hill sachs lesion and bankart lesion . Explain these two terms in detail
Reading File
Finding Sources
Searching Images
Hill Sachs lesion Bankart lesion shoulder dislocation
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive information from authoritative sources. Let me compile the full answer.
Hill-Sachs Lesion & Bankart Lesion
These are the two classic companion injuries of anterior glenohumeral (shoulder) dislocation — one affects the humeral head, the other the glenoid. Together they are called "bipolar lesions" and are the principal anatomical basis for recurrent shoulder instability.
Anatomy Refresher
The glenohumeral joint is a ball-and-socket joint with inherent bony instability (shallow socket). Static stability depends heavily on the glenoid labrum (a fibrocartilaginous ring deepening the socket) and the glenohumeral ligaments. During an anterior dislocation, the humeral head is forced anteriorly/inferiorly, generating two impact events:
- The anterior-inferior glenoid rim chips/tears (Bankart lesion)
- The posterolateral humeral head impacts the firmer glenoid rim and dents (Hill-Sachs lesion)
1. Bankart Lesion
Definition
A tear or avulsion of the anteroinferior glenoid labrum (with or without a bone fragment) from the anterior rim of the glenoid fossa. Named after British surgeon Arthur Sydney Blundell Bankart, who identified it in 1923 as the "essential lesion" creating shoulder instability.
"Bankart originally identified the labral tear as the essential lesion creating shoulder instability." — Rockwood and Green's Fractures in Adults, 10th ed.
Types
| Type | Description |
|---|---|
| Soft-tissue Bankart | Pure labrolligamentous detachment; no bone fracture; labrum stripped off glenoid rim with intact glenoid periosteum |
| Bony (Osseous) Bankart | Avulsion fracture of the anterior-inferior glenoid rim with attached capsulolabral structures; a fragment of bone is displaced |
| ALPSA lesion | Anterior Labroligamentous Periosteal Sleeve Avulsion — labrum peels off medially but periosteum remains intact |
| HAGL lesion | Humeral Avulsion of Glenohumeral Ligament — avulsion from the humeral side (variant) |
Mechanism
During anterior shoulder dislocation, the anteriorly displaced humeral head levers against the anterior glenoid rim, shearing off the labrum and inferior glenohumeral ligament (IGHL) complex.
Epidemiology / Clinical Significance
- Glenoid bone loss is present in 40% of first dislocations and 85% of recurrent dislocations
- A bony Bankart fragment undergoes rapid resorption within 1 year of the primary injury
- >20–25% glenoid bone loss (≈6–8 mm) is the critical threshold: above this, arthroscopic Bankart repair alone has a recurrence rate of 67% (vs. 4% with intact glenoid)
- Recurrence rate of shoulder dislocation in young adults can exceed 90% if not surgically repaired
— Miller's Review of Orthopaedics, 9th Edition; Rockwood and Green's, 10th ed.
Imaging
- X-ray: Frontal/axillary views may show bony fragment; Garth view useful
- MRI/MR Arthrogram: Best for soft-tissue Bankart — shows labral detachment and disruption of IGHL
- CT with 3D reconstruction: Best for bony Bankart — quantifies bone loss for surgical planning; humeral head can be digitally subtracted
2. Hill-Sachs Lesion
Definition
A posterolateral impaction fracture (compression defect) of the humeral head caused by its forceful contact with the harder anterior glenoid rim during anterior shoulder dislocation. Named after radiologists Harold Arthur Hill and Maurice David Sachs, who described it in 1940.
"A Hill-Sachs lesion represents an impaction fracture of the posterior humeral head against the firmer glenoid rim." — Rockwood and Green's Fractures in Adults, 10th ed.
Mechanism
During anterior dislocation, the soft cancellous bone of the posterolateral humeral head is driven against the harder cortical glenoid rim, producing a wedge-shaped or trough-shaped cortical depression.
Epidemiology
| Clinical Setting | Prevalence of Hill-Sachs Lesion |
|---|---|
| Recurrent subluxation (no dislocation) | ~40% |
| First-time dislocation | ~90% |
| Recurrent dislocations | ~100% |
Key Concept: Engaging vs. Non-Engaging
- Non-engaging: The Hill-Sachs defect does not align with the glenoid rim during functional range of motion — clinically less significant
- Engaging: When the shoulder is placed in abduction and external rotation, the rim of the Hill-Sachs defect aligns with and "catches" on the anterior glenoid rim → the humeral head subluxes or dislocates. This is clinically significant and a determinant of surgical approach.
