
IMG-20260620-WA0014(1).jpg
53/F k/c/o- hypertension a/w/c/o- outside eating in 10mins vomiting f/b dixziness, palpitations, sweating f/b vomiting, epigastri pain, loose motion 4epi
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute myocardial infarction" AND "gastrointestinal symptoms" AND "inferior"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is my full analysis:
Clinical Assessment - 53/F, Known Hypertensive
Presentation Summary
Post-outside-meal onset within 10 minutes: vomiting → dizziness, palpitations, sweating → vomiting + epigastric pain + loose stools x4 episodes
This constellation - GI symptoms dominating a cardiac event - is the classic trap of Inferior STEMI presenting as a GI illness. Do not be reassured by the food history.
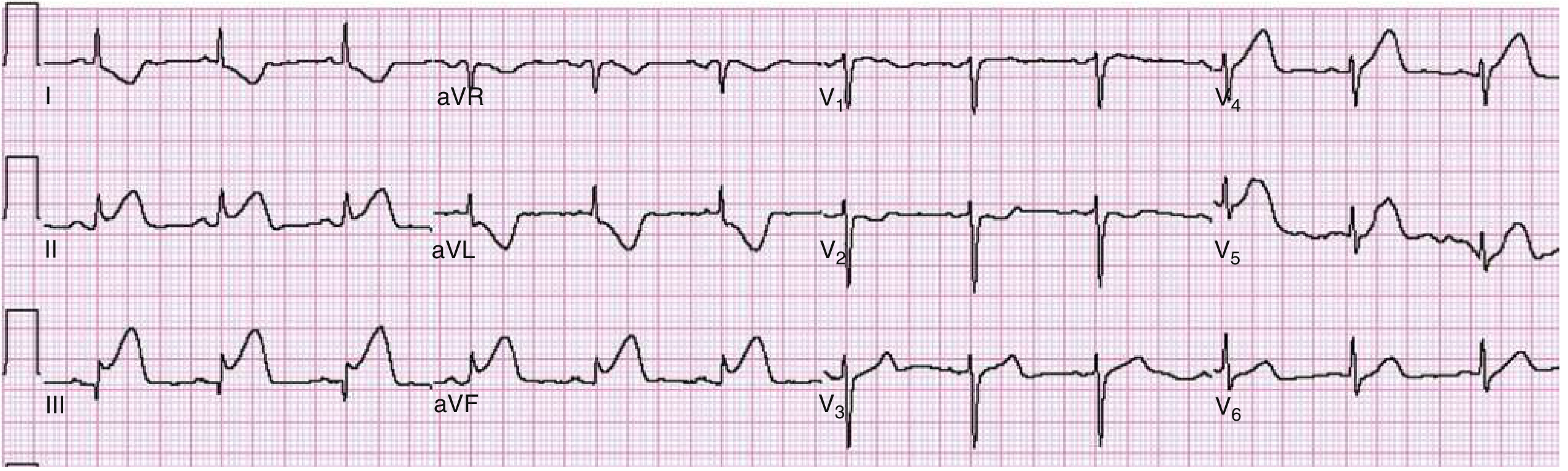
ECG Analysis (Schiller AT-102, 20-Jun-26, 16:24)
Machine read: Sinus Rhythm, HR 66/min, QTc 461 ms, Non-specific T abnormality
My read - this is NOT a normal ECG:
| Parameter | Value |
|---|---|
| Rate | 66 bpm |
| Rhythm | Sinus |
| PR | 156 ms (normal) |
| QRS | 70 ms (narrow) |
| QT/QTc | 430/461 ms (borderline prolonged) |
Critical ECG Findings:
1. INFERIOR LEADS (II, III, aVF):
- ST elevation is visible in leads II, III, and aVF - consistent with Inferior STEMI / Inferior wall injury
- The elevation appears more prominent in lead III > lead II - this pattern (ST III > ST II + ST depression in aVL/I) is >90% sensitive for Right Coronary Artery (RCA) occlusion
2. LEAD aVL:
- Reciprocal ST depression in aVL - classic mirror change of inferior STEMI; its presence confirms the inferior injury pattern and is associated with larger infarct size and higher mortality
3. PRECORDIAL LEADS (V1-V3):
- There appears to be ST depression in V1-V2 - this raises concern for either:
- Reciprocal change from inferior STEMI
- Posterior wall extension (inferobasal MI)
- Concomitant RV infarction (especially with ST elevation in V1 when III > II)
4. QTc 461 ms - mildly prolonged; monitor for arrhythmias
Machine label "Non-specific T abnormality" underestimates this ECG. The GI presentation masked what is clinically an Inferior STEMI with possible RV involvement until the ECG.
