Bile acid secretion and function
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive material from multiple authoritative textbooks. I can compose the full answer.
Bile Acid Secretion and Function
1. What Are Bile Acids?
Bile is a complex lipid-rich micellar solution, isotonic with plasma, secreted by the liver at a rate of 500-600 mL/day. Its major organic components by molar percentage are:
- Bile acids - 80%
- Phospholipids (lecithin, cephalins, sphingomyelin) - 16%
- Unesterified cholesterol - 4% (rising to 8-10% in the lithogenic state)
Other constituents include conjugated bilirubin, immunoglobulins, albumin, electrolytes, mucus, heavy metals, and drug metabolites.
(Sleisenger and Fordtran's GI and Liver Disease, Ch. 64; Harrison's Principles 22E)
2. Synthesis of Bile Acids
Primary Bile Acids
Bile acids are synthesized exclusively in hepatocytes from cholesterol, removing about 1-2 g of cholesterol from plasma daily. The two primary bile acids are:
- Cholic acid (CA) - trihydroxy
- Chenodeoxycholic acid (CDCA) - dihydroxy
Two Biosynthetic Pathways
| Pathway | Key Enzyme | Notes |
|---|---|---|
| Classical (neutral) | Cholesterol 7α-hydroxylase (CYP7A1) - rate-limiting | Predominant; produces CA and CDCA |
| Alternative (acidic) | Sterol 27-hydroxylase (CYP27A1) | Minor; regulated post-transcriptionally |
Conjugation
Before leaving the liver, primary bile acids are conjugated with taurine or glycine (amidation) via:
- Bile acid-CoA ligase (SLC27A5/FATP5)
- Bile acid-CoA:amino acid N-acyltransferase (BAAT)
Conjugation dramatically lowers the pKa, keeping bile acids ionized and water-soluble at intestinal pH - this prevents their passive reabsorption in the small bowel, maintaining high luminal concentrations needed for micelle formation.
Secondary Bile Acids
In the colon, intestinal bacteria deconjugate and dehydroxylate primary bile acids to form secondary bile acids:
- Deoxycholic acid (DCA) - from CA (7α-dehydroxylation)
- Lithocholic acid (LCA) - from CDCA (7α-dehydroxylation; largely insoluble and excreted)
(Harrison's Principles 22E; Sleisenger & Fordtran; Lippincott's Biochemistry 8th Ed)
3. Bile Secretion - Two-Stage Process
Bile is secreted in two stages (Guyton & Hall, Medical Physiology):
Stage 1: Hepatocyte Canalicular Secretion
Hepatocytes actively secrete bile into bile canaliculi between adjacent hepatocytes. This is the primary stage. Canalicular bile formation is classically divided into:
- Bile acid-dependent flow (~60%) - active pumping of bile acids into the canalicular lumen creates an osmotic gradient that drives water entry
- Bile acid-independent flow (~40%) - active secretion of reduced glutathione (GSH via MRP2/ABCC2) and bicarbonate (HCO3- via AE2 Cl-/HCO3- exchanger) also contribute osmotic driving force
Primary solutes (bile acids, GSH, conjugated bilirubin) actively pumped across the canalicular membrane generate bile flow. Secondary solutes (water, electrolytes, glucose, amino acids) follow passively down the osmotic gradient.
Stage 2: Ductal Modification by Cholangiocytes
As bile flows through bile ducts, cholangiocytes modify its composition by:
- Absorbing glucose, amino acids, some bile acids
- Secreting bicarbonate and chloride (a secretin-stimulated, cAMP-dependent process)
- Moving water through aquaporins and paracellularly
Ductal secretion can account for up to 30% of bile flow in humans. Secretin is the major stimulus, releasing additional NaHCO3 to neutralize gastric acid entering the duodenum.
(Sleisenger & Fordtran; Guyton & Hall; Harrison's)
4. Key Canalicular Transport Proteins (ABC Transporters)
| Transporter | Gene | Substrate |
|---|---|---|
| BSEP (Bile Salt Export Pump) | ABCB11 | Conjugated bile salts (primary driver) |
| MRP2 (Anionic conjugate pump) | ABCC2 | Bilirubin glucuronides, GSH, drug conjugates |
| MDR1 | ABCB1 | Hydrophobic compounds, drugs |
| MDR3 (Phospholipid pump) | ABCB4 | Phosphatidylcholine (into bile) |
| ABCG5/G8 | ABCG5/G8 | Cholesterol and phytosterols |
At the sinusoidal (basolateral) side, hepatocytes take up bile acids via:
- NTCP (Na+/taurocholate cotransporter, SLC10A1) - Na+-dependent
- OATP1B1/1B3 - Na+-independent organic anions
(Harrison's Principles 22E; Sleisenger & Fordtran Ch. 64)
5. The Gallbladder
The liver secretes bile continuously, but most is stored in the gallbladder (capacity 30-60 mL) until needed. The gallbladder concentrates bile 5- to 20-fold by actively absorbing Na+, followed by passive reabsorption of Cl-, water and small electrolytes. Total solute concentration rises from 3-4 g/dL (hepatic bile) to 10-15 g/dL (gallbladder bile).
