Angle closure glaucoma
Reading File
Finding Sources
Searching PubMed
"angle closure glaucoma"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from Kanski's Clinical Ophthalmology, Goldman-Cecil Medicine, and Tintinalli's Emergency Medicine. Let me compile a thorough, well-structured answer.
Angle Closure Glaucoma
Definition & Overview
Angle closure glaucoma refers to obstruction of the trabecular meshwork by the peripheral iris (iridotrabecular contact — ITC), blocking aqueous outflow and raising intraocular pressure (IOP). It can be:
- Primary — occurs in anatomically predisposed eyes
- Secondary — caused by another ocular or systemic factor
Primary angle-closure glaucoma (PACG) accounts for up to half of all glaucoma cases globally and is disproportionately common in Asia. It progresses more rapidly and causes more visual loss than primary open-angle glaucoma (POAG). — Kanski's Clinical Ophthalmology, 10e
Classification (Spectrum)
| Stage | Definition |
|---|---|
| Primary angle-closure suspect (PACS) | Occludable angle on gonioscopy, no ITC, no raised IOP, no optic nerve damage |
| Primary angle closure (PAC) | ITC in ≥3 quadrants ± raised IOP, but no glaucomatous optic neuropathy |
| Primary angle-closure glaucoma (PACG) | ITC + raised IOP + glaucomatous optic neuropathy |
| Acute primary angle closure (APAC) | Sudden complete closure causing acute crisis |
Pathophysiology
The dominant mechanism is relative pupillary block:
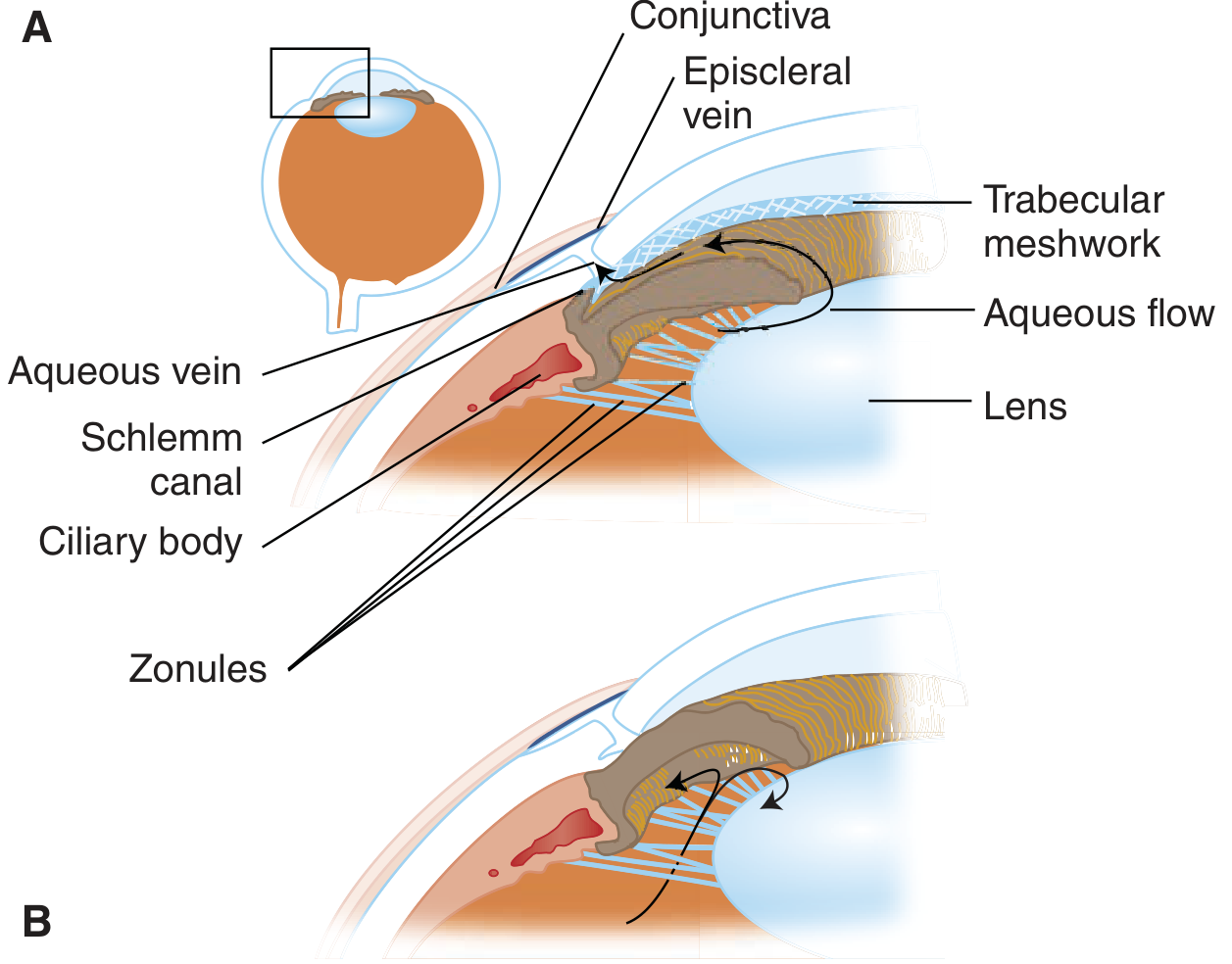
Normal aqueous flow (A) vs angle closure with pupillary block and iris bombé (B) — Tintinalli's Emergency Medicine
- Aqueous is produced by the ciliary body and normally flows from the posterior chamber → through the pupil → into the anterior chamber → exits via the trabecular meshwork into Schlemm's canal.
- When the posterior iris surface contacts the anterior lens surface, a pressure differential builds between the posterior and anterior chambers.
- This bows the peripheral iris forward (iris bombé), narrowing and eventually closing the trabecular meshwork angle.
- IOP rises rapidly — from a normal 10–20 mmHg to 50–80+ mmHg.
- When IOP exceeds the corneal pump's capacity, corneal epithelial oedema develops → blurred vision and halos.
The mid-dilated pupil state is the most dangerous: the iris is thickest peripherally while still partially covering the lens, maximising pupillary block. Dilation to a widely dilated or miotic state actually reduces risk.
