Management of allergic rhinitis?
Reading File
Finding Sources
Searching PubMed
"allergic rhinitis"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"allergic rhinitis" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Management of Allergic Rhinitis
Allergic rhinitis (AR) is the sixth most common chronic illness in the US, affecting 10-20% of adults. Management rests on three pillars: allergen avoidance, pharmacotherapy, and immunotherapy. Treatment is stratified by symptom frequency (intermittent vs. persistent) and severity (mild vs. moderate-severe), following the ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines.
ARIA Classification
| Intermittent | Persistent | |
|---|---|---|
| Definition | <4 days/week OR <4 weeks | ≥4 days/week AND ≥4 weeks |
| Mild | No sleep/daily activity impairment | |
| Moderate-Severe | Sleep disturbed, activities impaired |
Management Algorithm (ARIA)
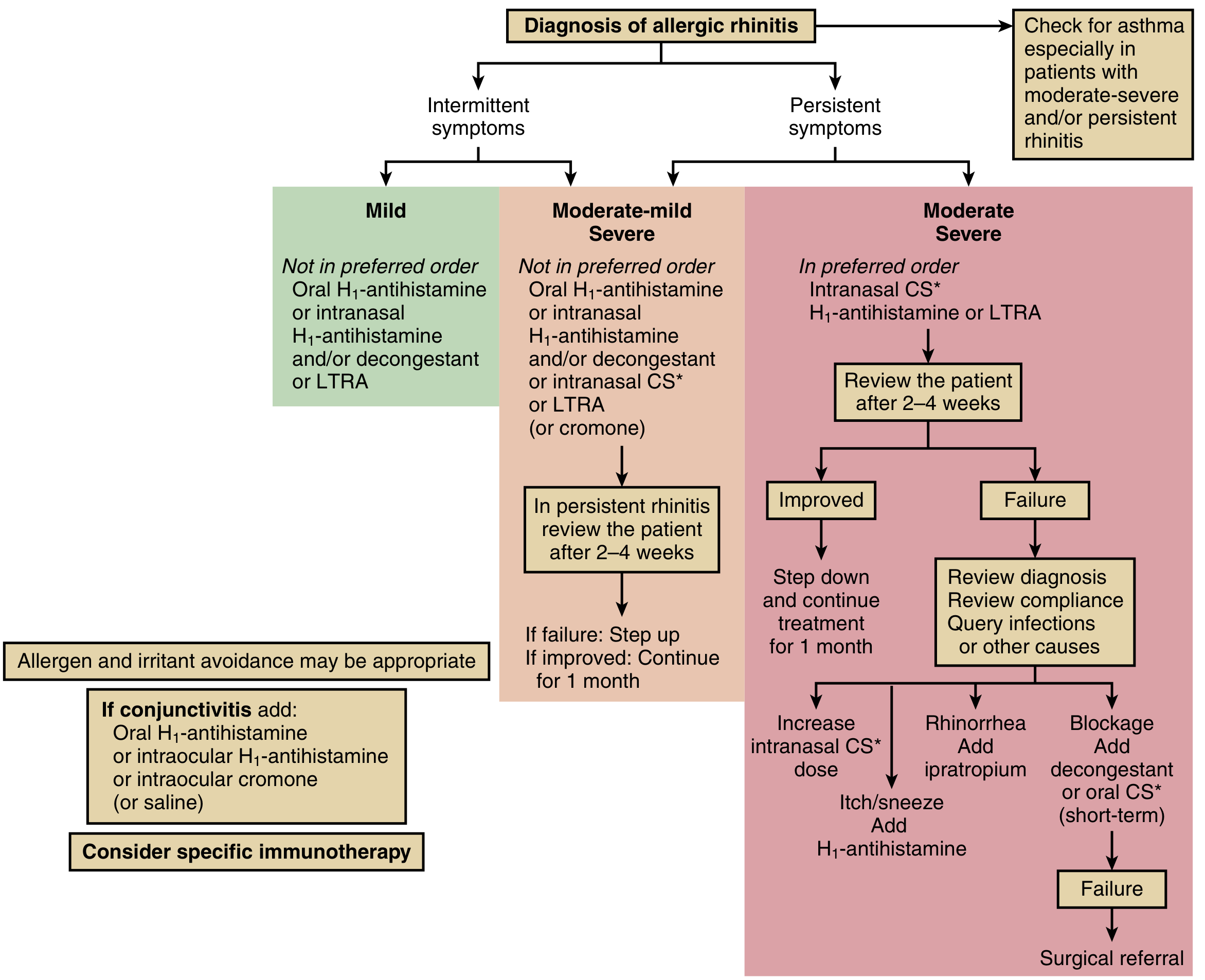
(From Murray & Nadel's Textbook of Respiratory Medicine, adapted from Bousquet et al., ARIA 2012)
1. Allergen Avoidance
- Identify triggers via skin prick testing or serum allergen-specific IgE (ImmunoCAP)
- Common seasonal triggers: tree and grass pollens
- Common perennial triggers: house dust mites, pet dander, mold
- Environmental measures (mattress covers, HEPA filters, pet removal) reduce allergen load
- Saline nasal irrigation provides modest symptomatic benefit and may reduce medication need
2. Pharmacotherapy
A. Intranasal Corticosteroids (INCs) - First-line for moderate-severe / persistent AR
Examples: Fluticasone, mometasone, budesonide, triamcinolone, ciclesonide
- Most effective monotherapy for all four cardinal symptoms, especially nasal congestion
- Require consistent daily use - no effect when used as-needed; maximal benefit over days to weeks
- Administration technique: clear nasal mucus first, tilt head slightly forward, direct spray laterally (away from septum) to reduce epistaxis risk
- Adverse effects: Local irritation, sneezing, epistaxis. At high cumulative doses (especially with concurrent inhaled steroids): reduced growth velocity in children, adrenal suppression - growth monitoring recommended
- A 2025 network meta-analysis (PMID: 39548801) confirmed INCs have superior efficacy compared to oral treatments for nasal symptoms
B. Oral H1-Antihistamines - First-line for mild/episodic AR
2nd-generation (preferred): Cetirizine, levocetirizine, fexofenadine, loratadine, desloratadine
