Currently used contraceptive name and use
Currently Used Contraceptive Methods: Names and Uses
I. SPACING METHODS (Reversible)
A. Behavioral / Natural Methods
| Method | How It Works / Use |
|---|---|
| Calendar (Rhythm) method | Counts cycle days to predict fertile vs. infertile days; avoids unprotected sex on fertile days (days 10-17 of a 28-day cycle) |
| Symptothermal method | Combines calendar counting with monitoring cervical mucus changes and basal body temperature rise at ovulation |
| Natural Cycles app | FDA-approved mobile app to assist fertility-awareness-based contraception |
| Lactational Amenorrhea Method (LAM) | Exclusive breastfeeding suppresses ovulation; effective for the first 6 months postpartum |
| Withdrawal (Coitus interruptus) | Penis withdrawn before ejaculation; 4% failure with perfect use, ~21% with typical use |
B. Barrier Methods
Physical Barriers
| Method | How It Works / Use |
|---|---|
| Male condom (Nirodh) | Sheath fitted over erect penis before intercourse; prevents sperm from entering vagina; also protects against STIs including HIV |
| Female condom | Polyurethane pouch lining the vagina; internal ring covers cervix, external ring stays outside; prelubricated; effective STI barrier; failure rate 5-21 per 100 women/year |
| Diaphragm (Dutch cap) | Shallow rubber cup (5-10 cm diameter) inserted to cover the cervix before intercourse; must be used with spermicidal jelly; requires fitting by a clinician |
| Cervical cap (FemCap) | Silicone cap that fits directly over the cervix; used with spermicide; works best in women who have never given birth |
Chemical Barriers (Spermicides)
| Method | How It Works / Use |
|---|---|
| Spermicides (nonoxynol-9) | Creams, foams, gels, films, or suppositories inserted vaginally before sex; destroy sperm cell membranes; most effective when combined with a physical barrier |
Combined (Physical + Chemical)
- Diaphragm + spermicide
- Condom + spermicide
C. Intrauterine Devices (IUDs)
Inert IUDs (older, mostly replaced)
- Lippes loop - first widely used plastic IUD
Copper IUDs (2nd generation)
| Name | Details |
|---|---|
| Cu-T 200 / Cu-T 380A / Cu-T 380 Ag | T-shaped device wound with copper wire; effective 5-10+ years; copper ions are spermicidal and alter uterine environment |
| Nova-T | Copper IUD with silver core; good effectiveness |
| Multiload Cu-250 / ML-Cu-375 | Alternative copper designs; number = copper surface area in mm² |
- Can also be used as emergency contraception if inserted within 3-5 days of unprotected intercourse
- Advantages: low expulsion rate, fewer side effects, effective in nulliparous women
Hormonal IUDs (3rd generation)
| Name | Details |
|---|---|
| Mirena (LNG-20 / LNG-IUS) | T-shaped IUD releasing 20 mcg levonorgestrel/day; effective for 10 years; reduces menstrual bleeding; failure rate 0.2 per 100 women-years |
| Progestasert | T-shaped device with 38 mg progesterone; releases 65 mcg/day; needs annual replacement |
| Kyleena, Liletta, Skyla | Lower-dose LNG-releasing IUDs with 3-5 year durations |
D. Hormonal Methods
1. Combined Oral Contraceptive Pills (COCPs)
- Contain estrogen (ethinyl estradiol) + progestin
- Taken daily for 21-24 active days, then 4-7 inactive/placebo days
- Mechanism: Suppress ovulation, thicken cervical mucus, thin endometrium
- Non-contraceptive benefits: Reduce dysmenorrhea, menorrhagia; protect against ovarian cancer (40-60% risk reduction) and endometrial cancer (20-60% reduction)
- Examples: Mala-N, Ovral, Lo-Ovral, Yasmin, Yaz, Seasonique (84-day regimen)
- Contraindications: Women over 35 who smoke, severe hypertension, migraine with aura, history of DVT/PE
2. Progestin-Only Pills (POP / "Mini-pill")
- Taken daily without a break
- Suitable for breastfeeding mothers, women who cannot use estrogen
- Examples: Norethisterone (Micronor), desogestrel (Cerazette)
3. Injectable Contraceptives
| Name | Details |
|---|---|
| DMPA (Depo-Provera) | Medroxyprogesterone acetate 150 mg IM every 3 months; highly effective; may cause menstrual irregularity and delayed return to fertility |
| NET-EN (Noristerat) | Norethisterone enanthate 200 mg IM every 2 months |
