Pancreatitis
Reading File
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks and pathology images. Here is the full structured answer:
Pancreatitis
Pancreatitis is inflammation of the pancreas, classified into acute and chronic forms. In acute pancreatitis (AP), function returns to normal if the cause is removed; chronic pancreatitis causes irreversible exocrine destruction.
1. Anatomy Recap
The pancreas is a retroperitoneal organ with head (nestled in the duodenal C-loop), body (posterior to the stomach), and tail (reaching the splenic hilum). The main pancreatic duct (duct of Wirsung) meets the common bile duct at the ampulla of Vater, draining through the sphincter of Oddi into the duodenum. - Rosen's Emergency Medicine, p. 1265
2. Pathophysiology
An inciting event (gallstone obstruction, alcohol, drug toxicity) disrupts normal membrane trafficking in acinar cells. This triggers:
- Inappropriate activation of trypsinogen → trypsin - activating other digestive enzymes
- Autodigestion of pancreatic parenchyma and surrounding fat
- Inflammatory cascade - macrophage and neutrophil recruitment, cytokine release
- Increased vascular permeability - edema, hemorrhage, necrosis
- SIRS → sepsis, shock if uncontrolled, with bacteremia from intestinal flora translocation
- Extrapancreatic organ dysfunction - ARDS, pleural effusions, renal failure - Rosen's Emergency Medicine, p. 1265
3. Etiology
Gallstones (40-70%) and alcohol (25-35%) account for ~80% of all cases. 10-20% are idiopathic. - Robbins & Kumar Basic Pathology, p. 641
| Category | Causes |
|---|---|
| Mechanical/Obstructive | Gallstones, pancreas divisum, annular pancreas, post-ERCP, tumors (ampullary, pancreatic carcinoma), trauma |
| Toxic-Metabolic | Alcohol, drugs (azathioprine, thiazides, estrogens, anticonvulsants), hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia |
| Infectious | Viral (mumps, coxsackievirus, HIV, CMV, EBV, varicella), bacterial (TB, Salmonella, Campylobacter, Legionella), parasitic (Ascaris) |
| Genetic | PRSS1 (cationic trypsinogen), SPINK1 (trypsin inhibitor), CFTR mutations |
| Vascular | Vasculitis, atheroembolism, shock/ischemia, polyarteritis nodosa |
| Other | DKA, autoimmune (IgG4-related), hereditary, scorpion venom |
Rosen's Emergency Medicine, p. 1266; Robbins & Kumar, p. 641
4. Pathology
Acute Pancreatitis
Ranges from interstitial edematous (most common, ~90-95%) to necrotizing pancreatitis (~5-10%):
- Edematous: interstitial edema, fat necrosis, minimal parenchymal necrosis
- Necrotizing: widespread hemorrhagic necrosis; in 40-60% of necrotizing cases, debris becomes infected - greatly worsening prognosis
Microscopy (Fig. A below): Fat necrosis (right) alongside focal pancreatic parenchymal necrosis, with neutrophilic infiltrate. Acinar cells are primarily damaged; islets of Langerhans may be destroyed in severe cases.
Gross specimen (Fig. B below): Areas of dark hemorrhage within the pancreatic substance and pale chalky fat necrosis in peripancreatic fat.
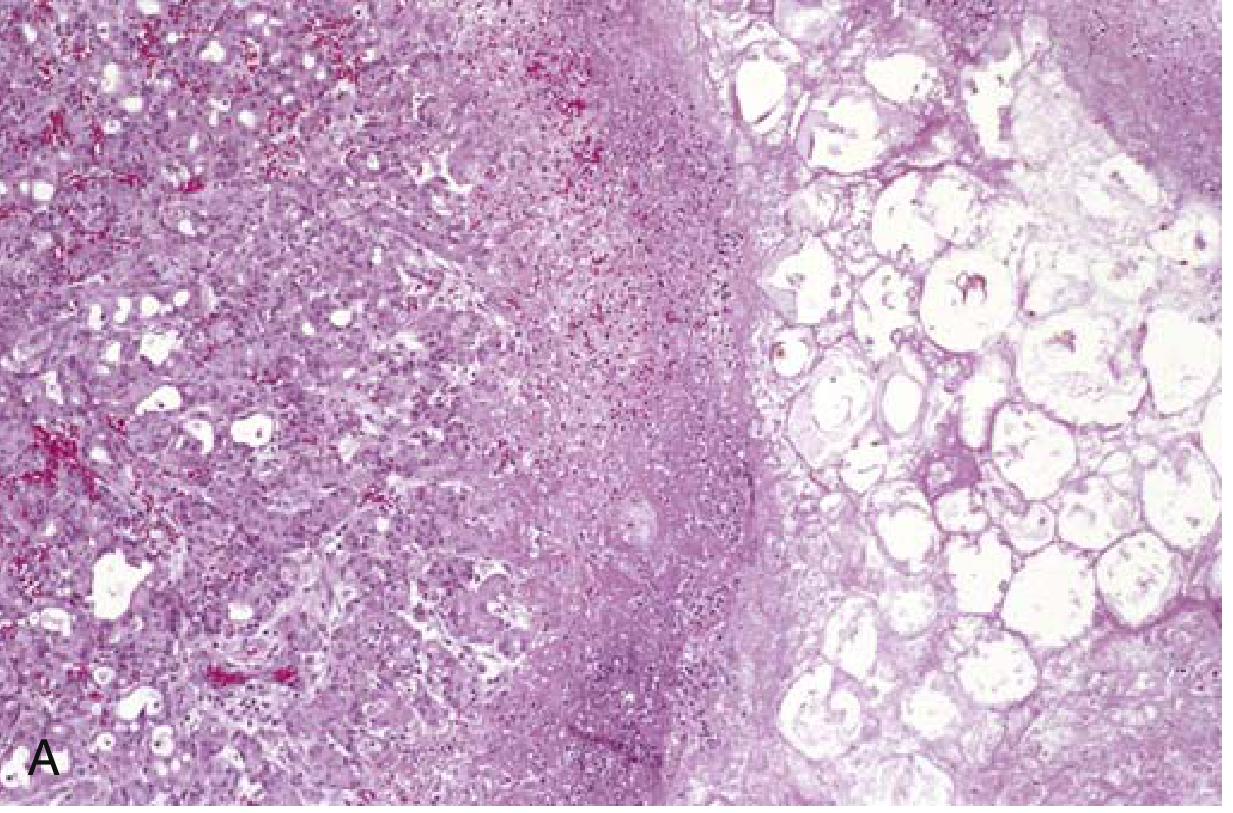
Fig. 15.3A - Microscopic: fat necrosis (right) and focal parenchymal necrosis (center) - Robbins & Kumar

Fig. 15.3B - Gross: hemorrhagic areas (dark) and peripancreatic fat necrosis (pale/yellow patches) - Robbins & Kumar
Chronic Pancreatitis
- Gross: Hard gland, dilated ducts, visible calcific concretions
