Infertility
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"female infertility"[MeSH Terms] AND "etiology"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
"infertility" AND "treatment" AND "women"
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Female Infertility - In-Depth Textbook Coverage
1. Definition & Epidemiology
Infertility is defined as failure of conception after 12 months of unprotected intercourse (6 months if the woman is >35 years old, or if either partner has a known risk factor). From 15-20% of all couples are infertile.
Age and fertility: Fertility peaks between ages 20-24. The decline in fecundability begins in the early 30s and accelerates in the late 30s and early 40s, with a steep decline after age 40.
Attribution of infertility:
- ~1/3 female factors
- ~1/3 male factors
- ~1/3 combined or unexplained
Berek & Novak's Gynecology, p. 2018; Textbook of Family Medicine 9e, p. 1051
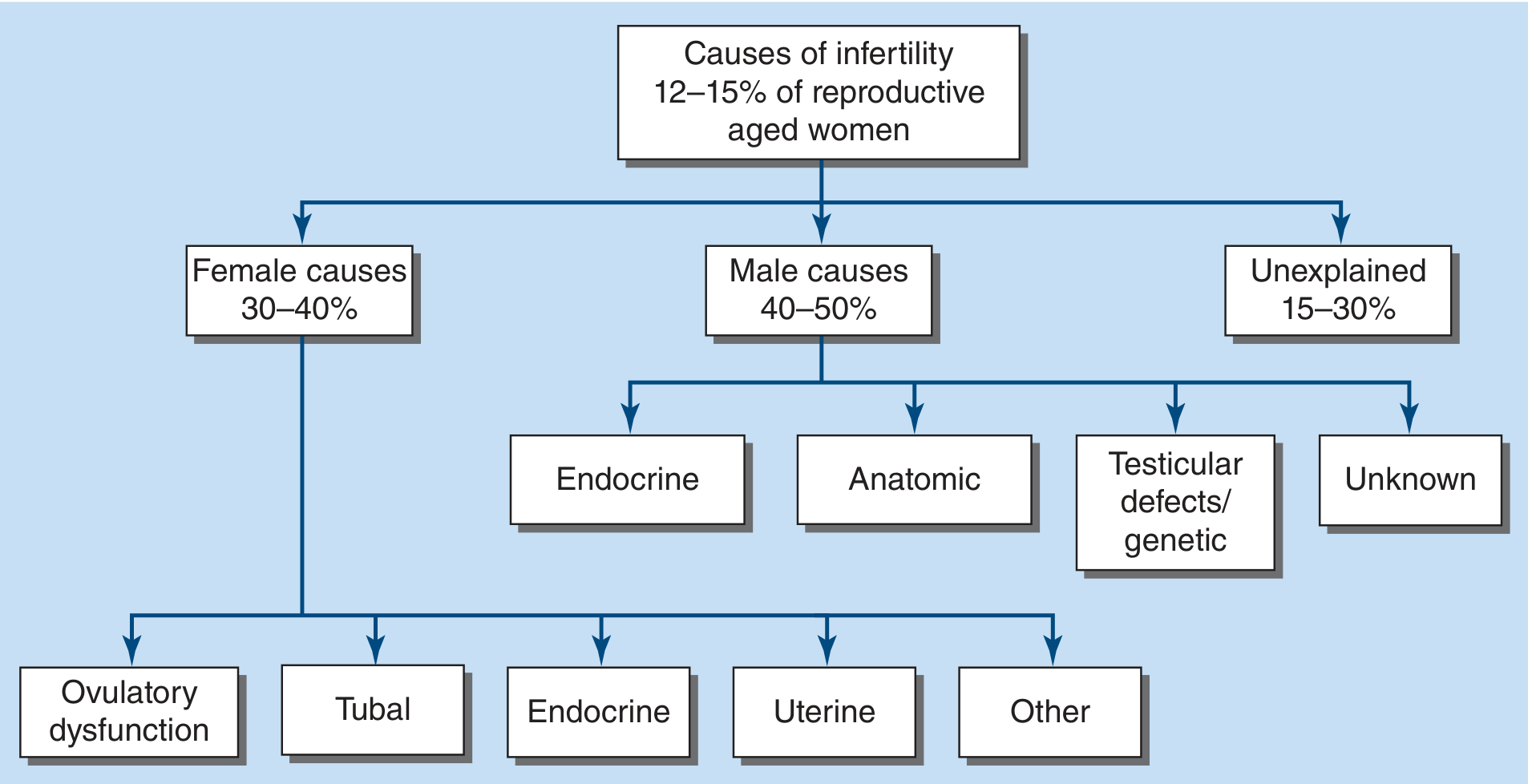
2. Causes of Female Infertility
The approximate prevalence of each cause in women:
| Cause | Approximate Prevalence |
|---|---|
| Ovulatory dysfunction | 21-36% (up to 30-40% in some sources) |
| Tubal or peritoneal factor | 30-40% |
| Uterine pathology | up to 15% |
| Cervical factor | <5% |
| Unexplained | 8-28% |
A. Ovarian / Hormonal Factors
- PCOS - the most common single cause of oligo-ovulation and anovulation in reproductive-age women
- Hypergonadotropic hypogonadism - primary ovarian insufficiency (POI), menopause, gonadal dysgenesis, resistant ovary syndrome, autoimmune/chemo/radiation damage
- Hypogonadotropic hypogonadism - hypothalamic suppression (stress, anorexia, extreme exercise, low BMI), Kallmann syndrome, pituitary adenoma/necrosis/tumor
- Hyperprolactinemia - pituitary tumor, drugs
- Thyroid / metabolic disease - obesity, androgen excess, liver disease
- Luteal phase deficiency
B. Tubal Factors
- Occlusion or scarring (pelvic inflammatory disease, STIs)
- Salpingitis isthmica nodosa
- Infectious salpingitis
- Peritubal/paratubal adhesions (including from endometriosis)
C. Uterine Factors
- Leiomyomata (fibroids)
- Congenital malformations (e.g., septate uterus)
- Adhesions (Asherman syndrome)
- Endometritis / abnormal endometrium
D. Cervical Factors
- Stenosis
- Inflammation/infection
- Abnormal mucus viscosity
E. Peritoneal Factors / Endometriosis
Endometriosis with tubal or peritoneal adhesions is categorized as a tubal-peritoneal factor; without adhesions, it is listed under unexplained infertility.
