PI in Color doppler week wise normal ratio in pregnancy
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Searching Images
pulsatility index normal values gestational age weeks pregnancy color doppler chart
Here is a comprehensive reference for Pulsatility Index (PI) — Normal Values by Gestational Week in Color Doppler during pregnancy, covering the three most clinically important vessels:
Pulsatility Index (PI) — Normal Values in Pregnancy
Formula: PI = (PSV − EDV) / TAV (time-averaged velocity)
PI decreases as pregnancy advances, reflecting progressively lower placental resistance and improved diastolic flow.
1. Umbilical Artery (UA) PI — Normal Reference
The umbilical artery PI steadily falls with advancing gestation as trophoblastic invasion reduces placental resistance.
| Gestational Week | PI (Mean) | PI (5th–95th Percentile) |
|---|---|---|
| 20 | ~1.60 | 1.20 – 2.00 |
| 22 | ~1.50 | 1.15 – 1.90 |
| 24 | ~1.40 | 1.10 – 1.75 |
| 26 | ~1.30 | 1.00 – 1.65 |
| 28 | ~1.20 | 0.95 – 1.55 |
| 30 | ~1.10 | 0.88 – 1.45 |
| 32 | ~1.05 | 0.80 – 1.35 |
| 34 | ~1.00 | 0.75 – 1.30 |
| 36 | ~0.95 | 0.70 – 1.25 |
| 38 | ~0.90 | 0.65 – 1.20 |
| 40 | ~0.85 | 0.60 – 1.15 |
From the textbook image (Creasy & Resnik): at 21 weeks PI ≈ 1.20, declining to ≈ 0.94 by 30 weeks.
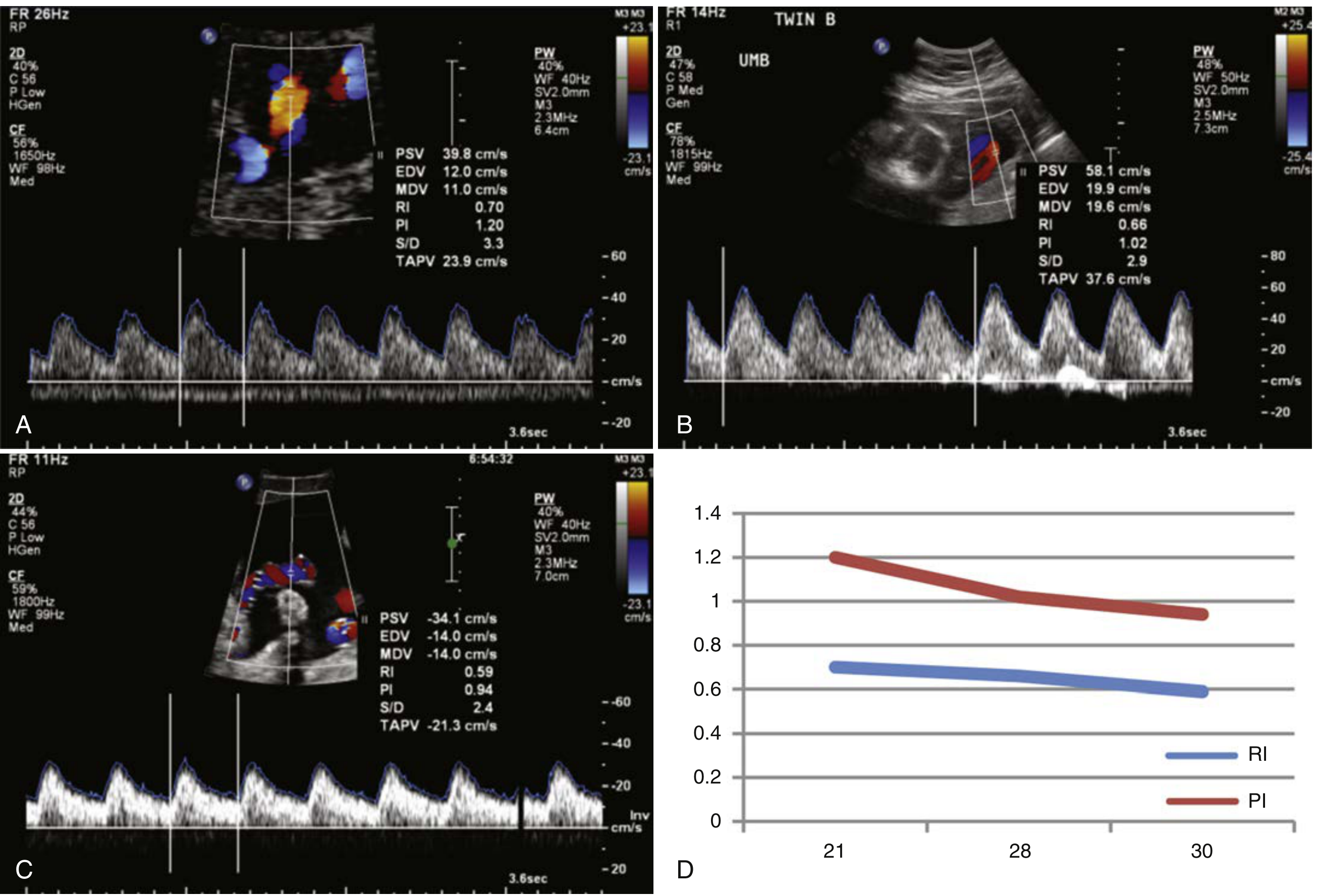
Umbilical artery RI and PI values 21–30 weeks (panel D). RI (blue) ~0.70→0.59; PI (red) ~1.20→0.94 — Creasy & Resnik's Maternal-Fetal Medicine
2. Uterine Artery (UtA) PI — Normal Reference