The "On-Track" vs. "Off-Track" Concept
Modern evaluation combines both lesions using the glenoid track concept:
- The glenoid track = 84% of the glenoid width
- If the Hill-Sachs lesion (measured as width from rotator cuff footprint to medial margin of the defect) extends beyond the glenoid track → "Off-track" = HIGH RISK of engaging; arthroscopic labral repair alone is insufficient
- If within the glenoid track → "On-track" = low risk; standard Bankart repair can suffice
— Miller's Review of Orthopaedics, 9th Edition
Imaging
- X-ray: Best seen on Stryker notch view and Garth view (posterior/superolateral humeral head notch)
- CT with 3D reconstruction: Gold standard for measuring lesion size and the glenoid track
- MRI: Shows bone marrow edema (acute phase) and cortical depression (chronic); MR arthrogram additionally shows associated labral pathology
The Bipolar Lesion Concept
When Hill-Sachs and Bankart lesions occur together, they are called bipolar lesions. This is critical because each lesion individually may be tolerable, but combined they dramatically increase instability risk:
- Prevalence: 33% in primary instability, 62% in recurrent instability
- Postoperative recurrence with bipolar lesions: 29%
- Management must address both sides of the pathology
— Rockwood and Green's Fractures in Adults, 10th ed.
Surgical Management Summary
| Lesion | Soft-Tissue / Small Bony | Large Bone Loss / Engaging |
|---|---|---|
| Bankart | Arthroscopic Bankart repair (labral reattachment) | Latarjet procedure (coracoid transfer to glenoid) |
| Hill-Sachs | Often observed if non-engaging | Remplissage (filling defect with infraspinatus tendon) or allograft |
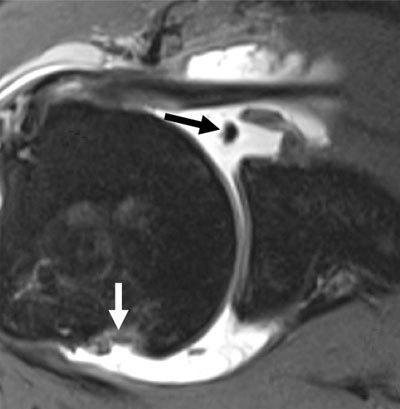
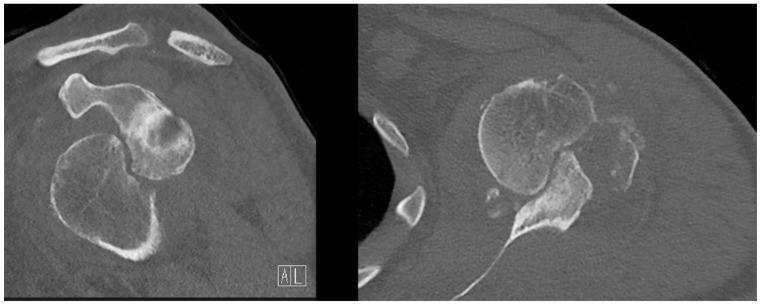
Imaging Examples
MR Arthrogram (Axial) — Soft-tissue Bankart lesion (white arrow, anterior-inferior glenoid) and Hill-Sachs deformity (black arrow, posterolateral humeral head):
CT Scan (Coronal and Axial) — Bony Bankart lesion (anterior-inferior glenoid rim defect) and large Hill-Sachs deformity (posterolateral humeral head depression) representing bipolar bone loss:
Reverse Variants (Posterior Dislocation)
| Classic Lesion | Reverse Lesion (posterior dislocation) |
|---|---|
| Hill-Sachs (posterolateral humeral head) | Reverse Hill-Sachs (anterolateral humeral head) |
| Bankart (anterior-inferior glenoid) | Reverse Bankart (posterior glenoid rim fracture) |
Sources: Rockwood and Green's Fractures in Adults 10th ed. | Miller's Review of Orthopaedics 9th ed. | Tintinalli's Emergency Medicine | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.