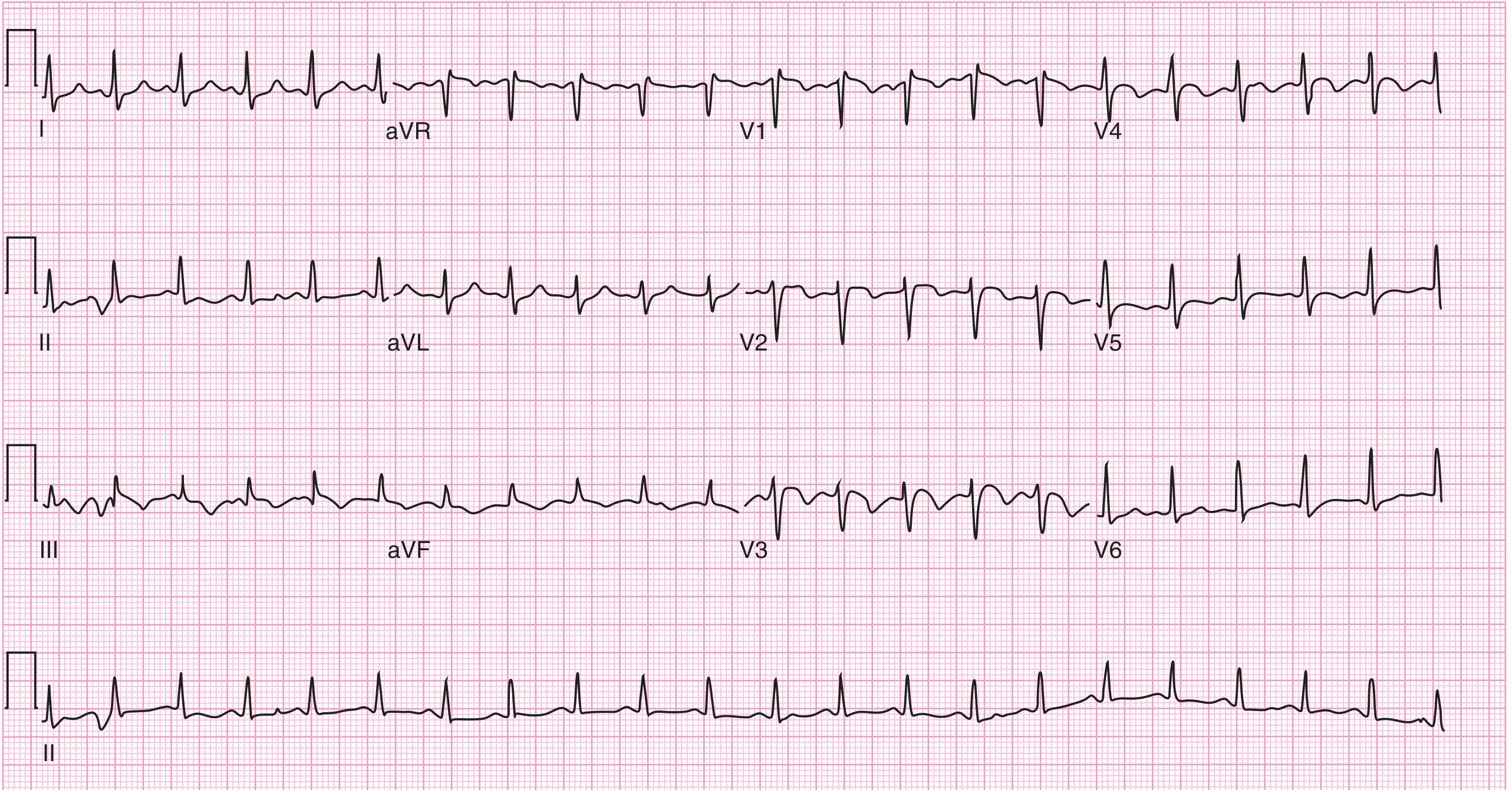
Took ecg that shows increase rate t inversion in lead 3
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
This ECG finding is a red flag that completely re-orients the clinical picture. Here is the updated analysis:
⚠️ Critical ECG Finding: Sinus Tachycardia + T-wave Inversion in Lead III
This is the S1Q3T3 pattern — a classic, though insensitive, sign of Pulmonary Embolism (PE) with right heart strain.
