explain step by step sensory examination demonstartion with expanation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
sensory examination dermatomes neurological testing
Here is a comprehensive, step-by-step guide to performing a sensory examination, drawn from Adams and Victor's Principles of Neurology (12th Edition) and Harrison's Principles of Internal Medicine (22nd Edition).
Sensory Examination — Step-by-Step Guide
Before You Begin: General Principles
- Question the patient first — Ask about any changes in sensation: numbness, tingling, burning, "dead" feeling, pins and needles, or unusual sensory experiences. Patients may confuse weakness with numbness.
- Explain the procedure simply — Tell the patient what you are doing in plain terms. Instruct them to say "yes" or "sharp" when they feel something rather than answering "Do you feel that?" each time — this avoids suggestion.
- Eyes closed — The patient should keep their eyes closed (or look away) throughout the examination to prevent visual cueing.
- Do not over-fatigue the patient — Avoid prolonged testing in a tired patient; results become unreliable.
- Compare both sides — Always test symmetrical areas on both sides of the body.
- Proceed from abnormal to normal — It is easier for the patient to identify the boundary of a numb area when you move from the reduced-sensation zone toward the normal area.
- Scope of testing — In a patient with no sensory complaints: a brief screen (vibration, position sense, pinprick in hands and feet + Romberg) is sufficient. In a patient with sensory symptoms or signs: full testing of all modalities is required.
The Five Primary Sensory Modalities
STEP 1 — Light Touch
How to test:
- Use a wisp of cotton, a tissue, or light fingertip touch.
- Demonstrate the sensation first on a normal area of skin so the patient knows what to expect.
- Ask the patient (eyes closed) to say "yes" each time they feel a touch.
- Touch various areas, including suspected abnormal regions.
- Apply a moving stimulus — patients are more sensitive to a moving touch than a stationary one.
- On calloused skin (palms, soles), a slightly firmer stimulus is needed. On hair-covered skin, a lighter touch suffices due to rich nerve endings around hair follicles.
- Avoid testing only on hairy skin due to abundant sensory endings.
What you are testing: Large myelinated fibers → posterior columns (lemniscal pathway)
STEP 2 — Pain Sensation (Superficial)
How to test:
- Use a clean, new pin (discarded after each patient).
- Ask the patient (eyes closed) to focus on the pricking or unpleasant quality — not just the touch or pressure.
- Compare symmetrical areas of the body, proximal to distal.
- If an area of hyalgesia (reduced pain) is found, map it by moving radially outward from the most hyalgesic point.
- Avoid repeated pinpricks in a small area — this causes temporal summation and can mask subtle hyalgesia.
- If overinterpretation is suspected, switch to warm/cold discrimination as a more objective alternative.
What you are testing: Small A-δ and C fibers → spinothalamic tract (contralateral)
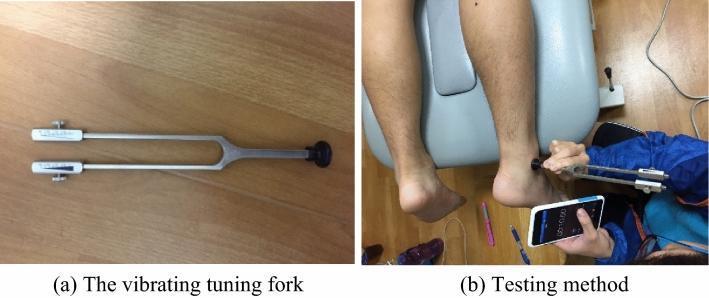
STEP 3 — Temperature Sensation
How to test:
- Quick method: Rub one side of a tuning fork briskly against your palm to warm it. Apply the warm and cool sides alternately to the patient's skin — ask "which is cooler/warmer?"
- Formal method: Use two stoppered test tubes — one with warm water (~45°C) and one with cold (~20°C). Apply the side of each tube to the skin for a few seconds; ask whether the object feels "less hot" or "less cold" compared to a normal area.
- Alternatively, a metal tuning fork at room temperature can test cold; warmed metal can test warmth.
- Both cold AND warmth should be tested as different receptors respond to each.
What you are testing: Small fibers → spinothalamic tract (contralateral)
STEP 4 — Vibration Sense
How to test:
- Use a 128-Hz tuning fork.
- Strike the fork to set it vibrating, then apply the base (handle end) to a bony prominence, beginning distally:
- Feet: dorsal surface of the distal phalanx of the big toe, then the medial and lateral malleoli
- Hands: dorsal surface of the distal phalanx of the index finger
- Ask the patient to say when they feel the vibration begin, and when it stops.
- The examiner places their own finger on the opposite side of the joint to compare their own vibration threshold to the patient's — a useful control.
- If abnormalities are found distally, move to more proximal bony points (wrist, elbow, knee, hip, spine).
What you are testing: Large myelinated fibers, especially Pacinian corpuscles → posterior columns (ipsilateral)
STEP 5 — Joint Position Sense (Proprioception)
How to test:
- Start with the distal interphalangeal (DIP) joint of the great toe or index finger.
- Grasp the digit at the sides (not top and bottom), perpendicular to the plane of movement. Stabilize more proximal joints.
- Move the digit passively up or down by small increments (1–2 mm excursions can normally be detected).
- Ask the patient to say "up" or "down" with each movement (eyes closed).
- If errors occur distally, test progressively more proximal joints (ankle, knee, wrist, elbow, shoulder).
- A useful proximal test: Ask the patient to extend both arms and bring their index fingers together with eyes closed. Normal individuals achieve this with errors of ≤1 cm.
