nerve coard cut and reattach susses reatio
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of what happens when a nerve cord is cut (transected) and then reattached (repaired), including the success rates and key factors.
Nerve Transection and Repair: What Happens & Success Rates
1. What Happens When a Nerve is Cut
When a peripheral nerve is severed, two major processes occur:
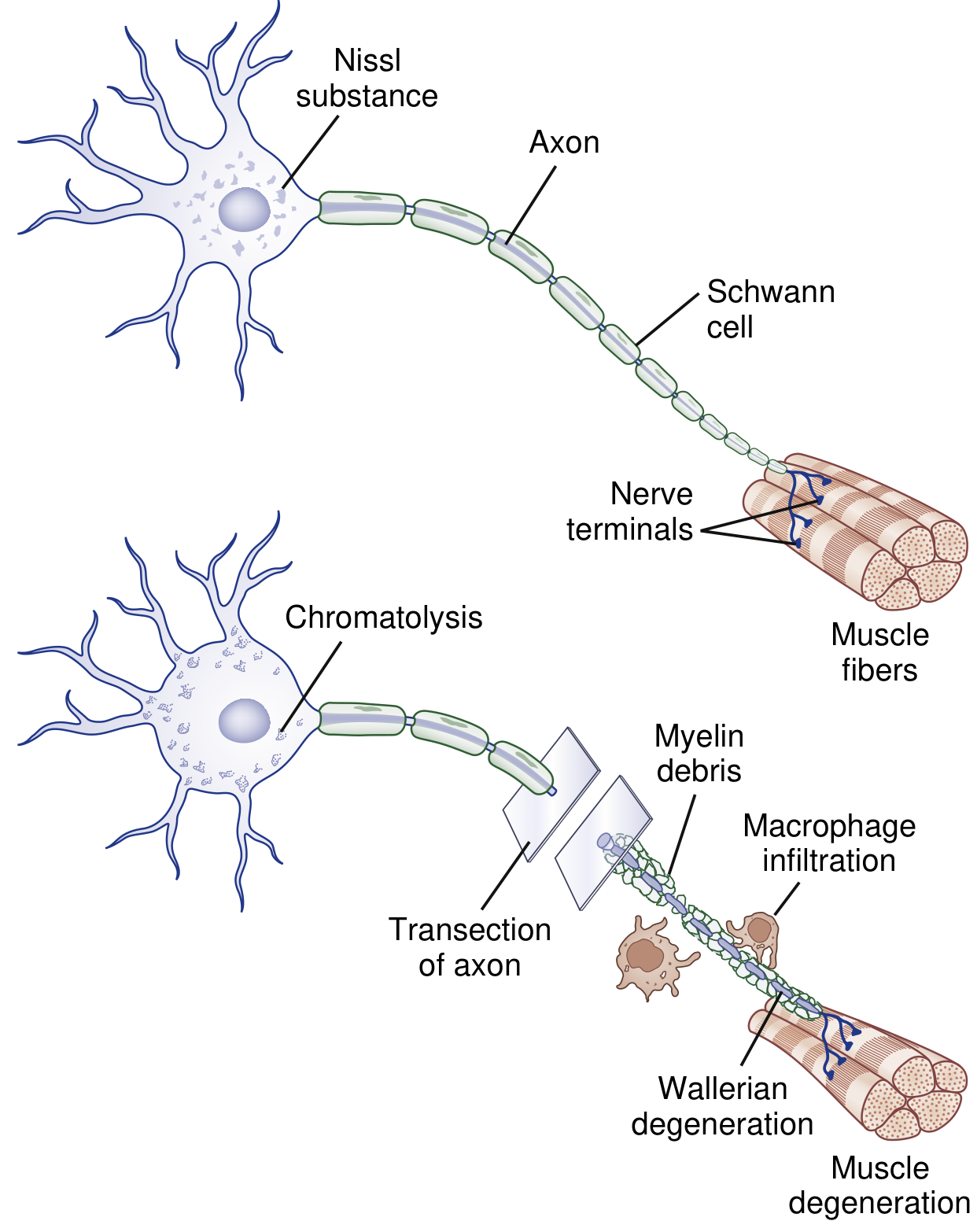
a) Wallerian Degeneration (distal to the cut)
The axon and myelin sheath distal to the transection begin to degenerate within hours to days. Macrophages are recruited to clear the myelin debris and axonal fragments. The Schwann cells dedifferentiate and form aligned tubes called bands of Büngner — these act as a pathway scaffold for regenerating axons. The muscle target loses its nerve supply and begins to atrophy (~30% weight loss in the first month, >60% by 4 months).
b) Proximal Changes & Chromatolysis
The cell body of the neuron undergoes chromatolysis — it switches from a maintenance mode to a regeneration mode. A small segment of Wallerian degeneration also occurs proximal to the cut, back to the nearest node of Ranvier.
2. Regeneration After Repair (Reattachment)
Once the nerve ends are surgically reattached (anastomosed/sutured), regeneration begins:
- Timing: Axon sprouts begin exiting the proximal stump only 2–3 weeks after injury, not immediately.
- Growth rate: Regenerating axons grow at approximately 1 mm/day on average (this can slow distally).