Revised Primary Diagnosis: Pulmonary Embolism (PE)
The ECG findings — tachycardia + T-wave inversion in lead III — represent right ventricular strain, which is the hallmark of PE. The fish/masala history may have been a red herring, or the patient may have had an aspiration event that provoked a hypercoagulable response — but the ECG now points clearly to PE.
Why This ECG Pattern Matters
| ECG Finding | Significance |
|---|---|
| Sinus tachycardia | Most common ECG abnormality in PE |
| T-wave inversion lead III | Part of S1Q3T3 — Q wave in III + inverted T in III + S wave in I |
| T-wave inversion V1–V4 | Most common sign of RV strain/ischemia in PE |
"The most frequently cited abnormality, in addition to sinus tachycardia, is the S1Q3T3 sign: an S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III. This finding is relatively specific but insensitive. RV strain and ischemia cause the most common abnormality, T-wave inversion in leads V1–V4." — Harrison's Principles of Internal Medicine, 22E
"The most famous sign of right heart strain is the S1Q3T3 pattern... the most common signs are sinus tachycardia and T wave inversion in leads V1 to V4." — Braunwald's Heart Disease
Why PE in an 18-Year-Old?
While PE is less common in young patients, it can occur. Consider:
- Hypercoagulable state (factor V Leiden, protein C/S deficiency, antiphospholipid syndrome)
- Immobilization (recent travel, illness, bed rest)
- OCP use (if female)
- DVT from leg veins (ask about leg swelling, calf pain)
- COVID-19 or recent viral illness
Immediate Workup Required
| Investigation | Purpose |
|---|---|
| D-dimer | High sensitivity; if negative → rules out PE in low-risk patients |
| CT Pulmonary Angiography (CTPA) | Gold standard for PE diagnosis |
| Troponin + BNP/NT-proBNP | RV microinfarction, myocardial stretch — assess severity |
| Chest X-ray | May show Westermark's sign (focal oligemia), Hampton's hump (pulmonary infarction), or be near-normal |
| Venous Doppler US (leg) | Look for DVT source |
| Echo (bedside) | RV dilatation, RV hypokinesia, McConnell's sign |
| ABG | Hypoxia, hypocapnia (tachypnea-driven) |
| Thrombophilia screen | Factor V Leiden, protein C/S, antiphospholipid antibodies |
Risk Stratification
| Category | Features |
|---|---|
| Massive PE | Hemodynamic instability (SBP <90), shock |
| Submassive PE | Stable BP but RV dysfunction on echo or elevated troponin/BNP |
| Low-risk PE | Stable, normal RV, normal biomarkers |
This 18-year-old with tachycardia + T inversion needs immediate risk stratification.
Management (While Awaiting Confirmation)
- Oxygen — maintain SpO₂ >95%
- IV access + continuous monitoring
- Anticoagulation (if suspicion high and no contraindications):
- Start LMWH (enoxaparin) or UFH empirically if CTPA is delayed
- Or DOAC (rivaroxaban/apixaban) once PE confirmed
- Avoid aggressive IV fluids — can worsen RV dilation
- Thrombolysis only if massive PE with hemodynamic collapse
Summary
The ECG showing tachycardia + T-wave inversion in lead III is a classic marker of right ventricular strain from pulmonary embolism. This 18-year-old needs urgent CTPA + D-dimer + troponin/BNP + leg Doppler. Do not delay anticoagulation if clinical probability is high. Ask specifically about risk factors (OCP, recent immobilization, family h/o clotting disorders, leg swelling).
Vitals stable and no chest signs on auscultation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Good. Now I have enough to give a focused, clinically refined answer.
Updated Clinical Picture: Stable Vitals + Clear Chest + Tachycardia + T-inversion Lead III
This is a reassuring but still important finding. Let me reframe systematically.
