Acute eosinophil pneumonia Full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute eosinophilic pneumonia"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from four major textbooks. Let me compile the full MD exam answer.
Acute Eosinophilic Pneumonia (AEP) — 15-Mark Exam Answer
Definition
Acute eosinophilic pneumonia (AEP) is a syndrome characterized by acute febrile respiratory illness, hypoxemic respiratory failure, diffuse bilateral pulmonary infiltrates, and pulmonary eosinophilia (>25% eosinophils on BAL), occurring in a previously healthy individual, with duration of illness <1 month, and dramatic response to corticosteroids without recurrence.
— Harrison's Principles of Internal Medicine 22E, p. 2275
Epidemiology
- Typically affects males aged 20–40 years
- No prior history of asthma required (unlike chronic eosinophilic pneumonia)
- No definite seasonal variation
- Up to 70% of patients have a smoking history
- Can occur at any age and in either sex, but male predominance is well established
Etiology & Pathogenesis
AEP is triggered by inhaled environmental agents in a susceptible host; in most cases, a specific antigen is never identified (hence "idiopathic").
Common triggers include:
| Category | Examples |
|---|---|
| Tobacco | New-onset cigarette smoking, recent change in smoking habits, e-cigarettes (vaping), flavored tobacco |
| Drugs | Minocycline, daptomycin, venlafaxine, NSAIDs, antidepressants, antimicrobials |
| Illicit substances | Cocaine, heroin inhalation |
| Environmental dust | Indoor renovations, World Trade Center dust, military deployment (Iraq), cave exploration, woodpile moving |
| Infections | Parasitic, fungal (rarely), H1N1 influenza |
| Systemic conditions | Chronic myelogenous leukemia, hematopoietic stem cell transplantation, HIV |
Pathogenetic mechanism:
- Inhaled agent → epithelial injury → release of DAMPs (IL-33, uric acid, ATP)
- IL-33 activates ILC2 cells → rapid innate immune activation
- CD4+ Th2 lymphocyte adaptive response (requires days to weeks)
- Release of type 2 cytokines: IL-4, IL-5, IL-13
- IL-5 → bone marrow eosinophil production and maturation; IL-13 → eosinophil chemotactic factors
- Eosinophil chemokines (eotaxins CCL11, CCL24, CCL26; LTB4) → massive eosinophil migration into lung
- Eosinophil granule proteins → tissue damage and diffuse alveolar injury
An early hypothesis of IgE-mediated type I hypersensitivity with mast cell degranulation has not been confirmed.
— Fishman's Pulmonary Diseases and Disorders, p. 1221–1222
Clinical Features
Symptoms (onset <7 days; may extend to 30 days):
- Acute onset fever (high-grade), chills, malaise, myalgias
- Dyspnea and dry/nonproductive cough
- Pleuritic chest pain
- Night sweats
- Rapid progression from mild dyspnea → overt respiratory failure requiring mechanical ventilation
Signs:
- Tachypnea, tachycardia
- High fever
- Bilateral basilar crackles (inspiratory); wheezing may be present
- Signs of hypoxemic respiratory failure (PaO₂ < 60 mmHg on room air)
- No signs of multiorgan dysfunction (this distinguishes AEP from sepsis/ARDS)
Key distinguishing features from ARDS/acute lung injury:
- No preceding infection or systemic illness
- BAL eosinophilia >25%
- Dramatic response to corticosteroids
- No multisystem organ failure
Laboratory Findings
| Investigation | Finding |
|---|---|
| CBC | Moderate leukocytosis with left shift; blood eosinophilia absent at onset (appears 7–30 days later; mean ~1700/μL) |
| ESR / CRP | Elevated (nonspecific) |
| IgE | Moderately elevated |
| ABG | PaO₂ < 60 mmHg; hypoxemic respiratory failure |
| BAL | >25% eosinophils — the key diagnostic finding; also lymphocytes, neutrophils; high pH |
| Pleural fluid | Marked eosinophilia, high pH |
| TARC/CCL17 | Elevated — helps distinguish AEP from non-eosinophilic ALI |
| FeNO | Elevated (>23.5 ppb); decreases with steroid treatment |
| KL-6 | Low/normal (helps exclude other ILD) |
Critical point: Blood eosinophilia is typically ABSENT at presentation — its absence should not exclude AEP. BAL eosinophilia is the cornerstone of diagnosis.
