Stye eye treatment
Reading File
Finding Sources
Searching Images
stye hordeolum eye treatment
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information. Let me compile the answer with the clinical images.
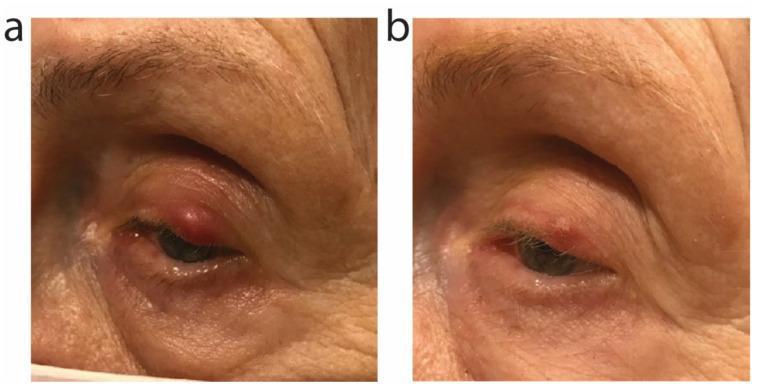
Stye (Hordeolum) — Treatment
A stye (hordeolum) is an acute bacterial abscess of a meibomian, Zeis', or Moll's gland in the eyelid, most commonly caused by Staphylococcus aureus. It is classified as external (pointing toward the skin) or internal (pointing toward the conjunctiva).

First-Line: Medical Management
Most hordeola resolve with conservative care in 5–7 days:
| Treatment | Details |
|---|---|
| Warm compresses | Apply for 10–15 min, 4× daily — promotes spontaneous drainage |
| Lid hygiene / scrubs | Cleanse lid margins nightly with diluted baby shampoo (1:1 with water) on a cotton swab, or use commercial ocular cleansing pads |
| Topical antibiotic ointment | Erythromycin ointment applied to the lid margin after washing |
| Oral antibiotics | Directed against Staphylococcus (e.g., dicloxacillin, amoxicillin-clavulanate, or doxycycline) — indicated when cellulitis is present or the lesion is not yet "pointing" |
The hordeolum typically drains spontaneously once it points, relieving symptoms. Monitor closely if treating medically.
When to Proceed to Incision & Drainage (I&D)
I&D is indicated when:
- The hordeolum fails medical management
- It causes significant pain
- There is a significant localized pus collection
- There is eyelid cellulitis associated with the lesion
Contraindication: If located nasal to the medial canthus (near the lacrimal punctum), refer to ophthalmology — risk of damaging the lacrimal drainage system. (Dacryocystitis at that location can track to the cavernous sinus.)
I&D Procedure (when needed)
- Instill topical ophthalmic anesthetic (e.g., tetracaine drops)
- Inject 2% lidocaine with epinephrine via 30-gauge needle at the lesion
- Incise from whichever surface (skin or conjunctival) gives best access, using a no. 11 scalpel blade
- Express pus with gentle pressure; use cotton swabs to clean the cavity
- Post-procedure: Apply antibiotic ointment (e.g., erythromycin) twice daily until resolved
Differentiating from Chalazion
| Feature | Hordeolum (Stye) | Chalazion |
|---|---|---|
| Onset | Acute | Subacute/chronic |
| Tenderness | Marked | Mild or absent |
| Fluctuance | Yes (abscess) | May have soft centre, not pus |
| Cellulitis | Common | Less common |
| Cause | Bacterial (acute abscess) | Lipogranulomatous (blocked meibomian gland) |
Red Flags — Refer urgently if:
- Swelling is nasal to the medial canthus (may be dacryocystitis)
- Signs of orbital cellulitis: proptosis, restricted eye movements, high fever, systemic toxicity
- Vision changes
— Pfenninger and Fowler's Procedures for Primary Care, p. 456–460; Kanski's Clinical Ophthalmology, p. 66
Moxiflox eye drops dose
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I have the authoritative data. Here's the answer:
Moxifloxacin Ophthalmic Eye Drops — Dosing
| Parameter | Detail |
|---|---|
| Concentration | 0.5% (5 mg/mL) |
| Standard dose | 1 drop twice daily (b.i.d.) × 7 days |
This is the standard regimen for bacterial conjunctivitis and routine eye infections.
Indication-Based Dosing
| Indication | Regimen |
|---|---|
| Bacterial conjunctivitis | 1 drop b.i.d. × 7 days |
| Corneal ulcer / keratitis | More intensive: 1 drop every 1–2 hours while awake (then taper) — ophthalmologist-directed |
| Post-procedure prophylaxis (e.g., paracentesis) | Single drop instilled immediately after procedure, then q.i.d. × 4–7 days |
Key Points
- Moxifloxacin 0.5% is a 4th-generation fluoroquinolone with broad-spectrum coverage including Staphylococcus, Streptococcus, Haemophilus, and Pseudomonas
- It is preservative-free (brand: Vigamox), making it well tolerated
- Compared to older fluoroquinolones (ciprofloxacin, ofloxacin), it does not require the intensive loading dose (q2h × 48h) — the b.i.d. schedule is simpler
- Do not use contact lenses during active infection/treatment
Compared regimen from the same table — Gatifloxacin 0.5% requires 1 drop q2h × 24h, then qid × 6 days, making moxifloxacin's b.i.d. schedule a simpler alternative.
— Goldman-Cecil Medicine, Table 391-7, p. 4130
This is a shared conversation. Sign in to Orris to start your own chat.