F. Psychosocial/Other
- Decreased libido, anorgasmia
- Immunologic factors (antisperm antibodies)
- Iatrogenic causes
Berek & Novak's Gynecology, Box/Table; Tietz Textbook of Laboratory Medicine 7e, Box 58.5
3. Diagnostic Algorithm
Evaluation should begin after:
- 12 months of unprotected intercourse in women <35 with regular cycles
- 6 months in women >35, or sooner if irregular menses, history of PID/STI, or exposure to gonadotoxins
Initial evaluation includes:
History:
- Menstrual history (cycle length, regularity, moliminal symptoms)
- Coital frequency and timing
- Duration of infertility and prior workup/treatment
- History of STIs, PID, pelvic surgery, cervical dysplasia/treatment
- Medications, tobacco, alcohol, BMI
Physical examination:
- External genitalia and hair pattern - signs of androgen excess (clitoromegaly, hirsutism, virilization)
- Pelvis - masses, nodularity, tenderness
- Breasts - galactorrhea
- Neurologic findings - smell, visual fields
- Thyroid - enlargement, nodules
- BMI
The diagnostic algorithm from Tietz Textbook of Laboratory Medicine, 7e summarizes the stepwise approach:
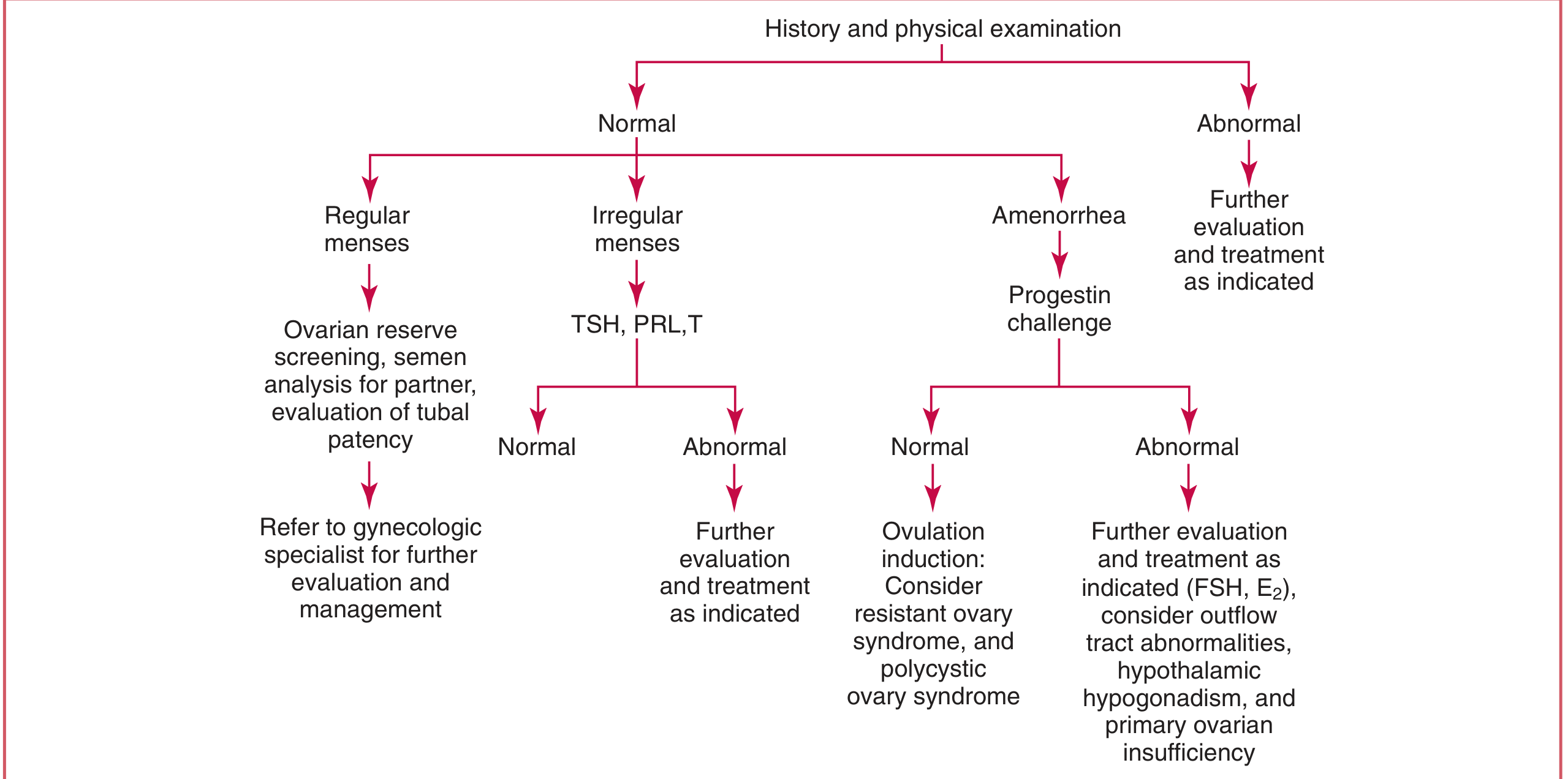
4. Investigations
Ovulation Assessment
- Urinary LH surge kits (OPKs) - predict ovulation prospectively
- Midluteal serum progesterone - measured 7 days before anticipated menses (day 21 in a 28-day cycle). Values >300 ng/dL (>9.5 nmol/L) confirm ovulation (corpus luteum formation)
- Basal body temperature (BBT) - a rise of 0.5-1°F after ovulation creates a biphasic pattern; limited because it cannot prospectively predict ovulation
- Transvaginal ultrasound - follicular tracking and monitoring
If cycles are absent or irregular, or signs of galactorrhea/thyroid disease are present: check TSH, prolactin, testosterone, FSH
Ovarian reserve testing (especially if >35, or diminished reserve suspected):
- Day 3 FSH - values >12 IU/L associated with poor ovarian response
- Anti-Mullerian hormone (AMH) and antral follicle count (AFC) by transvaginal ultrasound
Tubal Assessment
| Test | Features |
|---|---|
| Hysterosalpingography (HSG) | First-line; assesses tubal patency and uterine cavity; discomfort, iodinated contrast |
| Laparoscopy with chromotubation | Gold standard for tubal patency; also diagnoses adhesions and endometriosis |
| Fluoroscopic/hysteroscopic tubal cannulation | For suspected proximal occlusion |
Uterine Assessment
| Test | Features |
|---|---|