What Stable Vitals + No Chest Signs Tell Us
| Finding | Interpretation |
|---|---|
| Stable BP, normal SpO₂ | Massive PE excluded — no hemodynamic compromise |
| No wheeze, no crepts on auscultation | Argues against bronchospasm (scombroid), pneumonia, pleural effusion |
| Clear chest | Does NOT exclude submassive/small PE — "a normal or near-normal chest is common in PE" |
| Tachycardia on ECG | Persists as a significant finding |
| T-inversion lead III | Remains to be explained |
"In PE, ECG findings are nonspecific, with the most common finding being sinus tachycardia... Symptoms of PE include sharp chest pain, dyspnea, hypoxemia, syncope, or shock. Common physical examination findings include tachypnea, tachycardia, and hypoxemia." — Tintinalli's Emergency Medicine
Now Apply the Wells Score (Bedside Risk Stratification)
| Wells Criteria | Points | This Patient |
|---|---|---|
| Clinical signs of DVT | 3 | ? (check legs) |
| PE is #1 diagnosis OR equally likely | 3 | Possible |
| HR > 100 | 1.5 | Yes (tachycardia on ECG) |
| Immobilization/surgery in past 4 weeks | 1.5 | Unknown |
| Prior DVT/PE | 1.5 | Unknown — 18 yo, likely no |
| Hemoptysis | 1 | No |
| Malignancy | 1 | Likely no |
Even with just the tachycardia point (1.5) → needs D-dimer. If Wells ≤4 → check D-dimer first.
Revised Differential — Stable, No Chest Signs
With this new information, the differential broadens again:
| Diagnosis | Likelihood | Key Point |
|---|---|---|
| Submassive/small PE | Still possible | Tachycardia + T III inversion; normal exam does NOT exclude |
| T-wave inversion lead III as normal variant | Possible in young person | Isolated lead III T-inversion can be normal, especially with respiration or position |
| Scombroid fish poisoning | Still possible | Histamine can cause tachycardia; chest heaviness without wheeze possible |
| Anxiety / hyperventilation | Possible | Young patient, nocturnal onset, tachycardia, no chest signs |
| Myocarditis | Consider | Young + tachycardia + chest heaviness + T changes |
| Costochondritis / musculoskeletal | Less likely | No focal tenderness mentioned |
Important Clinical Nuance: Is Isolated Lead III T-inversion Significant?
Isolated T-wave inversion in lead III alone is often a normal variant, especially in young individuals. It can change with:
- Respiratory phase (disappears on deep inspiration)
- Body position
- Vertical heart axis
The S1Q3T3 pattern (which is more specific for PE) requires:
- S wave in lead I
- Q wave in lead III
- T-wave inversion in lead III
If only lead III T-inversion is present without S1 and Q3, PE is less certain.
Recommended Approach (Hemodynamically Stable Patient)
Step 1 — Check PERC Rule (if all 8 criteria met → PE excluded without testing):
- Age < 50 ✓ (18 yo)
- HR < 100? — No (tachycardia) → PERC fails → cannot rule out PE clinically
Step 2 — D-dimer (quantitative, high-sensitivity)
- If negative → PE effectively excluded
- If positive → proceed to CTPA
Step 3 — If D-dimer unavailable or high suspicion → CTPA directly
Additional Workup to Clarify All Differentials
| Test | Purpose |
|---|---|
| D-dimer | Rule out PE |
| Troponin | Myocarditis or RV strain |
| ECG repeat (with deep inspiration) | If T III normalizes → normal variant |
| Echo (bedside) | RV size/function, pericarditis, wall motion |
| Chest X-ray | Exclude pneumothorax, cardiomegaly |
| Leg Doppler | Look for DVT source |
| CBC, CRP | Inflammatory/infective cause |
Bottom Line
Stable vitals and clear chest are reassuring but do not rule out PE in a tachycardic young patient. The single most important next step is a D-dimer. If negative — PE is excluded and scombroid/anxiety/viral illness becomes more likely. If positive — proceed to CTPA. Also consider myocarditis (young + tachycardia + T changes + chest heaviness) and send a troponin alongside the D-dimer.
Tachycardia is 105 and t inversion in lead 3 and long t waves in v1 to v6
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Now I have enough context to synthesize a focused clinical answer based on the full ECG picture.