1st-generation: Diphenhydramine, chlorpheniramine (avoid for regular use)
- Target rhinorrhea, sneezing, and itching - do NOT relieve nasal congestion
- 2nd-generation agents: once-daily dosing (12-24 h duration), minimal CNS penetration, no significant sedation
- 1st-generation agents: avoid in patients requiring alertness; anticholinergic side effects (dry mouth, urinary retention, blurred vision)
- Metabolized by hepatic CYP450 (except cetirizine/levocetirizine - excreted unchanged in urine; fexofenadine - in feces)
C. Intranasal Antihistamines
Examples: Azelastine, olopatadine
- Faster onset of action than INCs - useful for acute breakthrough symptoms
- Adverse effects: Bitter taste, systemic absorption with potential for sedation
D. Intranasal Combination (INC + Intranasal Antihistamine)
Example: Azelastine/fluticasone (Dymista)
- For moderate-severe AR: superior rapidity and magnitude of relief compared to either agent alone
- A 2024 systematic review (PMID: 38685482) found combined intranasal antihistamines + corticosteroids have additive benefit over monotherapy
E. Decongestants
Oral: Pseudoephedrine, phenylephrine
Intranasal: Oxymetazoline, xylometazoline
- Relieve nasal congestion rapidly
- Intranasal decongestants: Limit to <3-5 days to avoid rhinitis medicamentosa (rebound congestion)
- Oral decongestants: Avoid in hypertension, cardiovascular disease, hyperthyroidism, glaucoma, BPH
F. Leukotriene Receptor Antagonists (LTRAs)
Example: Montelukast
- Consider when other therapies are ineffective or not tolerated; more effective in combination with antihistamines
- Important: FDA black box warning for serious neuropsychiatric events (depression, suicidal ideation) - reserve for patients where benefits outweigh risks
G. Ipratropium Nasal Spray
- Add-on for predominant rhinorrhea when INCs alone are insufficient
- Also useful in vasomotor (non-allergic) rhinitis
H. Cromones (Cromolyn Sodium)
- Mast cell stabilizer; safe profile but less efficacious than INCs
- Requires frequent dosing (3-4x/day)
- Useful in pregnancy or where steroid exposure is to be minimized
I. Ocular Symptoms (Allergic Conjunctivitis)
- Topical H1-antihistamines (ketotifen, olopatadine, azelastine) or mast cell stabilizers (cromolyn, lodoxamide)
- Oral antihistamines also help
- Avoid topical steroids unless directed by an ophthalmologist
3. Immunotherapy - Disease-Modifying Treatment
Immunotherapy is the only treatment that modifies the natural history of AR and can prevent progression to asthma.