Additional mechanisms (especially in Asians):
- Plateau iris configuration — anteriorly rotated ciliary processes hold the peripheral iris in a forward position; not relieved by iridotomy alone
- Phacomorphic closure — swollen or anteriorly subluxated lens
Risk Factors
| Factor | Detail |
|---|---|
| Hypermetropia (farsightedness) | Short axial length, shallow anterior chamber, narrow angle; up to 1 in 6 hyperopes ≥1 D are PACS |
| Age | Lens thickens with age, pushing iris forward |
| Female sex | More commonly affected than males |
| Asian ethnicity | Far Eastern and Indian Asians particularly at risk |
| Family history | Genetic factors, increased prevalence in first-degree relatives |
| Short axial length / nanophthalmos | Axial length <20 mm = very high risk |
| Cataracts | Increase lens vault |
Precipitating Factors for Acute Attack
- Pharmacological mydriasis (atropine, antihistamines, TCAs, cold/flu remedies, motion sickness patches)
- Sympathomimetics (epinephrine, pseudoephedrine, intranasal cocaine)
- Nebulized bronchodilators (albuterol + ipratropium) in ICU patients
- Topiramate and other sulfa derivatives (cause ciliary body effusion)
- Dim illumination / watching TV in a dark room
- Semi-prone position (e.g. reading)
- Acute emotional stress
Clinical Features
Symptoms
- Acute: sudden severe periocular/orbital pain, markedly decreased vision, nausea and vomiting (may simulate acute abdomen), headache
- Subacute/intermittent: blurring ("smoke-filled room") and haloes around lights from transient corneal oedema
Signs
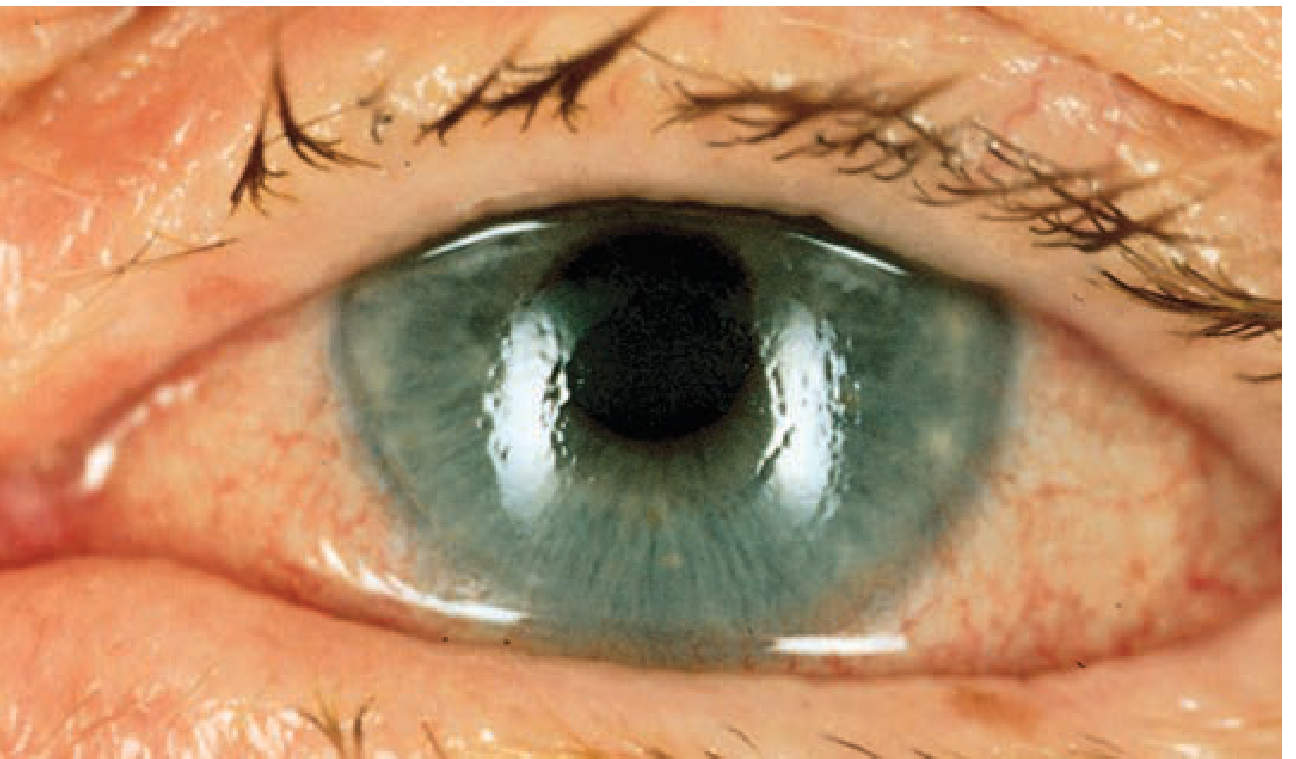
Acute angle closure: corneal cloudiness with circumcorneal injection — Tintinalli's Emergency Medicine
- Visual acuity typically 6/60 to hand movements
- IOP 50–80 mmHg (rock-hard globe)
- Hazy/steamy cornea (corneal epithelial oedema)
- Circumcorneal (ciliary) injection with violaceous hue
- Fixed, mid-dilated, vertically oval pupil — classic and pathognomonic
- Shallow anterior chamber with aqueous flare
- Fellow eye typically shows an occludable angle
After Resolution (Resolved APAC)
- Early: folds in Descemet's membrane, low IOP (ciliary body shutdown)
- Late: glaukomflecken (white foci of anterior lens necrosis), iris atrophy with spiral pattern, posterior synechiae, irregular pupil
Diagnosis
Gonioscopy is the definitive tool — it directly visualises the angle and grades closure. Key systems:
| Grade | Angle width | Structures visible |
|---|---|---|
| 4 (35–45°) | Wide open | Ciliary body visible |
| 3 (25–35°) | Open | Scleral spur visible |
| 2 (20°) | Narrow | Trabeculum visible, no scleral spur |
| 1 (10°) | Very narrow | Schwalbe line ± top of trabeculum |
| 0 | Closed | Iridocorneal contact |
Van Herick slit-lamp method screens angle width by comparing peripheral anterior chamber depth to corneal thickness — a ratio <1/4 warrants urgent gonioscopy.
Additional investigations: UBM (ultrasound biomicroscopy) to diagnose plateau iris; AS-OCT (anterior segment OCT) for angle imaging.
Differential Diagnosis of Acute IOP Elevation
- Acute APAC
- Lens-induced angle closure (swollen/subluxated lens)
- Malignant glaucoma (aqueous misdirection) — especially post-operatively
- Secondary angle closure (neovascular, inflammatory)
- Hypertensive uveitis / herpetic trabeculitis / Posner-Schlossman syndrome
- Scleritis with angle involvement
Treatment
Immediate (Acute Attack)
Position: Lay patient supine — gravity shifts the lens posteriorly, reducing pupillary block.
Medical IOP reduction (combine multiple agents):
| Agent Class | Drug & Dose |
|---|---|
| Carbonic anhydrase inhibitor | Acetazolamide 500 mg IV or PO, then 250 mg q4h (max 1 g/day); or topical dorzolamide/brinzolamide |
| Topical β-blocker | Timolol 0.5% — 1 drop to affected eye |
| Topical α₂-agonist | Apraclonidine 1% or brimonidine 0.2% — 1 drop |
| Hyperosmotic agent (if no IOP response at 1 hour) | IV mannitol 1.5–2 g/kg over 30 min; or oral glycerine |
⚠️ Pilocarpine is no longer recommended acutely — at very high IOP, the ischaemic iris sphincter is unresponsive; cholinergic agents can paradoxically shallow the anterior chamber and worsen closure. — Tintinalli's, 10e
Analgesia/antiemetics: Fentanyl is preferred (lowers IOP); ondansetron is safe (no IOP effect). Vomiting increases IOP and should be controlled.