Uterine artery PI falls sharply between 11–24 weeks as trophoblast invades the spiral arteries. A bilateral notch with PI >95th percentile at 20–24 weeks predicts preeclampsia/FGR.
| Gestational Week | Mean PI | 95th Percentile (Abnormal Threshold) |
|---|---|---|
| 11–13+6 (1st trimester) | ~2.35 | >2.35 (used in FMF screening) |
| 20–22 | ~1.20 | >1.45 |
| 22–24 | ~1.10 | >1.45 |
| 24–26 | ~1.05 | >1.40 |
| 28–32 | ~0.90 | >1.20 |
| 34–40 | ~0.80 | >1.10 |
A PI >95th percentile at 20–24 weeks, especially with bilateral notching, is a major risk marker for preeclampsia and IUGR. — Creasy & Resnik's Maternal-Fetal Medicine
The image below shows an elevated uterine artery PI of 1.75 at 22–24 weeks (above the 95th percentile of 1.45), with an early diastolic notch:
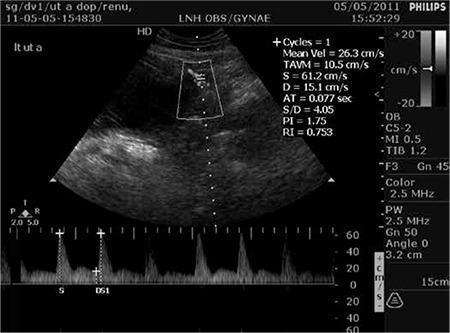
Uterine artery PI 1.75 (>95th percentile), with early diastolic notch — associated with impaired uteroplacental perfusion
3. Middle Cerebral Artery (MCA) PI — Normal Reference
MCA PI is high normally (reflecting high cerebrovascular resistance). It falls with fetal hypoxia — the "brain-sparing" effect. MCA PI < 5th percentile = abnormal.
| Gestational Week | Mean PI | 5th Percentile (Abnormal = Below) |
|---|---|---|
| 20 | ~1.85 | ~1.45 |
| 24 | ~1.90 | ~1.50 |
| 28 | ~1.90 | ~1.55 |
| 30 | ~1.85 | ~1.50 |
| 32 | ~1.75 | ~1.40 |
| 34 | ~1.65 | ~1.30 |
| 36 | ~1.55 | ~1.20 |
| 38 | ~1.45 | ~1.10 |
| 40 | ~1.35 | ~1.00 |
4. Ductus Venosus (DV) PI — Normal Reference
DV PI assesses venous return and cardiac function. Elevated DV PI or absent/reversed a-wave = severe fetal compromise.