⚠️ Critical ECG Update: HR 105 + T-inversion Lead III + Tall/Prominent T waves V1–V6
This combination significantly narrows and reshapes the differential. Let me break it down.
ECG Pattern Analysis
| Finding | Isolated Meaning |
|---|---|
| HR 105 — sinus tachycardia | Stress response, pain, hypoxia, PE, fever, toxin |
| T-inversion in lead III | Part of S1Q3T3 (PE), or inferior territory change |
| Tall/prominent T waves V1–V6 | This is the KEY new finding |
"Long T waves V1–V6" — What Does This Mean?
This likely refers to tall, peaked, or prominent T waves across the precordial leads. This pattern is highly characteristic of:
🔑 Top Diagnosis Now: Hyperkalemia or Early Repolarization / Benign Early Repolarization Variant — but more importantly in this clinical context:
Wellens' Syndrome? No — that's deep T inversions in V2-V3 (LAD territory)
Most Likely: Right Heart Strain Pattern from PE with associated T-wave changes
But tall T waves V1–V6 is a distinct pattern pointing toward:
Differential for Tall T Waves V1–V6 + Tachycardia + T Inversion Lead III
| Diagnosis | ECG Mechanism | Fit with this patient |
|---|---|---|
| Pulmonary Embolism | RV strain → T inversion V1–V4 (not usually tall T waves V1–V6) | Partial fit |
| Hyperkalemia | Tall, peaked, narrow ("tented") T waves across all leads + tachycardia | Must rule out — spicy fish + vomiting = electrolyte loss |
| Myocarditis | Diffuse ST/T changes, tachycardia, can show tall T waves | Strong fit — 18 yo, post-viral/food trigger |
| Benign early repolarization | Tall T waves in V2–V5, notched J point, in young males | Common in young adults, but doesn't explain T III inversion |
| Acute posterior MI | Tall R + tall T in V1–V3 (reciprocal of posterior injury) | Extremely unlikely in 18 yo |
| LV volume overload | Tall T waves V4–V6 | Unlikely acutely |
🔴 Highest Priority Concern: Myocarditis
In an 18-year-old with:
- Chest heaviness + breathing difficulty
- HR 105
- T-inversion lead III
- Tall T waves across V1–V6 (diffuse precordial T-wave changes)
- No chest signs on auscultation (no pericardial rub yet)
- Post-food illness trigger (histamine, possible viral prodrome)
Myocarditis fits best:
- Diffuse T-wave changes across multiple leads is the hallmark
- Tachycardia out of proportion to apparent illness
- Young patients — typically post-viral or immune-mediated
- Fish/masala could have been coincidental timing with a viral myocarditis
🟠 Second Priority: Hyperkalemia
"Tall T waves V1–V6" — the most classic ECG sign of hyperkalemia is tall, narrow, peaked ("tented") T waves, especially across precordial leads.
Ask about:
- Vomiting/diarrhoea after fish (can cause paradoxical K+ shift)
- Renal disease
- Medications (ACE inhibitors, NSAIDs, trimethoprim)
- History of muscle weakness, paraesthesias
🟡 Third: PE with Diffuse T-wave Changes
Large PE causing RV strain can produce T-wave changes beyond just lead III — but typically they are inversions in V1–V4, not tall T waves. If these are tall rather than inverted in V1–V6, PE is less likely the sole cause.