Definitive Treatment
Peripheral laser iridotomy (PI) — creates a full-thickness hole in the peripheral iris to equalize anterior and posterior chamber pressures, bypassing the pupillary block. Performed once the cornea is clear and IOP is controlled.
- Bilateral PI is standard (the fellow eye has an occludable angle)
- Does not help plateau iris — laser peripheral iridoplasty or lens extraction needed in those cases
Clear lens extraction / phacoemulsification with IOL — the EAGLE trial demonstrated that early lens extraction is more effective and cost-effective than laser PI for PAC and PACG with elevated IOP. Achieves IOP control in ~80% preoperatively elevated eyes and corrects hypermetropia.
Trabeculectomy (with mitomycin C) — reserved for persistent IOP elevation despite an open angle, though carries a risk of malignant glaucoma.
Prophylaxis for PACS
The ZAP trial showed laser PI has only a small protective benefit over 6 years; selective prophylactic PI is appropriate for higher-risk patients (symptoms of intermittent closure, need for frequent dilation, atropine-like medications, limited access to eye care).
Summary Flowchart
Acute red eye + severe pain + fixed mid-dilated pupil + cloudy cornea
↓
Measure IOP (≥40–50 mmHg) → APAC
↓
Supine position + Acetazolamide + Timolol + Apraclonidine
↓
If IOP not ↓ in 1 hr → IV Mannitol
↓
Urgent ophthalmology consult → Peripheral laser iridotomy
↓
Prophylactic PI to fellow eye
Key references: Kanski's Clinical Ophthalmology: A Systematic Approach, 10e | Tintinalli's Emergency Medicine, 10e | Goldman-Cecil Medicine, 26e
POAG
Finding Sources
Searching PubMed
"open-angle glaucoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive material from three authoritative sources. Let me compile the full answer.
Primary Open-Angle Glaucoma (POAG)
Definition
POAG is a chronic, progressive optic neuropathy of adult onset characterised by:
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve damage
- Characteristic visual field (VF) loss as damage progresses
- Open anterior chamber angle on gonioscopy (distinguishing it from angle-closure)
- Absence of secondary causes
IOP is the only proven modifiable risk factor, though POAG can occur at normal IOP (normal-tension glaucoma). — Kanski's Clinical Ophthalmology, 10e
Epidemiology
- The most prevalent glaucoma type in European and African populations
- Prevalence >70 years: ~6% in White, ~16% in Black, ~3% in Asian populations
- Affects both genders equally
- Responsible for the second leading cause of blindness worldwide
Risk Factors
| Factor | Key Points |
|---|---|
| Elevated IOP | Higher IOP → greater likelihood; asymmetry ≥4 mmHg is significant |
| Age | Risk rises with advancing age |
| Black race | ~4× more common, earlier onset, harder to control |
| Family history | Siblings: ~4× normal risk; offspring: ~2× |
| Myopia | Associated with increased POAG incidence and greater susceptibility |
| Large optic disc | Larger discs more vulnerable to damage |
| Low ocular perfusion pressure | Difference between arterial BP and IOP |
| Translaminar pressure gradient | IOP–CSF pressure differential deforms lamina cribrosa |
| Calcium-channel blockers | Meta-analysis shows higher POAG prevalence with monotherapy use |
| Anti-VEGF therapy | Repeated intravitreal injections (especially bevacizumab) can cause sustained IOP rise |
Diabetes mellitus is often cited clinically but longitudinal studies show no independent increased risk — an association seen in clinic-based studies reflects selection bias.
Genetics