- Microscopy: Parenchymal fibrosis, loss of acini, variable ductal dilation, chronic inflammatory infiltrate around lobules and ducts; relative sparing of islets of Langerhans initially, but eventual islet destruction leads to diabetes
- Autoimmune pancreatitis (IgG4-related): Dense lymphoplasmacytic infiltrate with IgG4+ plasma cells, "swirling" fibrosis, venulitis (lymphocytic sclerosing pancreatitis) - Robbins & Kumar, p. 644-645
5. Clinical Features
Acute Pancreatitis
- Pain: Persistent epigastric or LUQ pain, radiating to the back/chest/flanks; moderate to severe; intensity does not correlate with severity; may be alleviated by sitting forward
- Associated: Nausea, vomiting, anorexia (oral intake worsens pain)
- Signs:
- Fever, tachycardia, tachypnea (SIRS)
- Hypotension/shock in severe disease
- Epigastric tenderness ± guarding
- Cullen sign (periumbilical bluish discoloration - hemoperitoneum) - rare, poor prognosis
- Grey Turner sign (reddish-brown flank discoloration - retroperitoneal bleed) - rare, poor prognosis
- Jaundice suggests obstruction (gallstone, tumor)
- Diminished/absent bowel sounds with ileus
- Pleural effusions in up to 50% (more often left-sided)
- Systemic complications: ARDS, cardiovascular collapse, renal failure, DIC, coagulopathy, hyperglycemia, hypocalcemia - Rosen's Emergency Medicine, p. 1265-1266
Chronic Pancreatitis
- Recurrent or persistent abdominal and back pain (most common symptom)
- Jaundice from ductal compression
- Weight loss, hypermetabolism, malabsorption
- Exocrine insufficiency (steatorrhea)
- Diabetes mellitus (from eventual islet destruction)
- May be silent until complications develop - Robbins & Kumar, p. 645
6. Diagnosis
Diagnostic Criteria (Atlanta Classification)
Acute pancreatitis requires at least 2 of 3:
- Characteristic abdominal pain
- Serum lipase or amylase >3x upper limit of normal
- Characteristic findings on imaging
Laboratory Tests
| Test | Notes |
|---|---|
| Lipase | More specific and sensitive than amylase; peaks quickly, stays elevated 1-2 weeks; preferred marker |
| Amylase | Less specific (elevated in renal failure, appendicitis, cholecystitis); elevated ~3-5 days; falsely negative in alcohol/hypertriglyceridemia-induced AP |
| ALT | 3x elevated = 95% positive predictive value for gallstone pancreatitis |
| Triglycerides | >1000 mg/dL diagnostic when gallstone/alcohol excluded |
| Calcium | Hypocalcemia = fat necrosis (calcium precipitation); persistent = poor prognosis |
| CBC/BMP | Assess SIRS, organ failure |
| Bilirubin/LFTs | Evaluate obstructive etiology |
Degree of lipase/amylase elevation does NOT correlate with severity. - Rosen's Emergency Medicine, p. 1267
Imaging
- Abdominal US: First-line for biliary etiology (gallstones); limited for direct pancreatic visualization (obscured by bowel gas)
- CT with IV contrast: NOT routine; indicated for: (1) diagnostic uncertainty, (2) ruling out other pathology, (3) assessing complications at 48-72h of non-response - best done at 3-7 days; >90% sensitivity and specificity; pancreatic necrosis = non-enhancing areas; normal in 15-30% of mild cases
- MRI/MRCP: Superior biliary/ductal imaging; useful when contrast is contraindicated
- EUS: Biliary tract assessment, surgical planning
Local Complications (Revised Atlanta 2012)
| Type | Early (<4 wk) | Late (>4 wk) |
|---|---|---|
| Interstitial | Acute peripancreatic fluid collection | Pancreatic pseudocyst (well-defined wall) |