| Gestational Week | Mean PI | Upper Limit (95th Percentile) |
|---|---|---|
| 20–24 | ~0.55 | ~0.75 |
| 28–32 | ~0.50 | ~0.70 |
| 34–38 | ~0.45 | ~0.65 |
Key Clinical Points
| Finding | Interpretation |
|---|---|
| UA PI >95th percentile | Elevated placental resistance → FGR risk |
| UA absent/reversed end-diastolic flow | Severe FGR, imminent fetal compromise |
| UtA PI >1.45 at 20–24 wks + notch | Risk of preeclampsia, IUGR |
| MCA PI <5th percentile ("brain sparing") | Fetal hypoxia redistributing blood to brain |
| MCA PI/UA PI ratio (CPR) <1.0 | Cerebro-placental ratio — poor fetal outcome |
| DV reversed a-wave | Cardiac decompensation, delivery indicated |
Reference: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Swanson's Family Medicine Review
Explain early diastolic notch and its cler diagram
Finding Sources
Searching Images
uterine artery early diastolic notch doppler waveform diagram
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a complete explanation of the early diastolic notch in uterine artery Doppler:
Early Diastolic Notch — Uterine Artery Doppler
What Is It?
The early diastolic notch (also called protodiastolic notch) is a brief, transient dip in flow velocity that occurs immediately after the systolic peak and before the diastolic phase in the uterine artery Doppler waveform.
It represents a momentary reversal or sharp deceleration of blood flow velocity at the start of diastole — a reflection of high vascular resistance in the uteroplacental circulation.
Normal vs. Abnormal — The Physiology
In Normal Pregnancy:
During early pregnancy, the uterine arteries are high-resistance vessels. Between 16–22 weeks, trophoblast cells invade the spiral arteries, replacing their muscular walls with wide, low-resistance channels. This process is called physiological conversion of spiral arteries.
- Result: Uterine artery resistance falls progressively
- The diastolic notch disappears by 24 weeks in normal pregnancy
- Forward diastolic flow increases throughout pregnancy
When the Notch Persists:
If trophoblastic invasion is incomplete or absent, spiral arteries retain their muscular walls → remain high-resistance → the uterine artery shows:
- Elevated PI/RI
- Persistent diastolic notch beyond 24 weeks → abnormal
Diagrams
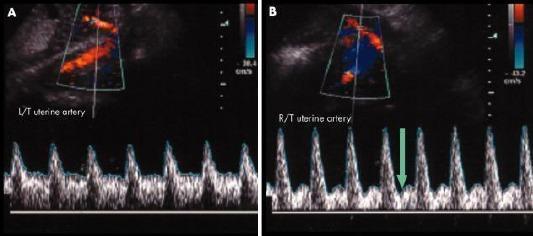
Panel A = NORMAL uterine artery — sharp systolic peaks, smooth continuous diastolic flow, NO notch.