POAG has been associated with ≥127 genomic loci (Nature Communications, 2021). Key causative mutations:
- MYOC gene → myocilin protein (expressed in trabecular meshwork)
- OPTN gene → optineurin
Pathophysiology
Aqueous outflow resistance at the trabecular meshwork is elevated, raising IOP. This elevated IOP (and/or vascular insufficiency to the optic nerve head) causes progressive retinal ganglion cell axon death at the lamina cribrosa. Loss follows the arcuate nerve fibre bundle distribution, causing the characteristic pattern of VF loss.
Normal IOP range: 10–21 mmHg. However, ~40–50% of POAG patients have IOP ≤21 mmHg at any single screening (normal-tension glaucoma subtype).
Clinical Features
Symptoms
- Usually asymptomatic until late — the insidious, painless onset is the hallmark
- Peripheral field loss goes unnoticed until advanced
- Late symptoms: difficulty reading, loss of contrast sensitivity, glare
- Central vision and acuity are preserved until end-stage
Optic Disc Signs
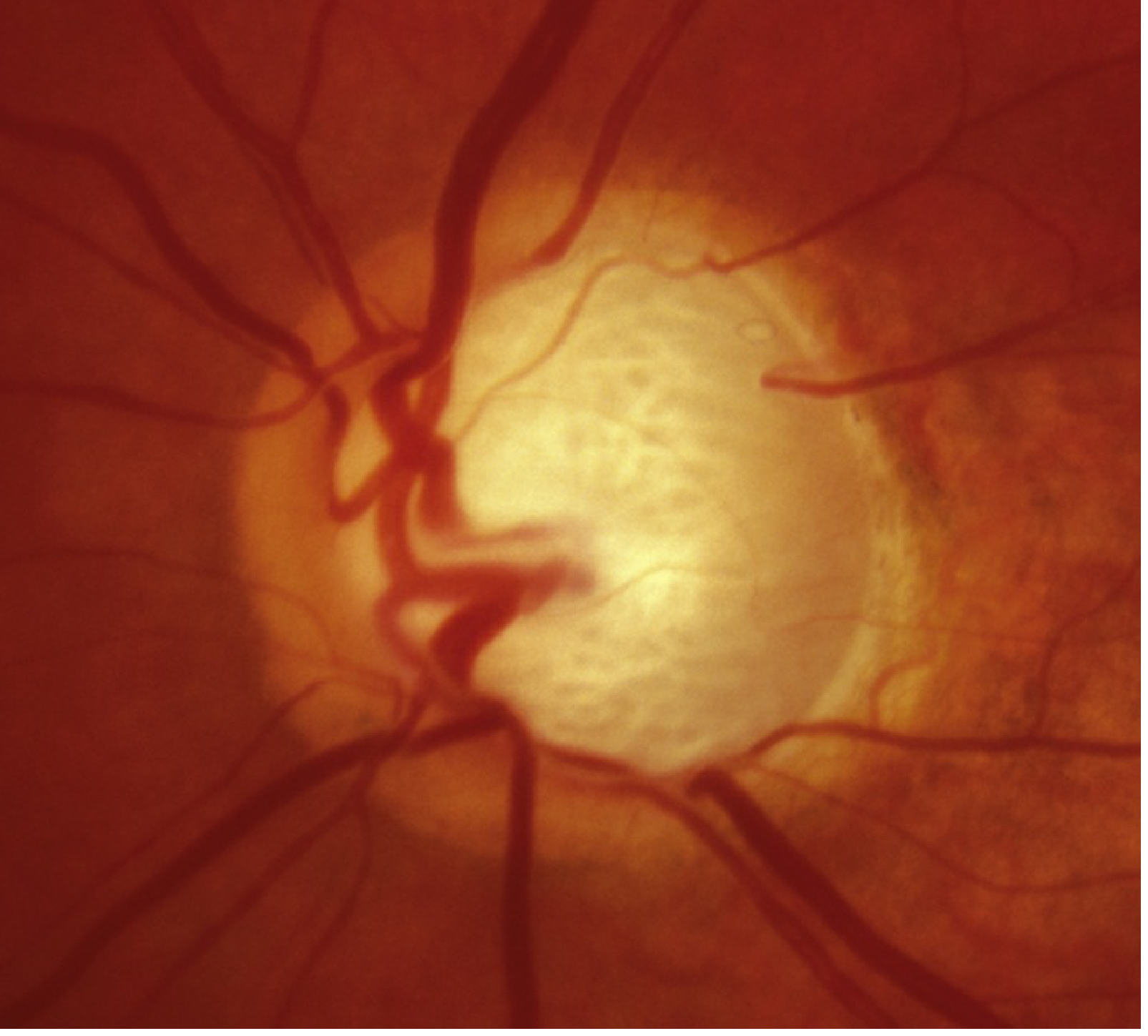
Advanced POAG: near-total cupping with remnant neuroretinal rim only — Wills Eye Manual
Key disc findings:
- Increased cup-to-disc (C:D) ratio — concentric enlargement of the cup; C:D >0.6 or asymmetry >0.2 is suspicious
- Neuroretinal rim notching — most common inferiorly (ISNT rule: normal rim is thickest Inferior > Superior > Nasal > Temporal)
- RNFL defects — wedge-shaped defects in the peripapillary NFL
- Disc haemorrhages (Drance haemorrhages) — small splinter bleeds at the disc margin; a marker of active progression
- Bayonetting / nasal displacement of vessels — vessels appear to dive into the disc and re-emerge
Disc Damage Likelihood Scale (DDLS) grades severity by the narrowest neuroretinal rim width (rim/disc ratio) from stage 1 (0.4+, at risk) through stage 10 (0, glaucoma disability).
Gonioscopy
- Open angle — no peripheral anterior synechiae (PAS); this is the key finding distinguishing POAG from PACG
Visual Field Defects
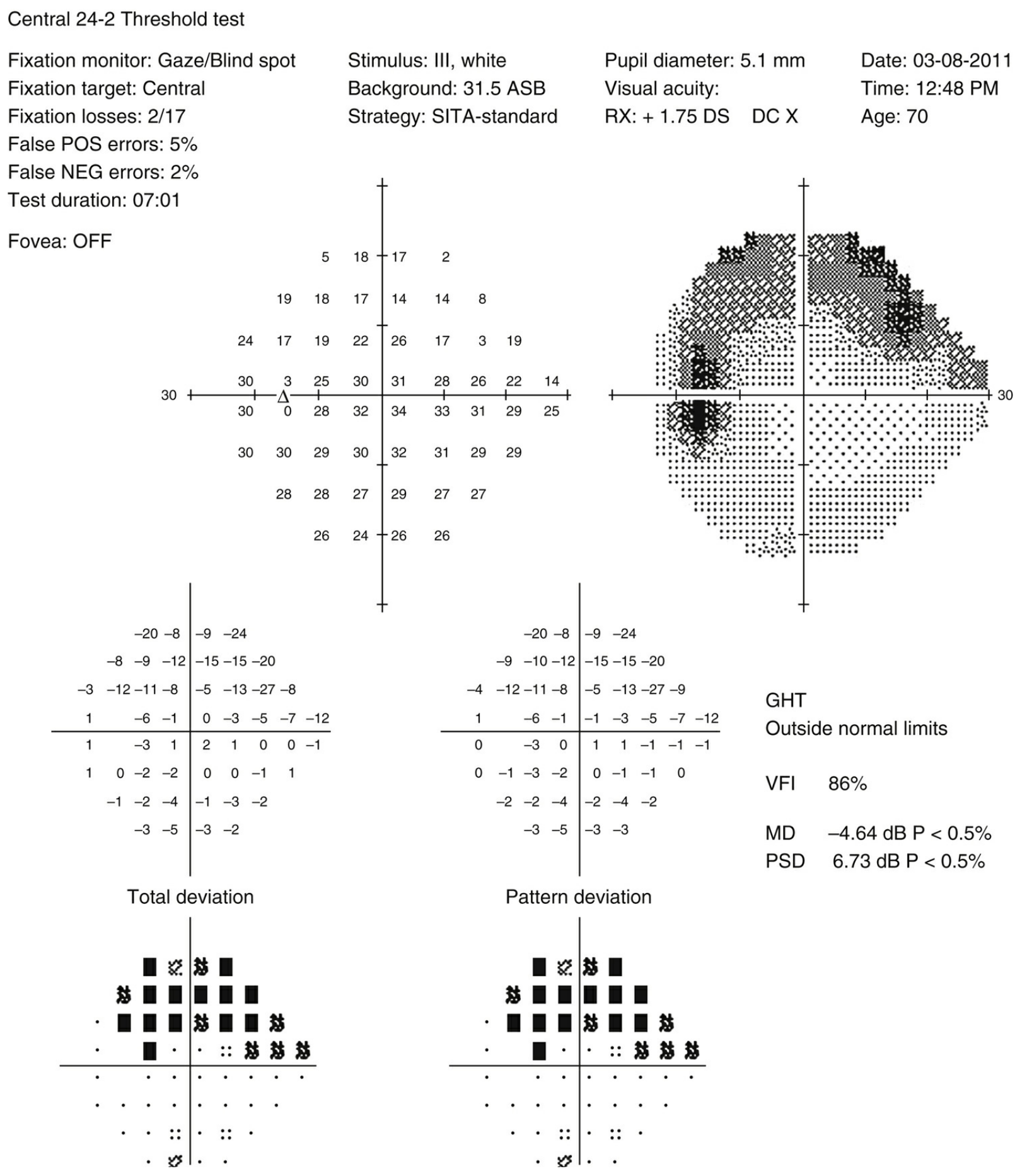
Humphrey 24-2 automated perimetry: superior arcuate defect with MD −4.64 dB, PSD 6.73 dB — Wills Eye Manual
VF loss follows the arcuate nerve fibre bundle pattern:
| Stage | Defect |
|---|---|
| Early | Paracentral scotomas (10–20° of fixation), nasal step, temporal wedge |
| Moderate | Arcuate scotomas (Bjerrum scotoma) — arc from blind spot around fixation |
| Advanced | Ring scotoma (superior + inferior arcuates join) |
| End-stage | Small central island ± temporal island |
HVF staging by Mean Deviation (MD):
- Early: MD > −6 dB
- Moderate: −6 to −12 dB
- Severe: < −12 dB
Minimal criteria for glaucoma (Hodapp-Parrish-Anderson):
- Glaucoma Hemifield Test (GHT) outside normal limits on ≥2 consecutive tests, OR
- Cluster of ≥3 non-edge points depressed at P<5%, with at least 1 at P<1%, on ≥2 tests, OR
- Corrected PSD (pattern standard deviation) <5% of normal on ≥2 consecutive fields
Investigations
| Test | Purpose |
|---|---|
| Automated perimetry (HVF 24-2/30-2) | Detect and monitor VF defects |
| OCT RNFL | Detect early RNFL thinning before VF loss; monitor progression |
| Gonioscopy | Confirm open angle; rule out secondary causes |
| Corneal pachymetry | CCT affects IOP measurement accuracy; thin corneas underestimate true IOP |
| Diurnal IOP curve | Captures IOP fluctuation throughout the day |
| Disc photos | Baseline and serial comparison |
Atypical features warranting further workup: optic pallor > cupping, VF defects respecting the vertical midline or hemianopic, decreased VA/colour vision disproportionate to cupping → consider neurological cause; MRI brain/orbits with gadolinium.
