Prehepa tic jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough account of prehepatic jaundice, drawn from multiple authoritative medical textbooks.
Prehepatic Jaundice
Overview
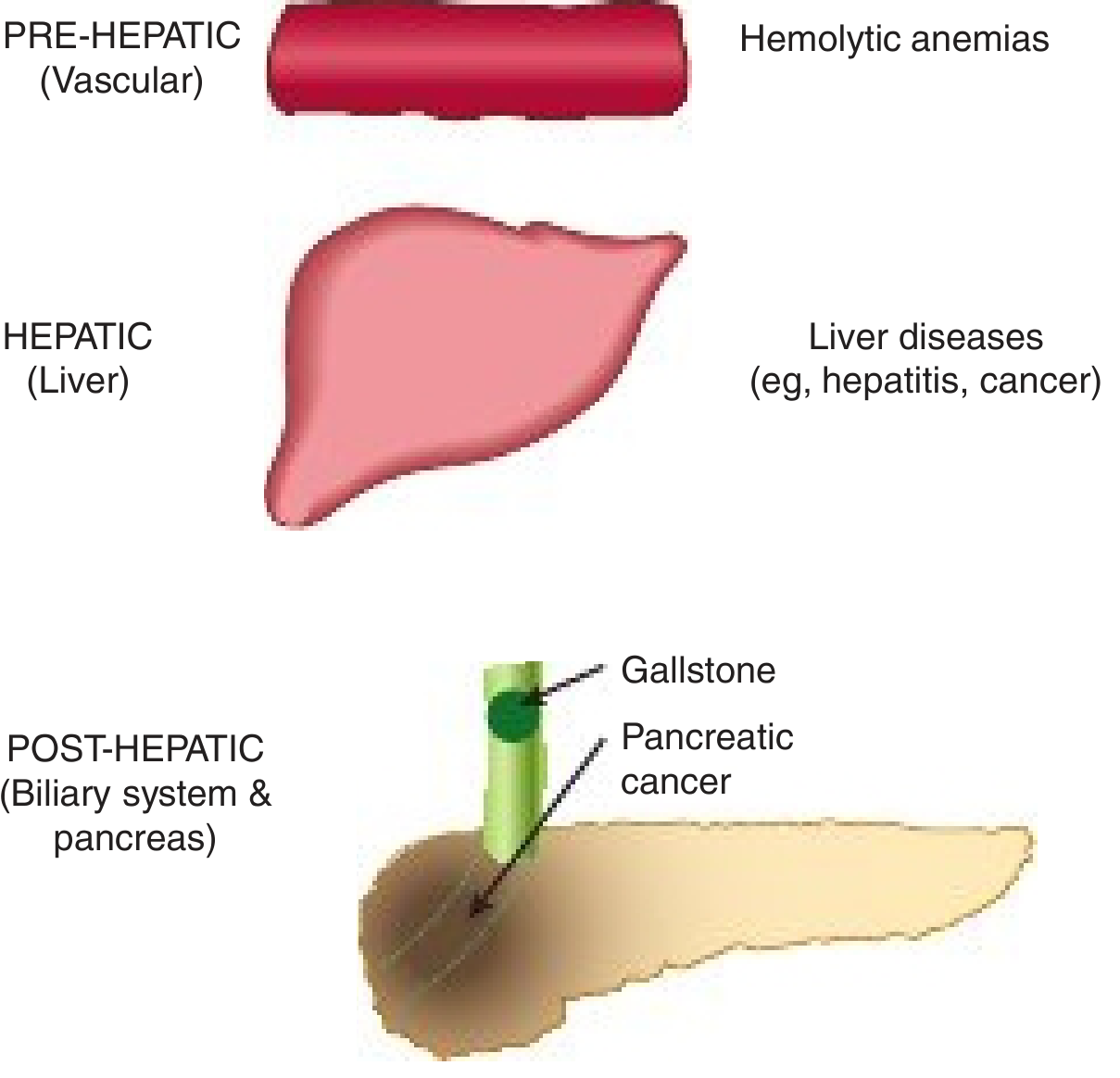
Figure: Major causes of jaundice. Prehepatic jaundice (vascular/bloodstream) = hemolytic anemias; Hepatic = liver diseases; Posthepatic = biliary obstruction (gallstone, pancreatic cancer). - Harper's Illustrated Biochemistry, 32nd Ed
Prehepatic jaundice refers to jaundice arising from events that occur before bilirubin reaches the liver. The core problem is excess bilirubin production - usually from hemolysis of red blood cells - that overwhelms the liver's conjugation capacity. The liver itself functions normally.
Bilirubin Metabolism - Background
When red blood cells are destroyed by the reticuloendothelial system, the iron from hemoglobin is recycled, and the porphyrin ring (globin) is broken down to form fat-soluble (unconjugated) bilirubin. This travels in the blood bound to albumin to the liver, where it is converted to a water-soluble (conjugated) form and secreted into the biliary tree and bowel.