Panel B = ABNORMAL — prominent early diastolic notch (green arrow), high resistance pattern:
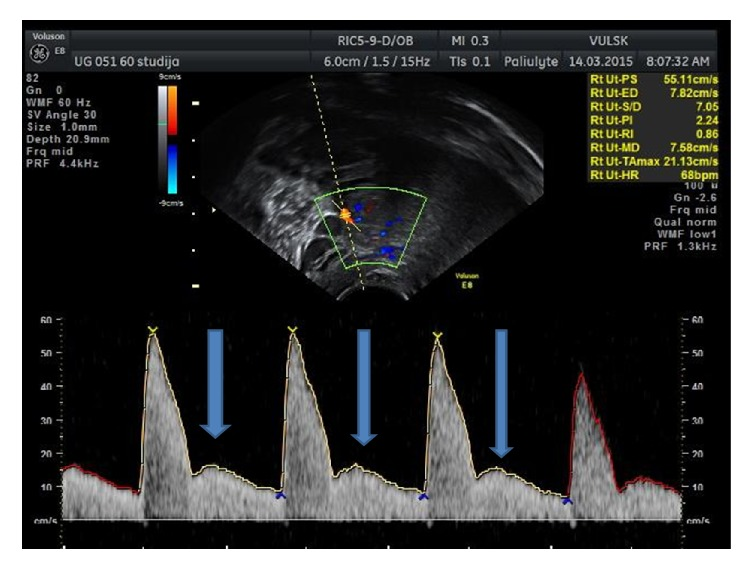
Prominent bilateral diastolic notch — blue arrows mark the notch dip after each systolic peak. PI = 2.24, RI = 0.86 (markedly elevated):
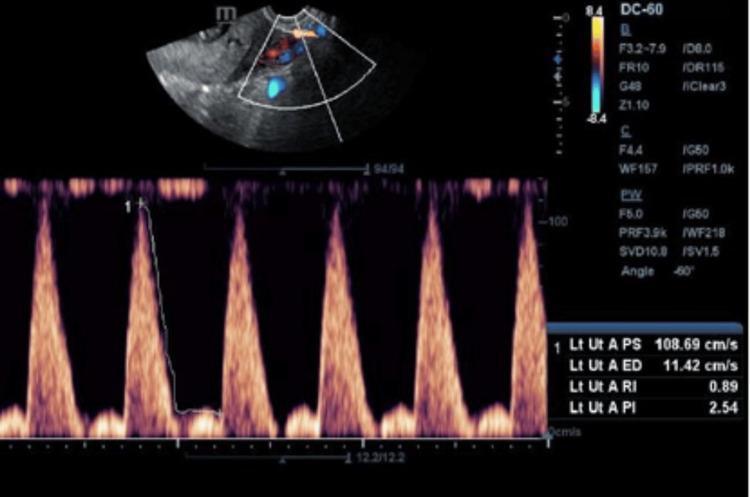
Left uterine artery with notch — PI 2.54, RI 0.89, PSV 108.69 cm/s, EDV 11.42 cm/s. Severely high resistance with prominent notch after each systolic peak:
Waveform Anatomy — Labeled
Velocity
↑
| /\
| / \
| / \___↓(NOTCH)___/‾‾‾‾\_____
| / diastole
|/__________________________ time →
↑ ↑
Systolic Notch = early diastolic dip
peak (high resistance marker)
| Part of Waveform | What It Represents |
|---|---|
| Rapid upstroke | Systolic ejection — cardiac contraction |
| Peak (PSV) | Peak systolic velocity |
| Sharp downtroke | Deceleration after systole |
| Notch/dip | Transient flow reversal = high resistance |
| Post-notch rise | Diastolic flow — reflects downstream compliance |
| EDV (trough) | End-diastolic velocity — reflects placental resistance |
Clinical Significance
| Finding | Interpretation |
|---|---|
| Notch disappears by 20–22 wks | Normal trophoblast invasion — good |
| Unilateral notch at 22–24 wks | Borderline — repeat in 4 weeks |
| Bilateral notch persisting >24 wks | Abnormal — failed spiral artery remodeling |
| Notch + PI >95th percentile | High risk for preeclampsia + IUGR |
| Notch + elevated AFP/low PAPP-A | Risk also for placental abruption |
Associated Conditions (Persistent Notch)
- Preeclampsia — most strongly associated
- Intrauterine Growth Restriction (IUGR/FGR)
- Placental abruption
- Stillbirth / perinatal death
"Persistent notching of the waveform after 24 weeks was associated with increased risk for abruption as well as IUGR and preeclampsia." — Creasy & Resnik's Maternal-Fetal Medicine
Screening Use (First Trimester)
At 11–13+6 weeks, uterine artery PI >95th percentile (>~2.35) combined with PAPP-A <10th percentile and maternal risk factors forms the FMF combined screening algorithm for early-onset preeclampsia, with sensitivity ~75–90% for early preeclampsia at 10% FPR.
This is a shared conversation. Sign in to Orris to start your own chat.