| Transvaginal ultrasound | 75% PPV for polyps; poor for adhesions |
| Sonohysterography (SIS) | 100% sensitivity/specificity for polyps; well-tolerated; also evaluates adnexa |
| HSG | Shows cavity contour; 50% sensitivity for polyps (vs. hysteroscopy) |
| Hysteroscopy | Gold standard for uterine cavity; direct visualization; gold standard for adhesions |
| MRI | For myometrium and congenital anomalies |
Cervical Assessment
- Cervical mucus evaluation
- Postcoital test (limited sensitivity)
Berek & Novak's Gynecology, Tietz Textbook, Family Medicine 9e
5. The "Fertile Window"
The fertile window is the 6-day interval ending on the day of ovulation. Sperm survive up to 6 days in well-estrogenized cervical mucus, but the egg is fertilizable for less than 1 day. The average woman is fertile between days 10-17, but there is wide variability. Intercourse 2-3 times per week throughout the cycle will usually include the fertile window, and is a practical alternative to timed intercourse tracking.
6. Management by Cause
A. Ovulatory Factor (Anovulation/Oligo-ovulation)
PCOS - first-line:
- Lifestyle modification - weight loss of even 5% improves pregnancy rates in overweight/obese women; reduce daily calories by 500 kcal + regular exercise
- Ovulation induction agents:
Letrozole (Femara) - aromatase inhibitor, currently preferred over clomiphene for PCOS:
- Mechanism: reduces ovarian estrogen → removes E2 negative feedback on pituitary → FSH rises → follicular development
- Half-life: 48 hours (shorter than clomiphene)
- Dose: 2.5 mg, cycle days 3-7, for up to 5 cycles
- Evidence: In a multicenter RCT of 750 women with PCOS, cumulative live birth rate was significantly higher with letrozole vs. clomiphene (27.5% vs. 19.1%; RR 1.44, 95% CI 1.10-1.87), with similar twin rates (3.4% vs. 7.4%)
Clomiphene citrate (Clomid, Serophene) - historical first-line, now second-line to letrozole:
- Mechanism: weak synthetic estrogen acting as estrogen antagonist; blocks hypothalamic estrogen receptors → increases GnRH pulsatility → increased FSH/LH → follicular development
- Half-life: 2 weeks
- Effectiveness over 6 months: 49% ovulation rate, 23.9% pregnancy rate, 22.5% live birth rate
- Decreased effectiveness with obesity, increased age, hyperandrogen states
- Side effects: vasomotor flushes, mood swings, breast tenderness, nausea; antiestrogenic effects on endometrium/cervix in a minority
- Multiple gestation: ~8% (mostly twins)