Treatment
Goal
Reduce IOP to a target level that halts or slows optic nerve damage. IOP reduction of ≥30% from baseline is generally the target. Treatment is lifelong.
Step 1 — Medical Therapy (First-Line)
Prostaglandin analogues — preferred first-line (once daily, most efficacious, ~25–35% IOP reduction):
| Drug | Dose |
|---|---|
| Latanoprost 0.005% | Once nightly |
| Bimatoprost 0.01–0.03% | Once nightly |
| Travoprost 0.004% | Once nightly |
| Tafluprost 0.0015% | Once nightly (preservative-free) |
Side effects: iris/periorbital hyperpigmentation (irreversible in hazel/gray irides), hypertrichosis of lashes. Caution in active uveitis, CME, pregnancy.
Beta-blockers (~20–25% IOP reduction):
- Timolol 0.25–0.5%, levobunolol — once or twice daily
- Avoid in: asthma, COPD, heart block, bradyarrhythmia, CHF, depression, myasthenia gravis
- Systemic effects: bronchospasm, bradycardia, hypotension, reduced libido, CNS depression
Alpha-2 agonists:
- Brimonidine 0.1–0.2% — b.i.d. to t.i.d.
- Contraindicated with MAOIs (hypertensive crisis); avoid in children <5 (CNS/cardiorespiratory depression)
- Apraclonidine 0.5–1%: short-term only (tachyphylaxis, high allergy rate)
Topical carbonic anhydrase inhibitors:
- Dorzolamide 2% or brinzolamide 1% — b.i.d. to t.i.d.
- Systemic CAIs (acetazolamide, methazolamide) reserved for refractory/urgent cases; monitor electrolytes; rare aplastic anaemia, Stevens-Johnson syndrome
Rho-kinase inhibitors (ROCK inhibitors):
- Netarsudil 0.02% — once daily; newer class; increases trabecular outflow
Pilocarpine: not routinely used due to side effects (headache, miosis, increased uveitis/RD risk, possible angle closure with miosis).
Punctal occlusion after instillation (10 sec) or lid closure (1–2 min) reduces systemic absorption.
Step 2 — Laser Trabeculoplasty
Can be used as first-line or when medications are insufficient, poorly tolerated, or compliance is a concern.
| Type | Detail |
|---|---|
| Selective Laser Trabeculoplasty (SLT) | Preferred; low energy, less tissue damage, repeatable; equivalent IOP reduction to ALT |
| Argon Laser Trabeculoplasty (ALT) | Initial success 70–80%, drops to ~50% at 2–5 years; not repeatable |
SLT targets pigmented trabecular meshwork cells without thermal damage. Particularly effective in patients with heavy TM pigmentation.
Step 3 — Surgery
Indicated for advanced disease, rapid progression, or IOP uncontrolled by medication/laser.
| Procedure | Notes |
|---|---|
| Trabeculectomy | Creates a fistula from anterior chamber to episcleral space (filtering bleb); adjunctive MMC/5-FU improves efficacy but increases bleb leak/hypotony risk |
| Tube-shunt (glaucoma drainage device) | Baerveldt, Ahmed — synthetic tube diverts aqueous to equatorial reservoir |
| MIGS (Minimally Invasive Glaucoma Surgery) | Shorter recovery, fewer complications; for mild-moderate disease. Includes: trabecular micro-bypass (iStent), canaloplasty, subconjunctival microstents (XEN gel stent), deep sclerectomy, trabectome |
| Laser cyclophotocoagulation | Diode or endolaser; reduces aqueous production; reserved for refractory/end-stage |
Follow-Up
- After starting new medication: review in 4–8 weeks
- If satisfactory response: reassess every 3–6 months
- If inadequate response: switch or add a second agent (wait 5 min between drops to prevent washout)
- Progressive disease despite good IOP: consider poor adherence; assess drop technique
- Serial optic disc photos + OCT RNFL + HVF at every significant visit
Normal-Tension Glaucoma (NTG)
A subtype of POAG where IOP is consistently ≤21 mmHg. Vascular insufficiency to the optic nerve head is implicated. Associated with vasospasm (migraine, Raynaud's), nocturnal hypotension, and cardiovascular risk. IOP reduction still slows progression (CNTGS trial: 30% reduction target). Disc haemorrhages are more common. Rule out neurological causes carefully (MRI essential if VF defects respect the vertical midline).
Comparison: POAG vs Angle-Closure Glaucoma
| Feature | POAG | ACG (Acute) |
|---|---|---|
| Onset | Insidious | Sudden |
| Pain | None | Severe |
| IOP elevation | Gradual | Abrupt, very high |
| Angle | Open | Closed |
| Cornea | Clear | Hazy/oedematous |
| Pupil | Normal | Fixed, mid-dilated |
| Prevalence | Europeans/Africans | Asians/hyperopes |
Key references: Kanski's Clinical Ophthalmology: A Systematic Approach, 10e | Wills Eye Manual, 8e | Goldman-Cecil Medicine, 26e
ONH evaluation various techniques
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content on all ONH evaluation techniques. Let me compile the full answer.
Optic Nerve Head (ONH) Evaluation — Techniques
Overview
The ONH (optic disc) is the anatomical gateway for retinal ganglion cell (RGC) axons exiting the eye. Its evaluation is central to glaucoma diagnosis and monitoring. The approach spans clinical examination, photography, and objective imaging technologies. Imaging supplements but does not replace clinical examination and visual field testing. — Kanski's Clinical Ophthalmology, 10e
1. Clinical Examination
Direct & Indirect Ophthalmoscopy
The simplest method — estimates the cup-to-disc ratio and gross disc appearance. Direct ophthalmoscopy provides a monocular, magnified (~15×) view but lacks stereopsis. Indirect (binocular indirect ophthalmoscope) gives a wider, stereoscopic view but is less magnified. Neither is adequate for detailed disc documentation.
Slit-Lamp Biomicroscopy with Fundus Lens
The clinical gold standard for disc examination. A slit lamp combined with a hand-held fundus lens (60D, 78D, 90D, or Goldmann 3-mirror) provides stereoscopic, high-magnification views.