Release is triggered by cholecystokinin (CCK), released from duodenal mucosa in response to fats and amino acids. CCK causes:
- Powerful gallbladder contraction
- Relaxation of the sphincter of Oddi
- Enhanced bile flow into the duodenum
In the fasting state, the entire bile acid pool may be sequestered in the gallbladder overnight.
6. Enterohepatic Circulation
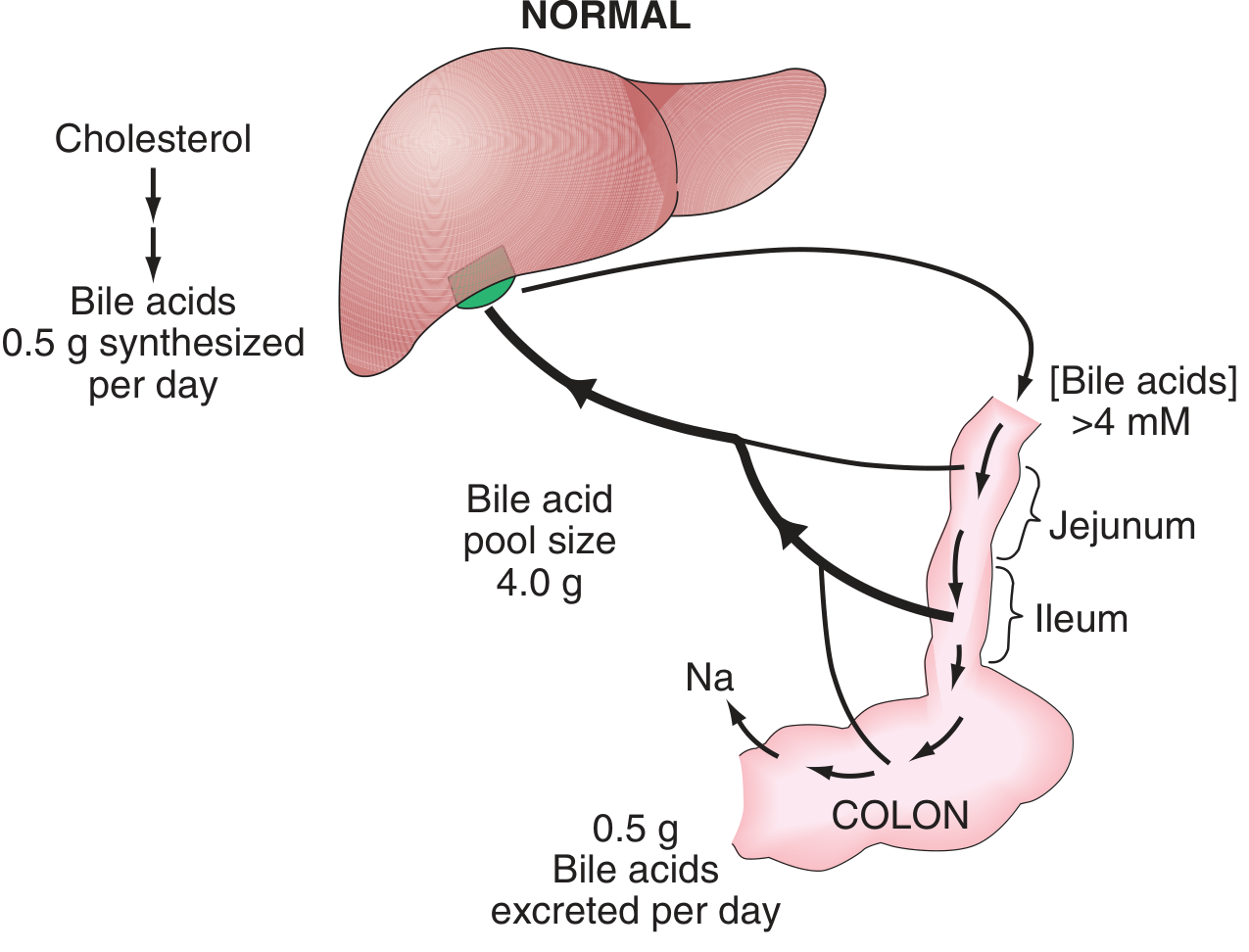
The enterohepatic circulation is a highly efficient recycling system:
| Parameter | Value |
|---|---|
| Total bile acid pool | ~2-4 g |
| Daily cycles | 5-10 per day |
| Intestinal reabsorption efficiency | ~95% |
| Daily fecal loss | 0.2-0.5 g |
| Daily hepatic synthesis (to replenish) | ~0.5 g (max ~5 g/day) |
Route of reabsorption:
- Most bile acids are absorbed in the terminal ileum via the apical sodium-dependent bile acid transporter (ASBT/SLC10A2) - an active, Na+-dependent process
- ~15% undergo bacterial deconjugation in the small intestine and may be passively absorbed or pass to the colon
- Deconjugated/dehydroxylated secondary bile acids are partially absorbed from the colon
- Reabsorbed bile acids travel via the portal vein back to the liver for re-uptake and re-secretion (first-pass extraction ~50-90%)
(Harrison's Principles 22E; Sleisenger & Fordtran)
7. Functions of Bile Acids
A. Fat Digestion and Absorption
Bile acids perform two essential roles:
- Emulsification - break large fat globules into small particles (~1 µm), vastly increasing the surface area for pancreatic lipase action
- Micelle formation - at concentrations exceeding the critical micellar concentration (CMC ~2-4 mM), bile acids form mixed micelles with phospholipids, monoglycerides, fatty acids, and fat-soluble vitamins (A, D, E, K). These micelles ferry lipid products to the brush border for absorption. Without bile acids, fat-soluble vitamins are poorly absorbed.