| Combined monthly injectable | Estrogen + progestin; given once a month |
4. Subdermal Implants (Long-Acting Reversible)
| Name | Details |
|---|---|
| Nexplanon (Implanon) | Single rod releasing etonogestrel; inserted under skin of upper arm; effective 3 years; highly reliable (failure <0.1%) |
| Jadelle / Norplant-2 | Two rods; 5-year duration; levonorgestrel-releasing |
5. Contraceptive Patch
- Ortho Evra / Xulane: Weekly transdermal patch delivering ethinyl estradiol + norelgestromin; worn for 3 weeks, then 1 week off
- Same mechanism and contraindications as combined OCs
6. Vaginal Ring
- NuvaRing: Monthly flexible ring inserted into vagina; releases ethinyl estradiol + etonogestrel for 3 weeks; removed for 1 week
- Annovera: Yearly ring; worn for 21 days each cycle
E. Emergency Contraception (Post-coital)
| Name | Details |
|---|---|
| Levonorgestrel (Plan B, iPill, Unwanted-72) | 1.5 mg single dose within 72 hours of unprotected sex; delays/inhibits ovulation; does NOT cause abortion |
| Ulipristal acetate (ella) | 30 mg within 120 hours (5 days); selective progesterone receptor modulator; more effective than LNG at 72-120 hrs |
| Combined OC (Yuzpe regimen) | High-dose estrogen + progestin in two doses 12 hours apart within 72 hours |
| Copper IUD | Inserted within 5 days; most effective emergency method (>99%) |
F. Centchroman (Non-hormonal Oral)
- Chhaya (Centchroman / Ormeloxifene): Weekly/biweekly oral pill; selective estrogen receptor modulator; no estrogenic side effects; approved in India; works by preventing implantation
II. TERMINAL METHODS (Permanent Sterilization)
| Method | Details |
|---|---|
| Male sterilization (Vasectomy) | Division/ligation of vas deferens; outpatient procedure; does not affect sexual function; failure rate ~0.1% |
| Female sterilization (Tubectomy / Tubal ligation) | Fallopian tubes cut, tied, or occluded (Pomeroy, Parkland, Filshie clip, Hulka clip methods); laparoscopic or minilaparotomy approach |
| Essure (hysteroscopic occlusion) | Microinserts placed into fallopian tubes via hysteroscope (largely withdrawn from market) |
Summary: Effectiveness Comparison
| Method | Typical Use Failure Rate (%) |
|---|---|
| Implant | <0.1 |
| Sterilization | 0.1-0.5 |
| Hormonal IUD (Mirena) | 0.2 |
| Copper IUD | 0.8 |
| Injectables | 0.3 (perfect), 4 (typical) |
| Combined OCP | 0.3 (perfect), 7-9 (typical) |
| Patch / Ring | ~7 (typical) |
| Male condom | 2 (perfect), 13-18 (typical) |
| Diaphragm + spermicide | 6 (perfect), 12-17 (typical) |
| Spermicide alone | ~18 (typical) |
| Fertility awareness | 1-9 (method-dependent) |
| Withdrawal | 4 (perfect), 18-21 (typical) |
| No method | ~85 |
Prepare flow chart
A clean, professional medical flowchart titled "Contraceptive Methods" showing classification and names. The flowchart starts at the top with "CONTRACEPTIVE METHODS" as the root node, then splits into two main branches: "SPACING METHODS (Reversible)" and "TERMINAL METHODS (Permanent)". Under SPACING METHODS, show 5 sub-branches: 1. "BEHAVIORAL/NATURAL" → Calendar Method, Symptothermal, LAM (Breastfeeding), Withdrawal 2. "BARRIER METHODS" → Physical: Male Condom, Female Condom, Diaphragm, Cervical Cap | Chemical: Spermicides (Nonoxynol-9) | Combined: Condom + Spermicide 3. "INTRAUTERINE DEVICES (IUD)" → Copper IUDs: Cu-T 380A, Nova-T, Multiload | Hormonal IUDs: Mirena (LNG-20), Kyleena, Skyla 4. "HORMONAL METHODS" → Combined OCP (Mala-N, Yasmin), Progestin-Only Pill (Micronor), Injectable (Depo-Provera, NET-EN), Implant (Nexplanon), Patch (Xulane), Vaginal Ring (NuvaRing) 5. "EMERGENCY CONTRACEPTION" → Levonorgestrel (iPill), Ulipristal Acetate (ella), Copper IUD, Centchroman (Chhaya) Under TERMINAL METHODS, show 2 sub-branches: 1. "MALE" → Vasectomy 2. "FEMALE" → Tubectomy / Tubal Ligation Use color coding: blue for the main title, green for spacing methods branch, red for terminal methods branch, light yellow boxes for individual drug/method names. Clean arrows connecting each level. Professional medical textbook style, white background, well-spaced readable text.