Correction factors for vertical disc diameter measurement:
| Lens | Correction factor |
|---|---|
| Volk 60D | ×0.88–1.0 |
| Volk 78D | ×1.1 |
| Volk 90D | ×1.3 |
| Goldmann 3-mirror | ×1.27 |
A narrow slit beam is focused on the disc; beam height is adjusted to match the superior-to-inferior NRR span, then read from the slit lamp graticule.
2. Normal ONH Parameters
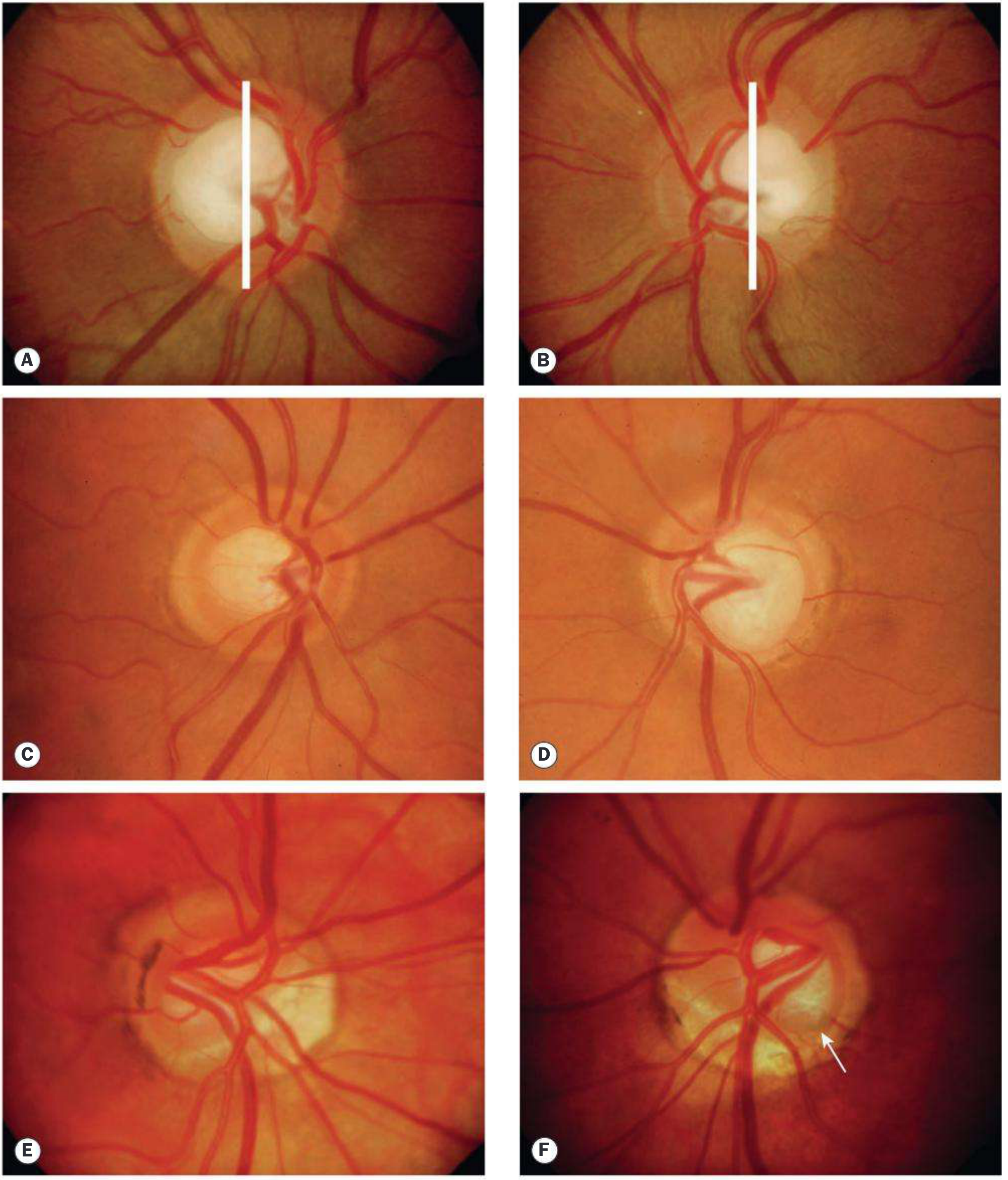
Optic disc asymmetry examples — Kanski's Clinical Ophthalmology
Cup-to-Disc (C:D) Ratio
- Vertical C:D is used (more sensitive than horizontal)
- C:D >0.7 in only 2% of the normal population
- Inter-eye asymmetry ≥0.2 in ~5% of normals but ~25% of glaucoma patients
- Key principle: large discs have large physiological cups — a C:D of 0.8 in a large disc may be normal; any cup in a small disc may be abnormal
Neuroretinal Rim (NRR) — The ISNT Rule
Normal rim tissue is thickest in the order: Inferior > Superior > Nasal > Temporal
- Sensitivity for glaucoma: 81%; specificity: 32% (not specific — many normal eyes violate ISNT)
- Glaucoma characteristically causes rim notching first inferiorly, then superiorly
Optic Disc Size
- Normal median vertical diameter: 1.5–1.7 mm (White populations)
- Largest mean disc size in persons of African descent
- Large discs are more vulnerable to glaucomatous damage (thinner lamina cribrosa, especially in NTG)
Disc Hemorrhages (Drance Hemorrhages)
- Small, splinter-shaped hemorrhages at the disc margin, usually inferotemporal
- Marker of active RNFL loss and glaucoma progression
- More common in NTG than POAG
3. Optic Disc Photography
Stereo Disc Photography
- Historically the reference standard for disc imaging and documentation
- Images acquired by slightly repositioning the camera between shots (manually or with a stereo separator)
- Allows direct serial comparison at follow-up
- Limitation: subjective interpretation, no automated quantification
Fundus Camera (2D)
- Non-stereoscopic single photographs; widely used for screening and baseline documentation
- Colour photographs document NRR colour, pallor, haemorrhages, peripapillary atrophy (PPA)
4. Optical Coherence Tomography (OCT)
OCT is now the dominant imaging modality for ONH and RNFL evaluation. It uses near-infrared light interference to generate cross-sectional images of retinal tissue with axial resolution of ~5–7 μm.