Subcutaneous Immunotherapy (SCIT)
- Weekly subcutaneous injections with gradually escalating antigen doses; total course 2-3 years
- Most well-studied approach in the US
- Risk: Rare anaphylaxis (must be administered in a clinical setting with emergency equipment)
Sublingual Immunotherapy (SLIT)
- FDA-approved products for timothy grass (Grastek), five grass pollens (Oralair), dust mites (Odactra), and short ragweed (Ragwitek)
- Can be self-administered at home; avoids injections
- Higher rate of mild local mucosal side effects; systemic reactions rarer than SCIT
- SCIT and SLIT have similar overall efficacy; head-to-head trials are limited
Indications for Immunotherapy
- Symptoms inadequately controlled with pharmacotherapy and avoidance
- Patient desiring disease modification rather than just symptom suppression
- Not recommended: Poorly controlled asthma, poor medication adherence
- Not well-studied in children under 5 years
- May reduce risk of new-onset asthma in AR patients
4. Step-Up/Step-Down Strategy
| Response at 2-4 weeks | Action |
|---|---|
| Improved | Step down, continue for 1 month |
| Failure | Review diagnosis, check compliance, exclude infection |
| Persistent congestion | Increase INC dose; add short-term oral/decongestant |
| Persistent rhinorrhea | Add ipratropium |
| Persistent itch/sneeze | Add H1-antihistamine |
| Refractory to all | Surgical referral (e.g., turbinate reduction) |
5. Special Considerations
- AR and asthma: 80% of patients with allergic asthma also have AR. Screen persistent/moderate-severe AR patients for asthma. INCs benefit both conditions (unified airway)
- Pregnancy: Prefer intranasal cromolyn or loratadine (category B); avoid decongestants especially in first trimester
- Children: Prefer 2nd-generation oral antihistamines or intranasal steroids; monitor growth with long-term INC use; immunotherapy not well-studied under age 5
- Montelukast: Use with caution given neuropsychiatric warning; not preferred first-line
Recent Evidence (2024-2025)
- [PMID 38685482] (J Allergy Clin Immunol 2024): Intranasal antihistamines + corticosteroids are superior to either alone - supporting combined intranasal therapy for moderate-severe AR
- [PMID 39251016] (J Allergy Clin Immunol Pract 2024): Intranasal treatments outperform oral treatments for nasal symptom control
- [PMID 39548801] (Allergy 2025): Network meta-analysis confirms INC monotherapy as most efficacious intranasal option; combination INC+antihistamine provides additional benefit
Sources: Murray & Nadel's Textbook of Respiratory Medicine, pp. 1610-1611; Harriet Lane Handbook 23e, p. 523; Lippincott Illustrated Reviews Pharmacology, p. 1314
This is a shared conversation. Sign in to Orris to start your own chat.