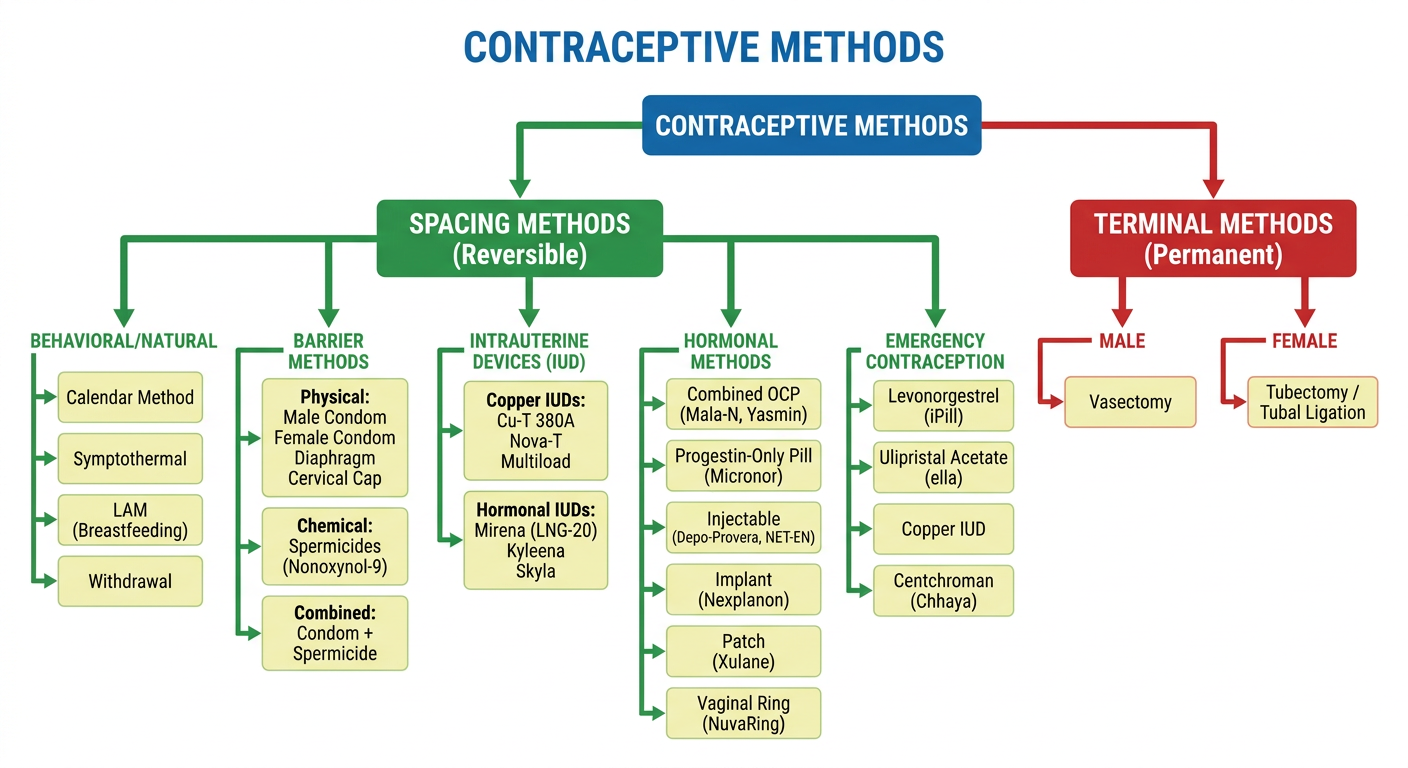
- Spacing Methods (Reversible) - covering Behavioral/Natural methods, Barrier methods, IUDs, Hormonal methods, and Emergency Contraception - with specific drug and device names under each category.
- Terminal Methods (Permanent) - Vasectomy (male) and Tubectomy/Tubal Ligation (female).