OCT RNFL Analysis
- A circular scan (3.46 mm diameter) is placed around the optic disc
- RNFL thickness is measured in microns at each clock position
- Displayed as a TSNIT plot (Temporal–Superior–Nasal–Inferior–Temporal) with a double-hump pattern in normal eyes
- Compared to a normative age-matched database; results colour-coded:
- Green = within normal limits (p>5%)
- Yellow = borderline (p<5%)
- Red = below normal limits (p<1%)
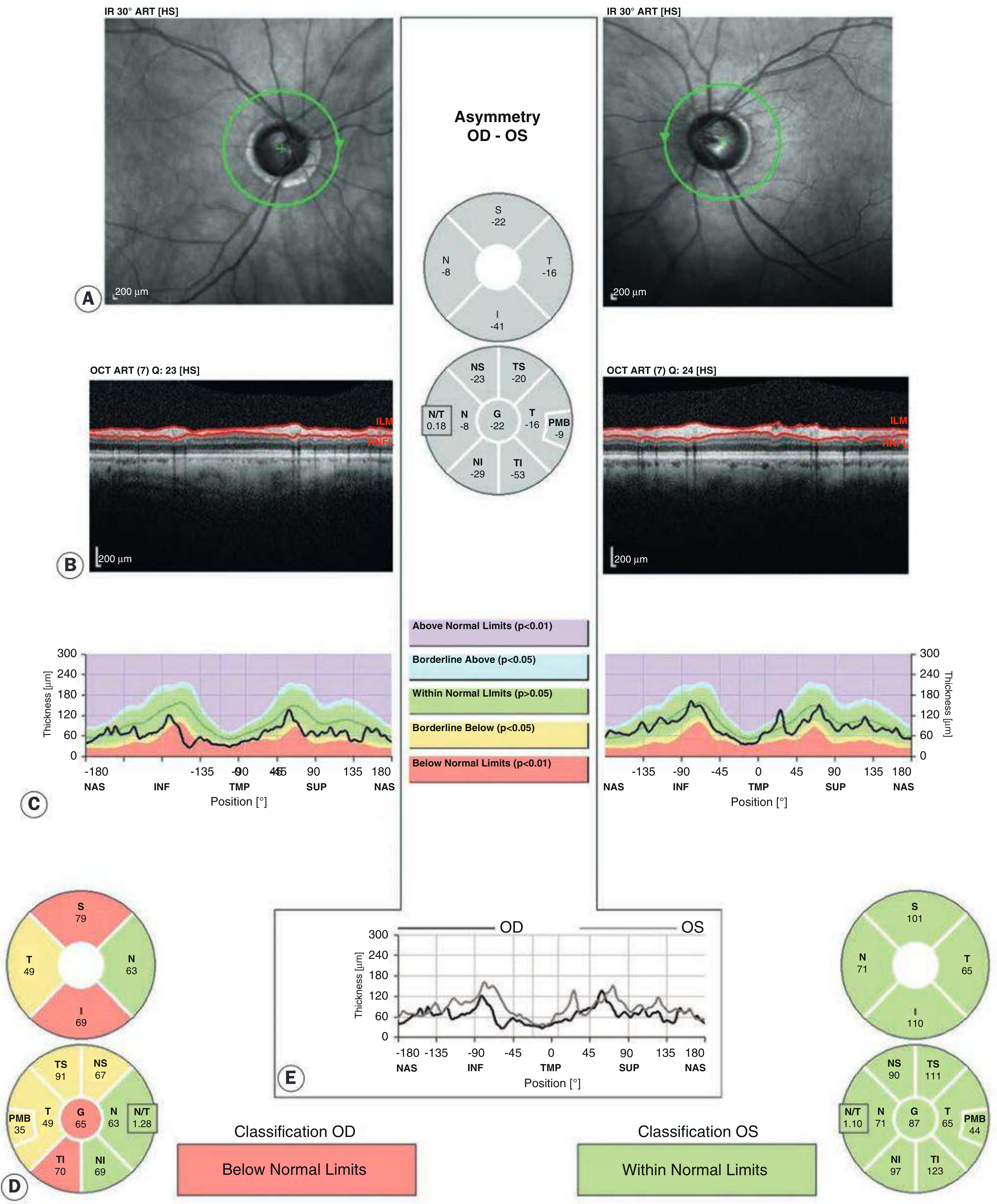
Heidelberg Spectralis OCT: RNFL asymmetry — OD classified "Below Normal Limits" with inferior and superior thinning — Kanski's Clinical Ophthalmology
OCT Optic Disc Analysis (Neuroretinal Rim)
- Measures rim area, disc area, C:D ratio, and rim width objectively
- BMO-MRW (Bruch's Membrane Opening — Minimum Rim Width): newer, more accurate parameter; measures the shortest distance from the BMO edge to the inner limiting membrane
OCT Ganglion Cell Complex (GCC) / Macular OCT
- Measures ganglion cell layer (GCL) + inner plexiform layer (IPL) thickness in the macular region
- Detects early glaucomatous damage — especially useful when the disc appearance is ambiguous or the optic disc is large/small
- Perifoveal GCL thinning corresponds to early superior/inferior arcuate VF defects
Serial OCT for Progression
- Event-based analysis: flags significant change from baseline
- Trend-based analysis: calculates rate of RNFL thinning (μm/year)
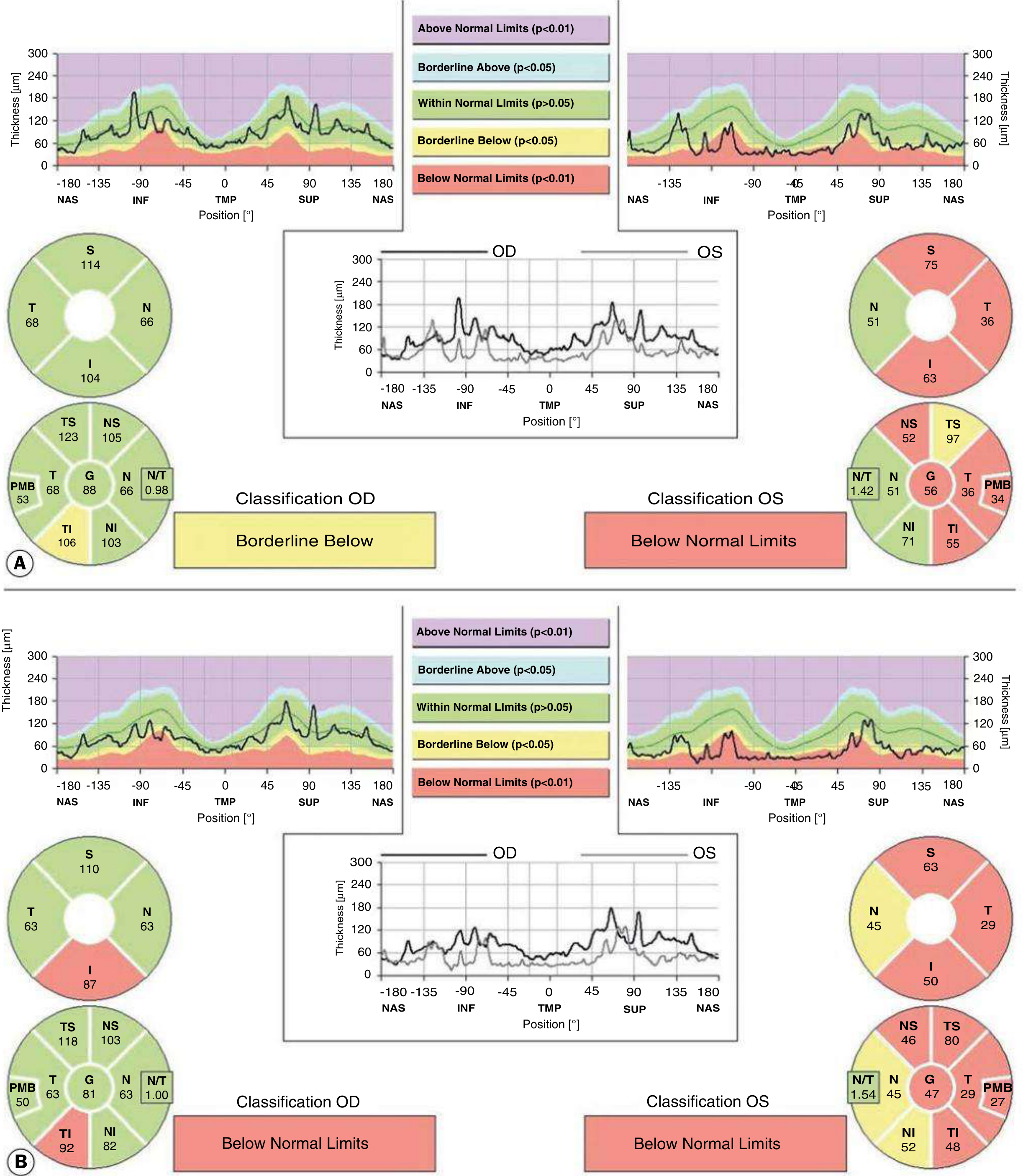
Progressive RNFL thinning documented on serial OCT — Kanski's Clinical Ophthalmology
Key principle: RNFL thinning on OCT precedes both optic disc changes and visual field loss on standard automated perimetry. OCT can detect structural damage years before functional loss becomes measurable.