- Gray's Anatomy for Students
Mechanism in Prehepatic Jaundice
The liver's excretory function is not impaired. However, red blood cells are hemolyzed so rapidly that hepatic cells simply cannot excrete bilirubin as fast as it is formed. As a result:
- Plasma unconjugated (indirect) bilirubin rises
- Urobilinogen formation in the intestine is greatly increased
- Much urobilinogen is reabsorbed into the blood and excreted in the urine
"In hemolytic jaundice, the excretory function of the liver is not impaired, but red blood cells are hemolyzed so rapidly that the hepatic cells simply cannot excrete bilirubin as quickly as it is formed."
- Guyton & Hall Textbook of Medical Physiology
Causes
Primary cause: Hemolytic anemia
The conjugation system is overwhelmed by excessive heme metabolism.
Inherited (immune-mediated - Coombs test positive):
- Autoimmune hemolytic anemia
- Drug-induced hemolytic anemia
Acquired non-immune-mediated (Coombs test negative):
- Drugs/toxins directly damaging RBCs
- Mechanical trauma (prosthetic heart valves)
- Microangiopathic hemolytic anemia (TTP, HUS)
- Infections (e.g., malaria)
- Incompatible blood transfusion
Hereditary RBC disorders:
- Hereditary spherocytosis
- Thalassemia
- G6PD deficiency
- Sickle cell disease
Other causes:
-
Failure of albumin transport of unconjugated bilirubin (e.g., severe burns, malnutrition with protein loss)
-
Inborn errors of bilirubin metabolism
-
Schwartz's Principles of Surgery, 11th Ed; Tintinalli's Emergency Medicine
Key Laboratory Features
The following table (from Harper's Illustrated Biochemistry, 32nd Ed) summarizes the lab findings across the three types of jaundice:
| Parameter | Normal | Hemolytic (Prehepatic) | Hepatitis (Hepatic) | Obstructive (Posthepatic) |
|---|---|---|---|---|
| Serum bilirubin (direct) | 0.1-0.4 mg/dL | Normal/slight rise | Raised | Raised (predominant) |
| Serum bilirubin (indirect) | 0.2-0.7 mg/dL | Raised | Raised | Normal/slight |
| Urine urobilinogen | 0-4 mg/24h | Increased | Decreased | Absent |
| Urine bilirubin | Absent | Absent | Present (if micro-obstruction) | Present |
| Fecal urobilinogen | 40-280 mg/24h | Increased | Decreased | Trace to absent |
Key pattern in prehepatic jaundice:
- Elevated indirect (unconjugated) bilirubin - the hallmark
- No bilirubin in urine (acholuric jaundice) - unconjugated bilirubin is albumin-bound and cannot be filtered by the kidneys
- Increased urine and fecal urobilinogen - more bilirubin delivered to the gut
Clinical Features
| Feature | Finding |
|---|---|
| Skin/sclera color | Yellow (mild - often lemon-yellow tinge) |
| Urine color | Normal or slightly dark (from urobilinogen, NOT bilirubin) |
| Stool color | Normal or dark (increased stercobilin) |
| Urine bilirubin (dipstick) | Negative |
| Splenomegaly | Often present (from active hemolysis) |
| Anemia | Present |
| Bilirubin level | Usually does not exceed 4-5 mg/dL (liver can compensate partially) |
Pathophysiology Summary
Excessive RBC destruction
↓
Overproduction of unconjugated bilirubin
↓
Liver conjugation capacity overwhelmed
↓
↑ Unconjugated bilirubin in blood (bound to albumin)
↓
Cannot cross glomerular filtration → NO bilirubin in urine
↓
More bilirubin conjugated and delivered to gut
↓
↑ Urobilinogen (gut) → reabsorbed → ↑ urine urobilinogen
→ ↑ stercobilinogen (dark stool)
Neonatal Prehepatic Jaundice - Special Note
In neonates, the hepatic conjugation machinery does not fully mature until ~2 weeks of age. Almost every newborn develops transient mild unconjugated hyperbilirubinemia (physiologic jaundice). Hemolytic disease of the newborn (erythroblastosis fetalis) causes severe unconjugated hyperbilirubinemia - the unbound fraction can diffuse into the brain, causing kernicterus (severe neurologic damage). Treatment is phototherapy (blue light converts bilirubin to a soluble isomer for urinary excretion) or exchange transfusion.
- Robbins & Kumar Basic Pathology
Differentiation from Other Types of Jaundice
| Feature | Prehepatic | Hepatic | Posthepatic |
|---|---|---|---|
| Primary bilirubin | Unconjugated (indirect) | Mixed | Conjugated (direct) |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | Increased | Decreased | Absent |
| Stool color | Normal/dark | Pale | Pale/clay-colored |
| van den Bergh test | Indirect positive | Both positive | Direct positive |
| LFTs | Usually normal | Elevated (transaminases) | Elevated (ALP, GGT) |
The van den Bergh reaction is the classic chemical test used to differentiate unconjugated from conjugated bilirubin in plasma. - Guyton & Hall
Sources: Gray's Anatomy for Students | Guyton & Hall Textbook of Medical Physiology | Schwartz's Principles of Surgery, 11th Ed | Tintinalli's Emergency Medicine | Harper's Illustrated Biochemistry, 32nd Ed | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.