Imaging
Chest X-ray:
- Early: subtle patchy infiltrates, Kerley B lines
- Later: bilateral alveolar and interstitial infiltrates (diffuse)
- Bilateral pleural effusions in 50–70% of patients
HRCT / CT Chest:
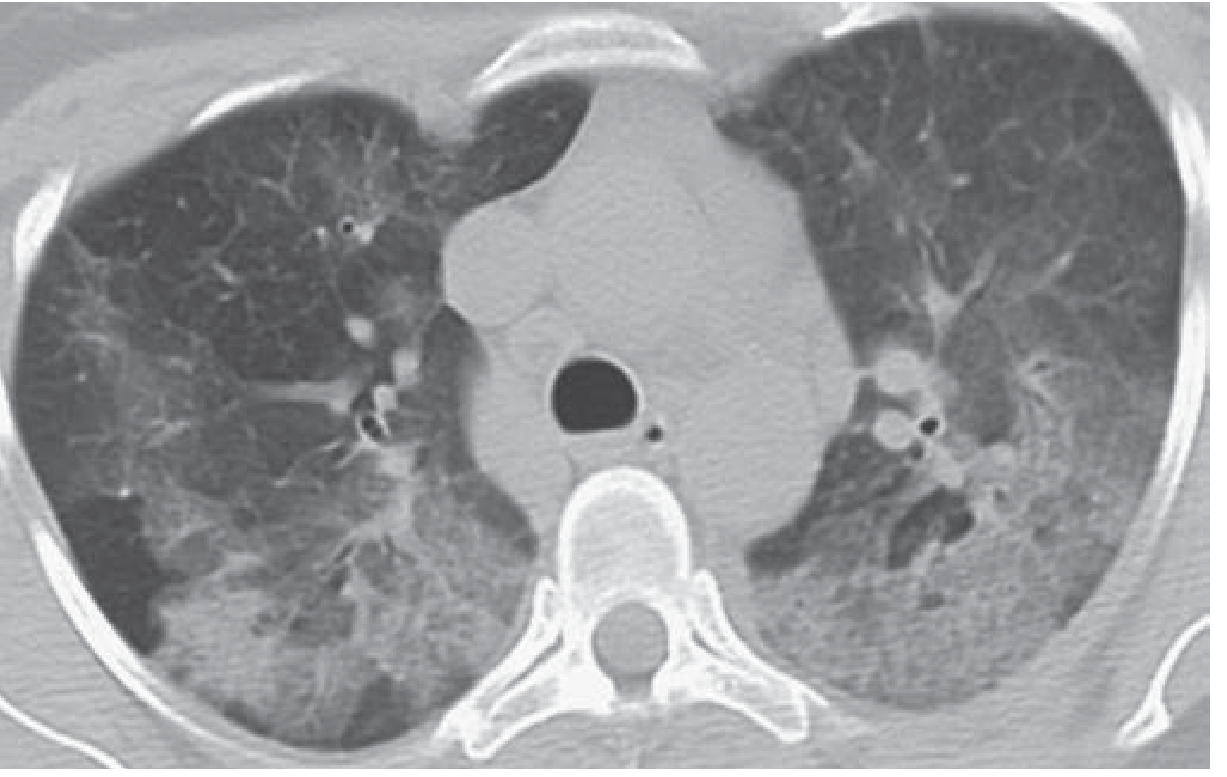
- Bilateral ground-glass opacification and consolidation in a random (non-segmental) distribution
- Interlobular septal thickening
- Thickening of bronchovascular bundles
- Small to moderate bilateral pleural effusions
- Mediastinal lymphadenopathy (common)
- CT appearance can mimic pulmonary edema or DAD