5. Heidelberg Retinal Tomograph (HRT) — Confocal Scanning Laser Ophthalmoscopy (cSLO)
- Uses a confocal laser (670 nm diode) to acquire a series of images at different focal depths, building a 3D topographic map of the ONH surface
- Key parameters: rim area, cup area, cup volume, rim volume, mean RNFL thickness, cup shape measure
- Moorfields Regression Analysis (MRA): compares rim area to disc area against a normative database for each of 6 sectors — classified as within normal limits, borderline, or outside normal limits
- Glaucoma Probability Score (GPS): alternative analysis without requiring a manual disc margin contour
- Serial exams enable topographic change analysis (TCA) — automatically identifies areas of significant surface depression
Advantages: No dilation required; established long-term progression databases; reproducible
Limitations: Requires manual disc margin delineation (operator-dependent); less sensitive than OCT in detecting early RNFL change; limited by media opacity
Limitations: Requires manual disc margin delineation (operator-dependent); less sensitive than OCT in detecting early RNFL change; limited by media opacity
6. Scanning Laser Polarimetry (GDx)
- Uses polarized laser light to measure birefringence of RNFL — the parallel arrangement of microtubules in RGC axons retards polarized light in proportion to NFL thickness
- Output: TSNIT average, superior average, inferior average, Nerve Fiber Indicator (NFI) (0–100; NFI >30 = glaucoma likely)
- Variable Corneal Compensation (VCC) and Enhanced Corneal Compensation (ECC) correct for corneal birefringence artefacts
Limitations: Atypical birefringence patterns (in some patients) can cause false-positive results ("atypical scan pattern"); largely superseded by spectral-domain OCT in modern practice
7. Anterior Segment OCT (AS-OCT)
- Evaluates the filtration angle structure non-invasively
- Measures Angle Opening Distance (AOD500) — distance between the iris and trabecular meshwork at 500 μm from the scleral spur
- Measures Trabecular-Iris Surface Area (TISA) — cross-sectional area of the angle recess
- Particularly useful for angle-closure assessment, screening, and post-iridotomy evaluation
- Limitation: cannot image structures behind the iris (ciliary body, lens zonules)
8. Ultrasound Biomicroscopy (UBM)
- High-frequency ultrasound (35–50 MHz) providing up to 25 μm axial / 50 μm lateral resolution
- Unique ability to visualise structures posterior to the iris — ciliary body, posterior chamber, lens zonules, ciliary processes
- Essential for diagnosing:
- Plateau iris configuration
- Ciliary body cysts/tumours
- Malignant glaucoma (aqueous misdirection — showing forward rotation of the ciliary body)
- Angle recession
- Requires immersion in saline or coupling gel; patient must be supine
Compared to AS-OCT:
| Feature | AS-OCT | UBM |
|---|---|---|
| Behind iris | ✗ | ✓ |
| Angle imaging | ✓ | ✓ |
| Non-contact | ✓ | ✗ (immersion) |
| Resolution | ~15–18 μm | ~25 μm axial |
9. Pattern ERG (pERG)
- Measures electrical activity of macular retinal ganglion cells in response to a pattern-reversal stimulus
- Waveform components: N35 (35 ms negative), P50 (50 ms positive), N95 (95 ms negative) — N95 is reduced in glaucoma (reflects RGC dysfunction)
- Objective, non-invasive measure that can detect functional RGC loss before structural changes on OCT in some cases
- Not a substitute for clinical examination or imaging; useful for monitoring subtle optic neuropathy
10. Corneal Pachymetry
- Measures central corneal thickness (CCT)
- Not an ONH technique per se, but essential for interpreting IOP — applanation tonometry (Goldmann) assumes a CCT of ~540 μm
- Thin corneas (e.g. <520 μm): IOP underestimated → true IOP is higher
- Thick corneas (e.g. >600 μm): IOP overestimated → true IOP is lower
- CCT is also an independent risk factor for glaucoma progression (thinner CCT = higher risk), beyond just its effect on IOP measurement
Summary Comparison Table
| Technique | What it measures | Key strength | Key limitation |
|---|---|---|---|
| Slit-lamp biomicroscopy | NRR, C:D, disc size | Stereoscopic, clinical gold standard | Subjective, no quantification |
| Stereo disc photography | Disc morphology | Serial comparison, permanent record | No quantification |
| OCT RNFL / BMO-MRW | RNFL thickness, rim width, GCL | Earliest structural detection; objective; progressive monitoring | Signal quality affected by media opacity, myopia |
| HRT (cSLO) | Disc surface topography, rim area | 3D map, established progression databases | Requires contour line; superseded by OCT for RNFL |
| GDx (SLP) | RNFL birefringence (thickness) | Non-dilated; NFI score | Atypical birefringence artefact; largely replaced by OCT |
| AS-OCT | Angle width, iris-trabecular anatomy | Non-contact angle imaging | Cannot see behind iris |
| UBM | Posterior iris structures, ciliary body | Only method to see behind iris | Contact/immersion; operator-dependent |
| Pattern ERG | Macular RGC function | Objective functional measure | Not for routine use; requires specialist lab |
| Pachymetry | Corneal thickness | IOP correction, risk stratification | Indirect measure only |
Key references: Kanski's Clinical Ophthalmology: A Systematic Approach, 10e | Wills Eye Manual, 8e
This is a shared conversation. Sign in to Orris to start your own chat.