| Necrotizing | Acute necrotic collection (heterogeneous) | Walled-off necrosis |
7. Severity Scoring
Rosen's and Sleisenger & Fordtran emphasize that stratifying patients with severe AP from mild-to-moderate disease is essential to triage:
- Severe AP: persistent multi-organ failure >48 hours, ICU admission, mechanical ventilation
- Scoring systems (Ranson, APACHE-II, BISAP, CT Severity Index/CTSI) are used to predict mortality and guide disposition
8. Management
Acute Pancreatitis - General Principles
1. Fluid Resuscitation
- Aggressive early IV fluid resuscitation is the cornerstone of management
- Recent evidence (2025 meta-analysis, PMID 40085761) favors Lactated Ringer's solution over normal saline for reducing progression to moderate-to-severe AP
2. Analgesia
- Adequate pain control; IV opioids as needed
3. Nutrition
- Previous practice of NPO ("pancreatic rest") has been replaced by early enteral nutrition (EN)
- Severe AP (ICU, SIRS, mechanical ventilation): NG/NJ tube + EN initiated within 24-36 hours of admission
- Mild-moderate AP (ward patient): Oral diet as tolerated; EN only if diet fails to advance after 4 days
- EN vs. PN: Meta-analyses show EN provides 2-fold reduction in infectious complications and 2.5-fold reduction in mortality vs. parenteral nutrition (PN)
- Gastric vs. jejunal feeding: No significant clinical difference in severe AP - Sleisenger & Fordtran, p. 2935-2939
4. Treat the Cause
- Gallstone pancreatitis + cholangitis/obstruction: urgent ERCP
- Hypertriglyceridemia: insulin infusion, plasmapheresis if triglycerides >1000 mg/dL
- Drugs: discontinue offending agent
5. Infected Necrosis
- Antibiotics + drainage (endoscopic, percutaneous, or surgical - "step-up approach")
- Surgery reserved for failed minimally invasive drainage or abdominal compartment syndrome
6. Complications Monitoring
- Watch for ARDS, renal failure, DIC, hyperglycemia, hypocalcemia, splenic/portal vein thrombosis
Chronic Pancreatitis Management
- Alcohol/smoking cessation
- Pancreatic enzyme replacement for exocrine insufficiency
- Pain management: NSAIDs, opioids, antioxidants (selenium, ascorbic acid, beta-carotene, alpha-tocopherol, methionine - evidence mixed)
- Jejunal feeding to improve weight and reduce pain in severe cases
- Endoscopic or surgical decompression for ductal hypertension
- Autoimmune pancreatitis: Steroids ± anti-B cell therapy (responds well)
- Monitor and treat diabetes mellitus
9. Differential Diagnosis
- Peptic ulcer disease / perforated peptic ulcer
- Acute cholecystitis / cholangitis / choledocholithiasis
- Mesenteric ischemia / bowel infarction
- Aortic dissection / abdominal aortic aneurysm
- Myocardial infarction (inferior/posterior)
- Pneumonia, pericarditis
- Sickle cell crisis, DKA
Recent Evidence (2024-2026)
A 2025 systematic review and meta-analysis (PMID 40085761) supports Lactated Ringer's over normal saline for fluid resuscitation in AP, reducing progression to moderate-to-severe disease. The 2026 Ibero-Latin American (iLATAM-AP) guidelines (PMID 42216617) provide updated international consensus on AP management published June 2026, which may contain updates beyond standard textbook recommendations.
Sources: Robbins & Kumar Basic Pathology 10e (pp. 641-645); Rosen's Emergency Medicine 9e (pp. 1265-1270); Sleisenger & Fordtran's GI and Liver Disease (pp. 2935-2943)
This is a shared conversation. Sign in to Orris to start your own chat.