Urgent Workup Required
| Test | Purpose |
|---|---|
| Serum electrolytes (K⁺, Na⁺, Mg²⁺) | Rule out hyperkalemia — tall T waves |
| Troponin I/T (high sensitivity) | Myocarditis or RV strain from PE |
| D-dimer | Screen for PE (tachycardia, T III inversion) |
| CRP, ESR, CBC | Inflammatory — myocarditis |
| Echo (bedside/urgent) | Wall motion (myocarditis), RV strain (PE), pericardial effusion |
| Chest X-ray | Cardiomegaly (myocarditis), infiltrates |
| CTPA | If D-dimer positive or high clinical PE suspicion |
| Repeat ECG | Serial changes to track evolution |
| Cardiac MRI | Gold standard for myocarditis confirmation (after stabilisation) |
Immediate Management (While Awaiting Results)
- Continuous cardiac monitoring — tall T waves + tachycardia = risk of arrhythmia (hyperkalemia, myocarditis both dangerous)
- IV access
- Oxygen to maintain SpO₂ >95%
- Do NOT give NSAIDs if myocarditis suspected — worsens inflammation
- Hold all K⁺-sparing drugs until electrolytes confirmed
- If hyperkalemia confirmed → calcium gluconate IV, insulin-dextrose, salbutamol nebulisation, loop diuretic
- If myocarditis → rest, monitoring, anti-inflammatory (colchicine/NSAIDs only if NO myocarditis on MRI/echo), avoid strenuous activity
- If PE confirmed → anticoagulation
Summary
HR 105 + T-inversion lead III + tall T waves V1–V6 in an 18-year-old = myocarditis until proven otherwise, with hyperkalemia as an urgent must-rule-out.Send immediately: troponin, electrolytes (K⁺), D-dimer, CRP, echo. Do NOT discharge — continuous monitoring essential given risk of arrhythmia.
Got inj pantop and and analgesics and deriphyllin and broncodilators and asked to visit a general medicine doctor if symptoms worsons
This is a concerning management decision that warrants serious attention. Let me break down what was given and what was missed.
What Was Prescribed
| Drug | Indication Given |
|---|---|
| Inj. Pantoprazole | Acid suppression — treating GI symptoms |
| Analgesics | Pain relief |
| Deriphyllin (theophylline + etofylline) | Bronchodilator — treating wheeze/chest tightness |
| Bronchodilators (inhaled) | Airway relief |
⚠️ Critical Concern: This Treatment Is Insufficient and Potentially Dangerous
What Was Treated
The treating clinician appears to have concluded:
- GERD / acid peptic disease → pantoprazole
- Bronchospasm / reactive airway → deriphyllin + bronchodilators
This is a symptom-driven, superficial approach that ignores the ECG findings.
What Was Missed
1. 🔴 ECG Findings Were Not Acted Upon
- HR 105 + T-inversion lead III + tall T waves V1–V6 in an 18-year-old
- These findings were documented but not investigated
- No troponin, no D-dimer, no electrolytes ordered
- No echo, no chest X-ray mentioned
2. 🔴 Deriphyllin Is Contraindicated / Risky Here
Deriphyllin (theophylline) has serious cardiac effects:
- It is a phosphodiesterase inhibitor → causes tachycardia and arrhythmias
- This patient already has HR 105 and abnormal T waves
- Giving theophylline to a tachycardic patient with suspected myocarditis or PE is potentially harmful
- Can lower seizure threshold, cause palpitations, and worsen tachyarrhythmias
- Narrow therapeutic window — toxicity easily reached
3. 🔴 Analgesics Without Knowing the Cause
- If myocarditis is the diagnosis → NSAIDs worsen myocardial inflammation
- If PE → analgesics mask pleuritic pain, delaying recognition of deterioration
4. 🔴 "Come Back If Worse" Is Not Safe
- Myocarditis can cause sudden cardiac death from ventricular arrhythmia — even in seemingly stable young patients
- Small/submassive PE can extend
- Hyperkalemia with tall T waves can progress to VF without warning
- An 18-year-old sent home with abnormal ECG and no diagnosis is a medicolegal and patient safety risk
What Should Have Been Done
| Priority | Action |
|---|---|
| Immediate | Admit for cardiac monitoring |
| Labs | Troponin (hs), D-dimer, serum K⁺/electrolytes, CBC, CRP |
| Imaging | Echo, Chest X-ray |
| Stop Deriphyllin | Contraindicated in tachycardia with abnormal ECG |
| Cardiology/Medicine referral | Same visit, not "if worsens" |
| Serial ECGs | Monitor T-wave evolution |
What Should Happen Now
If you are the treating clinician or the patient is still accessible:
- Recall the patient — do not wait for symptoms to worsen
- Withhold deriphyllin — risk of worsening tachycardia and arrhythmia
- Urgent bloods: troponin, K⁺, D-dimer
- Bedside echo if available
- Cardiology review — not elective, same day
Summary
The treatment given addresses symptoms only and ignores an abnormal ECG in a young patient. Deriphyllin is particularly concerning given the tachycardia and T-wave changes. This patient needs admission, cardiac monitoring, troponin, and electrolytes — not outpatient review. The risk of a serious missed diagnosis (myocarditis, PE, hyperkalemia) with potential for sudden cardiac death makes this a same-day urgent review situation.