- Contraindicated in: pregnancy, ovarian cysts (non-PCOS), uncontrolled thyroid/adrenal disease, undiagnosed abnormal uterine bleeding, sex hormone-dependent tumors
Gonadotropins (FSH/LH injections) - for clomiphene/letrozole failure; careful monitoring required to reduce multiple gestation and OHSS risk
B. Hyperprolactinemia
- MRI pituitary to exclude macroadenoma
- Dopamine agonists are first-line:
- Bromocriptine 1.25-2.5 mg daily (titrate); normalizes prolactin and restores ovulation in 80-90%; side effects: nausea, vomiting, postural hypotension, headache
- Cabergoline 0.25 mg twice weekly; fewer side effects, better tolerated; safety at conception confirmed in >700 cases (no increased miscarriage or malformation rates)
C. Hypogonadotropic Hypogonadism
- Address reversible causes: normalize body weight, reduce exercise, treat eating disorders
- Exogenous leptin has been reported to restore ovulation in diet/exercise-induced amenorrhea
- Gonadotropin therapy (FSH + LH/hCG) or pulsatile GnRH (when hypothalamic dysfunction) for those who do not respond to lifestyle changes
- Exclude intracranial lesions with MRI
D. Tubal Factor
- Mild proximal occlusion: fluoroscopic or hysteroscopic tubal cannulation
- Surgical repair (tuboplasty/salpingostomy) for distal disease; success depends on extent of damage
- IVF is the definitive treatment when tubal disease is severe or surgery fails; also indicated in cases of bilateral salpingectomy
E. Uterine Factor
- Submucosal fibroids and endometrial polyps: operative hysteroscopy for resection
- Intrauterine adhesions: hysteroscopic adhesiolysis
- Congenital anomalies (e.g., uterine septum): hysteroscopic metroplasty
F. Cervical Factor
- Often managed with intrauterine insemination (IUI), which bypasses the cervix
G. Unexplained Infertility
- Superovulation + IUI - reasonable first step; less successful than ART
- IVF - for those who fail superovulation/IUI
7. Assisted Reproductive Technology (ART)
ART techniques include:
- IUI (intrauterine insemination) - best studied insemination technique; bypasses cervical factor
- IVF (in vitro fertilization) - gold standard; indicated for tubal disease, severe male factor, unexplained infertility after failed simpler therapies
- ICSI (intracytoplasmic sperm injection) - for male factor infertility; ART outcomes comparable to non-male-factor IVF when ICSI is used
- GIFT (gamete intrafallopian transfer) and ZIFT (zygote intrafallopian transfer) - largely replaced by IVF due to improved IVF success rates