What you are testing: Muscle spindles, joint capsule receptors, Golgi tendon organs → posterior columns (ipsilateral)
STEP 6 — The Romberg Test (Proprioception Screening)
How to perform:
- Ask the patient to stand with feet as close together as needed to maintain balance while eyes are open.
- Then ask them to close their eyes.
- A positive Romberg (loss of balance with eyes closed) indicates impaired proprioception.
A Romberg test primarily reveals a posterior column or peripheral proprioceptive deficit — cerebellar ataxia, by contrast, is present even with eyes open.
STEP 7 — Cortical (Discriminative) Sensation
These tests require intact primary sensation. They evaluate parietal lobe integration. Always compare both sides.
a) Two-Point Discrimination
- Use calipers set at various widths (2 mm to several cm).
- Apply two points simultaneously to the test site.
- On fingertips, normal individuals distinguish two points ≥3 mm apart as separate.
- Inability = impaired parietal cortex function.
b) Touch Localization
- Apply light pressure briefly with fingertip or cotton wool.
- Ask the patient (eyes closed) to point to where they were touched.
- Errors suggest a parietal lesion.
c) Bilateral Simultaneous Stimulation (Extinction)
- Lightly touch one or both hands simultaneously.
- Ask the patient (eyes closed) to identify where they are being touched.
- If the patient consistently fails to perceive the stimulus on one side when both sides are touched simultaneously → sensory extinction/neglect, suggesting a contralateral parietal lobe lesion.
d) Graphesthesia
- With the patient's eyes closed, trace a number or letter on the palm of their hand using your fingertip (letters should be >4 cm; on the fingertip, 1 cm numbers can normally be detected).
- Ask the patient to identify it.
- Inability = agraphesthesia — a sign of parietal cortex dysfunction.
e) Stereognosis
- Place a common object (key, coin, paper clip) in the patient's hand with eyes closed.
- Ask them to identify it by feel (shape, texture, size).
- Normal: can distinguish a dime from a penny, a nickel from a quarter.
- Inability = astereognosis — implies contralateral parietal lobe or thalamocortical pathway lesion.
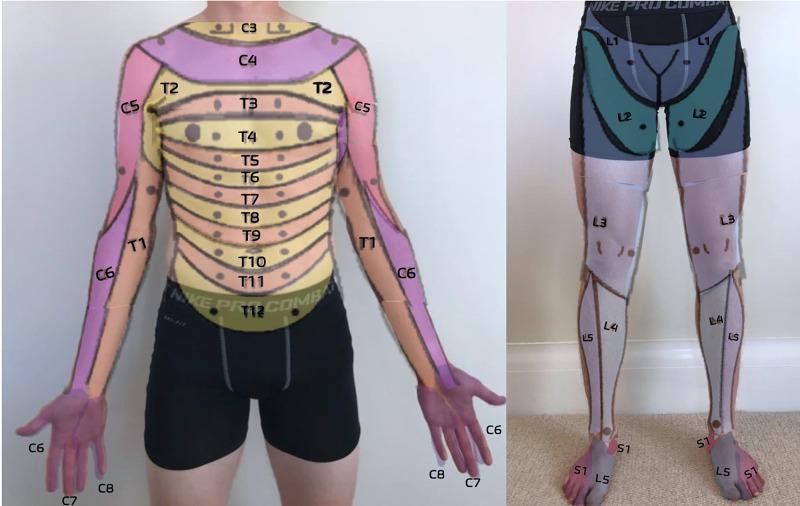
Dermatomal Reference Map
Summary Table
| Modality | Tool | Pathway | Clinical Significance |
|---|---|---|---|
| Light touch | Cotton wisp / finger | Posterior columns (and spinothalamic) | Peripheral neuropathy, posterior column disease |
| Pain (pinprick) | New pin | Spinothalamic (contralateral) | Syringomyelia, Brown-Séquard, peripheral neuropathy |
| Temperature | Test tubes / tuning fork | Spinothalamic (contralateral) | Small-fiber neuropathy, syringomyelia |
| Vibration | 128-Hz tuning fork | Posterior columns (ipsilateral) | B12 deficiency, tabes dorsalis, peripheral neuropathy |
| Joint position | Passive digit movement | Posterior columns (ipsilateral) | Proprioceptive ataxia, posterior column lesions |
| Romberg | Standing with eyes closed | Posterior columns / vestibular | Sensory vs. cerebellar ataxia |
| Two-point discrimination | Calipers | Parietal cortex | Parietal lobe lesion |
| Graphesthesia | Fingertip on palm | Parietal cortex | Agraphesthesia in parietal lesions |
| Stereognosis | Object in hand | Parietal cortex | Astereognosis in parietal/thalamocortical lesions |
Special Notes
- Effect of age: Vibration sense is the first to decline with aging, followed by proprioception and touch — especially in the feet. Do not over-attribute sensory loss to aging without ruling out treatable causes.
- Uncooperative patient: Reduce testing to observing withdrawal responses to noxious stimuli (pinch), and use balance/gait to infer proprioceptive function.
- Spinal cord lesions: Test all modalities, look for a sensory level, and compare root/dermatomal distributions.
- Cortical lesions: Screen primary modalities first — cortical sensory tests are only valid when primary sensation is intact.
- Recording: Document findings in narrative form or shade affected regions on a body diagram.
Sources: Adams and Victor's Principles of Neurology, 12th Edition | Harrison's Principles of Internal Medicine, 22nd Edition
This is a shared conversation. Sign in to Orris to start your own chat.