Pathology
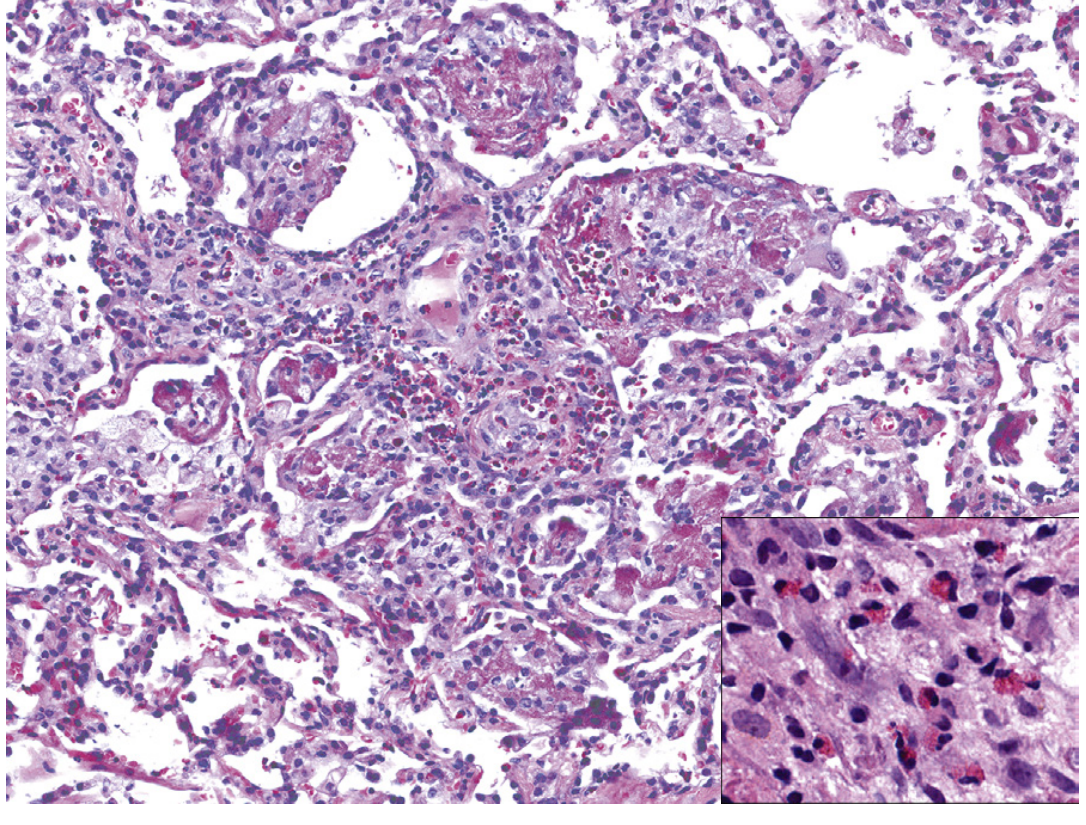
Light microscopy reveals:
- Prominent eosinophil infiltration in interstitium, alveolar spaces, and bronchial walls
- Diffuse alveolar damage (DAD) pattern with hyaline membranes — distinctive for AEP
- Type 2 pneumocyte hyperplasia
- Intra-alveolar fibrinous exudate
- Lymphocytic interstitial infiltration
- Granulomas, alveolar hemorrhage, and non-necrotic perivascular inflammation reported
- Basal lamina damage is unusual
Biopsy is generally NOT required if BAL eosinophilia >25% is present.