Indian population policy
India National Population Policy 2000 objectives targets
https://www.sociologydiscussion.com/population/national-popu…
Indian Population Policy
Historical Background
Timeline of Key Policy Milestones
| Year | Milestone |
|---|---|
| 1952 | World's first National Family Planning Programme launched |
| 1976 | First formal National Population Policy - raised legal marriage age (girls: 15→18; boys: 18→21); included compulsory sterilization provisions (later criticized) |
| 1977 | Policy modified after public backlash; compulsion removed; programme renamed "Family Welfare Programme"; small family norm promoted voluntarily |
| 1983 | National Health Policy adopted; long-term goal set: Net Reproductive Rate (NRR) = 1 by year 2000 (goal not achieved) |
| 2000 | National Population Policy (NPP) 2000 - the landmark comprehensive policy |
| 2019 | National Health Policy 2017 and vision documents updated population stabilization targets |
National Population Policy (NPP) 2000 - The Core Policy
Definition
Philosophy
- Reaffirms commitment to a target-free approach in administering family planning services
- Gives informed choice to people to voluntarily avail reproductive health care services
- Goes beyond fertility/mortality rates - addresses women's education, empowerment, child survival, adolescent health, and under-served populations
Objectives of NPP 2000
1. Immediate Objective
2. Medium-Term Objective
3. Long-Term Objective
National Socio-Demographic Goals (to be achieved by 2010)
| # | Goal |
|---|---|
| 1 | Address unmet needs for reproductive and child health services, supplies, and infrastructure |
| 2 | Make school education up to age 14 free and compulsory; reduce school dropouts to below 20% for both boys and girls |
| 3 | Reduce Infant Mortality Rate (IMR) to below 30 per 1000 live births |
| 4 | Reduce Maternal Mortality Ratio (MMR) to below 100 per 1,00,000 live births |
| 5 | Achieve universal immunization of children against all vaccine-preventable diseases |
| 6 | Promote delayed marriage for girls - not earlier than 18 years, preferably after 20 years |
| 7 | Achieve 80% institutional deliveries and 100% deliveries by trained persons |
| 8 | Achieve universal access to information, counselling, and services for fertility regulation with a wide basket of contraceptive choices |
| 9 | Achieve 100% registration of births, deaths, marriages, and pregnancies |
| 10 | Contain the spread of AIDS; promote integration between RTI/STI management and NACO |
| 11 | Prevent and control communicable diseases |
| 12 | Integrate Indian Systems of Medicine (ISM/AYUSH) in reproductive and child health services |
| 13 | (Promote male participation in planned parenthood) |
| 14 | Bring about convergence in implementation of related social sector programmes so family welfare becomes a people-centred programme |
Key Features of NPP 2000
Scope - Broader than Previous Policies
- Women's education and empowerment
- Child survival and health
- Adolescent health and education (including adolescent reproductive health)
- Increased male participation in planned parenthood
- Focus on under-served groups: urban slums, tribal communities, hill areas, displaced and migrant populations
- Collaboration with NGOs
Approach - Target-Free
- Moved away from sterilization targets
- Focus on individual choice ("cafeteria approach" - offering all methods from which an individual can choose)
- Community-based delivery at panchayat and nagar palika levels
Organisational Structure for Implementation
National Commission on Population (chaired by PM)
|
State Commissions on Population (chaired by Chief Ministers)
|
District/Block level committees
|
Panchayat / Nagar Palika level implementation
Population Projections and Outcomes
| Projection | Figure |
|---|---|
| Technical Group projection for 2010 (without NPP) | 1162 million |
| Projected population for 2010 (with full NPP implementation) | 1107 million |
| Actual Census 2011 population | 1210 million |
- 28% unmet need for contraception services
- Inadequate health infrastructure
- Poor coverage and outreach at village level
Family Welfare Programme Under NPP
- Barrier methods (condoms, diaphragm)
- Oral contraceptive pills (Mala-N, Chhaya)
- Intrauterine devices (Cu-T, Mirena)
- Injectable (Depo-Provera)
- Terminal methods (vasectomy, tubectomy)
- Emergency contraception
Current Status and Updates
- India's TFR reached 2.0 (below replacement level) as per NFHS-5 (2019-21) - a major milestone
- Several states (Kerala, Tamil Nadu, Andhra Pradesh) achieved replacement-level TFR decades ago
- Focus has now shifted from population control to quality of reproductive health services, adolescent health, and addressing high-fertility states (UP, Bihar, MP, Rajasthan)
- The Mission Parivar Vikas (2016) targets 146 high-fertility districts in 7 states