- Oocyte/embryo cryopreservation - for fertility preservation (e.g., before chemotherapy)
- Preimplantation genetic diagnosis/screening (PGD/PGS) and morphokinetic embryo selection
- Gestational carriers - for women with uterine factor or inability to carry pregnancy
Multiple gestation remains the principal risk of ART and ovulation induction. Single embryo transfer (SET) strategies are recommended where possible.
Berek & Novak's Gynecology, p. 2083
8. Special Considerations
Age
Ovarian reserve declines progressively from the early 30s, with acceleration after 35-40. Women >35 should have FSH measured on day 3; FSH >12 IU/L suggests poor ovarian response and warrants referral to a reproductive endocrinologist. Chemotherapy may hasten ovarian reserve loss - fertility preservation counseling should be offered before starting gonadotoxic therapy.
Endometriosis
- Associated with infertility via tubal/peritoneal adhesions, altered pelvic environment
- Surgical laparoscopy (ablation/excision of lesions) may improve fertility in minimal/mild disease
- Moderate-severe disease: IVF is usually preferred
- Medical suppression of endometriosis (GnRH agonists, etc.) does NOT improve fertility
Obesity
- Associated with anovulation, PCOS, and poor ART outcomes
- Weight loss of 5% or more can restore ovulation and improve pregnancy rates
- Weight loss surgery should precede conception attempts in severely obese patients
Thyroid Disease
- TSH should be checked in women with irregular cycles or signs of thyroid disease
- Both hypo- and hyperthyroidism impair fertility; correction is essential before treatment
9. Key Points Summary
| Factor | Proportion of Female Infertility | First-line Management |
|---|---|---|
| Ovulatory dysfunction | 30-40% | Letrozole (PCOS); dopamine agonist (hyperprolactinemia); lifestyle (hypothalamic) |
| Tubal/peritoneal | 30-40% | Surgical repair or IVF |
| Uterine | up to 15% | Operative hysteroscopy |
| Cervical | <5% | IUI |
| Unexplained | 8-28% | Superovulation + IUI, then IVF |
Sources:
- Berek & Novak's Gynecology - Chapter 36 (Infertility), pp. 2018-2090
- Tietz Textbook of Laboratory Medicine, 7th Edition - Chapter 58 (Female Infertility evaluation), pp. 2381-2390
- Textbook of Family Medicine, 9th Edition - Chapter 35, pp. 1051-1053
Recent PubMed evidence:
- A 2025 systematic review and meta-analysis in Fertil Steril (PMID 39332623) examined therapeutic management for diminished ovarian reserve from RCTs.