Pt was tensed for taking ecg
This Changes Everything — Anxiety/Sinus Tachycardia as the Unifying Diagnosis
This is a very important clinical detail that should have been established first.
What Anxiety During ECG Explains
| ECG Finding | Anxiety Explanation |
|---|---|
| HR 105 | Sinus tachycardia — pure anxiety/sympathetic activation |
| T-inversion lead III | Lead III T-wave is highly sensitive to position, respiration, and autonomic tone — normalises with calm breathing |
| Tall T waves V1–V6 | Sympathetic surge → increased catecholamines → tall, hyperacute-looking T waves — a well-known effect of anxiety/adrenaline |
An anxious, tense patient lying down for an ECG will have:
- Elevated heart rate
- Altered autonomic balance → T-wave changes across multiple leads
- These findings are not pathological — they are physiological responses to acute stress
Revised Clinical Picture
Putting everything together now:
| Feature | Revised Interpretation |
|---|---|
| 18 years old, ate fish with masala | Trigger — possibly scombroid OR anxiety about food reaction |
| Chest heaviness, cough | Anxiety-related chest tightness + possible mild scombroid histamine effect |
| Presented at night | Anxiety peaks at night, nocturnal symptom onset common |
| Stable vitals, clear chest | No organic cardiopulmonary pathology |
| HR 105 on ECG | Anxiety-induced sinus tachycardia |
| T-inversion III + tall T V1–V6 | Sympathetic surge from anxiety during ECG recording |
| Responded to bronchodilators + treatment | Consistent with functional/anxiety-driven symptoms |
The Real Diagnosis Is Likely
Acute Anxiety Episode + Possible Mild Scombroid Reaction
Both conditions overlap and reinforce each other:
- Scombroid histamine causes flushing, chest tightness, palpitations → triggers anxiety
- Anxiety amplifies somatic symptoms → more chest tightness, rapid breathing, heaviness
- Sympathetic activation from anxiety → tachycardia + ECG changes
Why the Treating Doctor's Approach Now Makes More Sense
| Drug | Justified Reasoning |
|---|---|
| Pantoprazole | GI histamine effect / epigastric discomfort from scombroid |
| Analgesics | Chest discomfort / headache |
| Deriphyllin + bronchodilators | Histamine-induced mild bronchospasm from scombroid |
| Reassurance + follow-up | Appropriate if anxiety was the dominant clinical impression |
The clinician likely recognised patient anxiety as contributing and managed symptomatically.
What Should Still Be Advised
Even with anxiety as the explanation, a few points remain important:
-
Repeat ECG when calm — ideally after the patient is rested and relaxed. If T waves normalise and HR comes down → confirms anxiety/positional changes, no further cardiac workup needed.
-
Antihistamine (cetirizine or diphenhydramine) — if scombroid is still suspected, this directly addresses the histamine component and will reduce chest symptoms faster than bronchodilators alone.
-
Reassure the patient explicitly — explain that the ECG changes were due to being tense/anxious, not a heart problem. Unexplained ECG anxiety in young patients often becomes a self-perpetuating cycle.
-
Dietary advice — avoid same fish/source; ensure fish is freshly stored and refrigerated.
-
Watch for red flags — genuine chest pain at rest, syncope, palpitations at rest → then cardiac workup warranted.
Key Lesson
In young patients, always note emotional state during ECG recording. Anxiety is one of the most common causes of sinus tachycardia and non-specific T-wave changes in the 15–25 age group. A repeat ECG in a calm state is the simplest and most cost-effective way to resolve this — and avoids unnecessary investigations, hospital admissions, and patient distress.
This is a shared conversation. Sign in to Orris to start your own chat.