B. Cholesterol Homeostasis
- Bile acid synthesis represents cholesterol catabolism - the primary route for irreversible cholesterol elimination
- Bile acids facilitate absorption of biliary and dietary cholesterol via mixed micelles
- Bile acid secretion accounts for ~50% of daily cholesterol elimination
- In the gallbladder, bile salts + lecithin keep cholesterol solubilized; imbalance leads to cholesterol precipitation and gallstone formation
C. Bile Formation and Hepatic Excretion
- The active transport of bile acids into canaliculi is the primary driving force for bile flow (bile acid-dependent fraction)
- Bile serves as the excretory route for bilirubin, heavy metals, drug metabolites, and xenobiotics
D. Signaling - Bile Acids as Hormones
Bile acids act as ligands for nuclear and membrane-bound receptors that regulate metabolism:
| Receptor | Type | Key Actions |
|---|---|---|
| FXR (Farnesoid X Receptor, NR1H4) | Nuclear | Master regulator of bile acid synthesis; activates SHP to inhibit CYP7A1; upregulates BSEP; represses bile acid synthesis |
| TGR5 (GPBAR1) | G-protein-coupled | Stimulates GLP-1 release from intestinal L-cells (glucose homeostasis); induces thyroid hormone activation in brown adipose tissue; regulates intestinal motility |
| PXR, VDR, CAR | Nuclear | Detoxification of secondary bile acids (notably LCA) |
FGF19 feedback loop: Bile acids in the ileum activate FXR → ileal FGF19 release → FGF19 binds hepatic FGFR4/β-klotho complex → inhibits CYP7A1 → suppresses bile acid synthesis. This is the key postprandial feedback mechanism.
(Sleisenger & Fordtran; Harrison's 22E)
8. Regulation Summary
| Regulator | Effect on Bile Acid Synthesis |
|---|---|
| FXR (activated by bile acids) | ↓ via SHP-mediated CYP7A1 inhibition |
| FGF19 (ileal, postprandial) | ↓ via hepatic FGFR4/β-klotho |
| LXR (oxysterol sensor) | ↑ CYP7A1 (in rodents); regulates ABCG5/G8 |
| HNF4α, LRH-1 | ↑ CYP7A1 (positive regulators) |
| Cholesterol availability | ↑ provides substrate |
9. Clinical Consequences of Bile Acid Deficiency
When bile acid synthesis, secretion, or reabsorption is disrupted:
| Process | Pathologic Defect | Disease Example |
|---|---|---|
| Synthesis | Decreased hepatic function | Cirrhosis, bile acid synthesis defects |
| Biliary secretion | Altered canalicular function (BSEP mutations) | Primary biliary cholangitis, PFIC |
| Conjugation maintenance | Bacterial overgrowth | Jejunal diverticulosis, SIBO |
| Ileal reabsorption | Abnormal ileal function | Crohn's disease, ileal resection |
Consequences include: steatorrhea, fat-soluble vitamin deficiency (A, D, E, K), bile acid diarrhea (from colonic bile acid excess), gallstone formation, and - in synthesis defects - progressive cholestatic liver disease.
Key references:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 64 (Bile Acids)
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapters 336 & 338
- Guyton and Hall Textbook of Medical Physiology, Chapter 65
- Lippincott's Illustrated Reviews: Biochemistry, 8th Ed., Chapter on Cholesterol Metabolism
This is a shared conversation. Sign in to Orris to start your own chat.