Reference ECG - Inferior AMI with Reciprocal Changes (Textbook, Rosen's Emergency Medicine):
Rosen's Emergency Medicine: Marked ST elevation in II, III, aVF with reciprocal ST depression in I and aVL - identical pattern to this patient.
Why the GI Presentation?
The inferior wall of the LV and the AV node are supplied by the RCA (~90% of patients). RCA territory ischemia stimulates the Bezold-Jarisch reflex - a vagal reflex triggered by inferior wall receptors - producing:
- Nausea and vomiting
- Bradycardia/dizziness
- Diaphoresis
- Hypotension
- Diarrhea (increased bowel motility via vagal activation)
This perfectly explains her presentation within 10 minutes of eating (the meal likely increased vagal tone, unmasking or worsening the ischemic event).
Immediate Management
Step 1 - Activate STEMI Protocol NOW
- Call for emergency PCI (target door-to-balloon < 90 min)
- If PCI not available within 120 min → fibrinolysis
Step 2 - Bedside Assessment (Urgent)
- BP in both arms, check for hypotension
- SpO2 - give O2 only if <94%
- Right-sided ECG (V3R-V4R) - MANDATORY to rule out RV infarction (ST elevation in V4R confirms RV MI)
- IV access x2, continuous cardiac monitoring
Step 3 - Medications
| Drug | Dose | Notes |
|---|---|---|
| Aspirin | 325 mg loading PO stat | Chew, do not swallow whole |
| P2Y12 inhibitor | Ticagrelor 180 mg OR Clopidogrel 600 mg | Per local PCI protocol |
| Anticoagulation | UFH 60 U/kg IV (max 4000 U) bolus | Or enoxaparin per protocol |
| Morphine | Use cautiously | Can delay P2Y12 absorption |
| Nitroglycerin | WITHHOLD if hypotension or RV infarction suspected | RV is preload-dependent; NTG can cause catastrophic BP drop |
"If hypotension is present or is anticipated to occur (i.e., inferior wall STEMI with identified or suspected right ventricular infarction), it is very appropriate to withhold NTG in all formulations."
- Rosen's Emergency Medicine
Step 4 - If RV Infarction Confirmed
- IV fluid challenge: 500 mL NS bolus (RV needs preload)
- Avoid diuretics, NTG, morphine
- Watch for complete heart block (RCA supplies AV node - may need temporary pacing)
Step 5 - Labs (Stat)
- Troponin I/T (high-sensitivity), serial at 0 and 1-2 hrs
- BMP/electrolytes, CBC, coagulation
- Echo ASAP (wall motion abnormality will confirm inferior/posterior involvement)
Differential to Keep in Mind (Lower Priority)
- Acute coronary vasospasm (Prinzmetal) - possible but less likely given age and hypertension
- Food poisoning alone - EXCLUDED by ECG findings
- Hypertensive emergency with demand ischemia - less likely given the focused inferior pattern
Bottom Line
This is an Inferior STEMI in a 53-year-old hypertensive woman presenting atypically with GI symptoms - a well-recognized masquerade. The Bezold-Jarisch reflex explains all her symptoms. The ECG shows ST elevation in II/III/aVF with reciprocal aVL depression; ST III > ST II suggests RCA culprit; V1-V2 changes warrant right-sided leads to exclude RV MI.
Do not give nitrates until RV involvement is excluded. Do not delay reperfusion for GI workup.
- Rosen's Emergency Medicine (9e), Electrocardiographic Abnormalities in ACS, p. 1005-1006
- Rosen's Emergency Medicine (9e), Pharmacologic Intervention in ACS, p. 1025
This is a shared conversation. Sign in to Orris to start your own chat.