Diagnostic Criteria (Modified Philit Criteria)
All four criteria must be met:
| # | Criterion |
|---|---|
| 1 | Acute respiratory illness of ≤1 month duration |
| 2 | Diffuse bilateral pulmonary infiltrates on CXR or CT |
| 3 | Pulmonary eosinophilia: BAL >25% eosinophils OR eosinophilic pneumonia on biopsy |
| 4 | Exclusion of known causes: parasitic/fungal/viral infection, drugs, toxins, EGPA, HES, ABPA |
Additional features supporting diagnosis (Harrison's 22E):
- Hypoxemic respiratory failure
- Quick clinical response to corticosteroids
- Failure to relapse after discontinuation of corticosteroids
Differential Diagnosis
| Condition | Key differentiator |
|---|---|
| ARDS / ALI | No BAL eosinophilia; poor steroid response; often multiorgan failure |
| Community-acquired pneumonia | No eosinophilia; responds to antibiotics |
| Chronic eosinophilic pneumonia | Indolent course weeks-months; peripheral opacities; blood eosinophilia present; female, non-smoker |
| EGPA (Churg-Strauss) | Asthma, sinusitis, systemic vasculitis, ANCA positivity |
| Löffler syndrome | Fleeting transient infiltrates; parasitic etiology; mild illness |
| Hypereosinophilic syndrome | Persistent blood eosinophilia >1500; multiorgan involvement |
Treatment
Step 1: Identify and remove the causative exposure (stop smoking, discontinue culprit drug)
Step 2: Corticosteroids — the mainstay of treatment
- Mechanism: Induce apoptosis of eosinophils → rapid resolution
- Oral prednisone: 40–60 mg/day for mild-moderate disease
- IV methylprednisolone: 60–125 mg every 6–8 hours for severe/intubated patients
- Duration: typically 2–4 weeks, then taper over 1–2 months
- Response: Fever and respiratory symptoms abate within 12–48 hours; radiographic resolution within 1–2 weeks; complete resolution within several weeks
Step 3: Respiratory support
- ICU admission for severe hypoxemia
- Non-invasive ventilation (CPAP/BiPAP) for moderate respiratory failure
- Invasive mechanical ventilation for respiratory failure unresponsive to NPPV
- Supplemental oxygen
Key treatment principles:
- Do NOT delay steroids while waiting for investigation results if AEP is strongly suspected
- Antibiotics are NOT indicated (unless concurrent infection excluded)
- No role for antifungal or antiparasitic therapy unless infection confirmed
Prognosis
- Excellent prognosis — characteristic feature of AEP
- Complete clinical and radiographic recovery in almost all patients within several weeks
- No recurrence in truly idiopathic AEP after corticosteroid discontinuation
- No residual pulmonary sequelae (unlike ARDS)
- Relapse possible if smokers resume smoking — disease may recur upon re-exposure
AEP vs Chronic Eosinophilic Pneumonia — Key Comparison
| Feature | AEP | CEP |
|---|---|---|
| Onset | Acute (<1 month) | Subacute (weeks–months) |
| Sex | Male predominance | Female predominance |
| Smoking | Often smokers | Non-smokers |
| Asthma | Absent | Present in majority |
| Blood eosinophilia | Absent initially | Present |
| Respiratory failure | Common, severe | Uncommon |
| CXR pattern | Diffuse bilateral | Peripheral upper zone ("photographic negative of pulmonary edema") |
| Recurrence | Rare (unless re-exposed) | Common |
Summary Flowchart
Young male + acute fever + dyspnea + bilateral infiltrates + hypoxemia
↓
Suspect AEP (especially if recent smoking onset or new inhaled exposure)
↓
BAL → >25% eosinophils? Yes → Exclude infection/drugs → AEP CONFIRMED
↓
Remove exposure + IV methylprednisolone → rapid response within 24–48h
↓
Complete recovery, no recurrence
Sources: Harrison's Principles of Internal Medicine 22E (2025); Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Grainger & Allison's Diagnostic Radiology | Recent review: Carbone RG et al., Acute and chronic eosinophilic pneumonia: an overview — Front Med (Lausanne) 2024 [PMID: 38711783]
This is a shared conversation. Sign in to Orris to start your own chat.