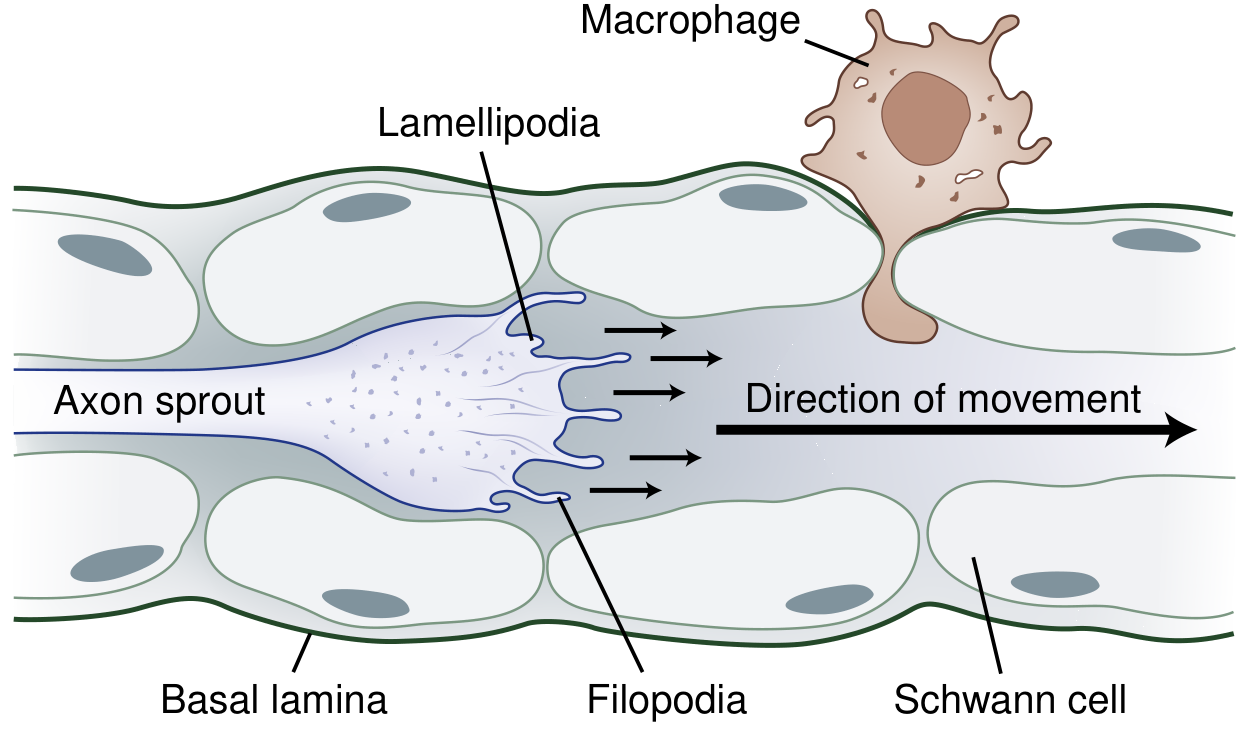
- The growth cone — the motile tip of the regenerating axon — uses lamellipodia and filopodia to navigate, guided by neurotrophic molecules (semaphorins, netrins, ephrins) and the Schwann cell tubes.
3. Success Rate (What Limits Recovery)
Recovery after nerve repair is often incomplete, for several important reasons:
| Barrier | Effect on Recovery |
|---|---|
| The repair site itself | Even a 1–2 mm gap is a significant barrier; ~50% of axons fail to cross and form a neuroma in continuity instead |
| Poor type specificity | Motor axons may enter sensory endoneurial tubes, and vice versa — those axons are functionally lost |
| Poor topographical specificity | Axons may reinnervate the wrong body region (e.g., a thumb nerve ending up in the middle finger) |
| Muscle denervation atrophy | After >12 months of denervation, atrophy becomes difficult to reverse; after 24 months, it is essentially irreversible |
| Delay to repair | Strong experimental evidence shows regeneration quality deteriorates profoundly if repair is delayed beyond 1–2 months |
Key statistic: Only roughly 50% of axons successfully cross the repair site. Of those that do enter the distal nerve, many are misdirected.
4. Timing of Recovery
- Collateral sprouting (from intact fibers): clinical recovery in 3–6 months
- Axonal regeneration (the main mechanism after complete cuts): recovery from 6 to 24 months, depending on how far the nerve must grow to reach its target
- After a brachial plexus injury, for example, it can take 12–18 months for axons to even reach distal muscles
5. Surgical Principles That Improve Outcomes
- Early repair — ideally within weeks; delay beyond 1–2 months worsens outcomes significantly
- Fascicular matching — aligning nerve fascicles rotationally to maximize topographic specificity (critical for reducing misdirection)
- Tension-free anastomosis — a repair under tension leads to scarring and blocks regeneration; if gap is too large, a nerve graft is used to bridge it
- Conduits and grafts — acellular nerve grafts, absorbable conduits, and tubules can bridge gaps and facilitate regeneration when direct end-to-end repair isn't possible
Summary
Nerve cut-and-reattach (primary neurorrhaphy) triggers Wallerian degeneration distally, then slow axonal regeneration from the proximal stump across the repair site. About 50% of axons fail to cross the repair. Those that do may be misdirected. The window for meaningful recovery is roughly 2 years — after which muscle atrophy becomes irreversible. Early surgery, precise fascicular alignment, and tension-free repair are the key determinants of functional success.
— Bradley and Daroff's Neurology in Clinical Practice | Rockwood and Green's Fractures in Adults 10th ed
This is a shared conversation. Sign in to Orris to start your own chat.