- A 2024 meta-analysis in Adv Nutr (PMID 39019217) evaluated antioxidant supplementation in women with ovarian aging.
- A 2024 systematic review in BMC Women's Health (PMID 39707272) identified sleep disturbances as a factor in female infertility.
Primary and secondary
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative textbook content from four sources. Here is the full in-depth answer.
Primary vs. Secondary Infertility
Definitions
| Term | Definition |
|---|---|
| Infertility | Failure to conceive after 12 months of regular, unprotected intercourse (6 months if female partner >35 years; evaluate immediately if >40 years) |
| Primary infertility | The couple (or individual) has never conceived - no previous pregnancy of any kind |
| Secondary infertility | The couple has previously conceived (although not necessarily resulting in a live birth) but is currently unable to conceive again |
| Subfertility | Often used interchangeably with infertility |
| Fecundability | Probability of achieving pregnancy per menstrual cycle |
| Fecundity | Probability of achieving a live birth per cycle |
"Primary infertility, in which no previous pregnancies have occurred, and secondary infertility, in which a prior pregnancy, although not necessarily a live birth, has occurred."
- Berek & Novak's Gynecology, p. 2019
Why the Distinction Matters
The classification guides the probability of a prior reproductive event being relevant to the current problem:
- Primary infertility suggests the couple has never successfully fertilized an egg and implanted, pointing toward congenital, structural, genetic, or longstanding ovulatory/endocrine causes
- Secondary infertility confirms the reproductive tract has worked at least once, so the investigation focuses more on acquired causes - things that happened after the previous pregnancy (e.g., post-partum complications, new infection, progressive disease like endometriosis, age-related ovarian decline)
"These types of infertility generally share common causes."
- Tietz Textbook of Laboratory Medicine, 7e, p. 2378
Despite this, the underlying causes overlap considerably - the same factors (ovulatory dysfunction, tubal disease, male factor) are found in both types.
Epidemiology
- WHO classifies infertility as a disease of the reproductive system - the third most common disease worldwide
- Affects approximately 48-72 million couples globally
- Global prevalence: ~17.5% (has remained relatively stable over decades)
- ~85-90% of couples with regular unprotected intercourse will conceive within 12 months
- ~95% will conceive within 24 months
- A specific identifiable cause is found in ~80% of couples
Distribution of causes (overall - both primary and secondary combined):
| Cause category | Proportion |
|---|---|
| Female factors | 30-40% |
| Male factors | 40-50% |
| Both female + male | 20-30% |
| Unexplained | 15-30% |
Causes Particularly Associated with PRIMARY Infertility
These are causes that typically prevent any conception from occurring - they are congenital or longstanding from the outset:
Female:
- Congenital Müllerian anomalies (absent/bicornuate/septate uterus, vaginal agenesis)
- Gonadal dysgenesis (Turner syndrome - 45,XO - absent functional ovaries from birth)
- Kallmann syndrome - congenital hypothalamic GnRH deficiency with anosmia
- Primary ovarian insufficiency presenting before any pregnancy
- Congenital tubal aplasia / atresia
- Androgen insensitivity syndrome (46,XY female phenotype - no uterus/ovaries)
Male:
- Congenital bilateral absence of the vas deferens (CBAVD) - associated with CFTR mutations (cystic fibrosis)
- Klinefelter syndrome (47,XXY) - azoospermia
- Y chromosome microdeletions affecting spermatogenesis
- Congenital hypogonadotropic hypogonadism (Kallmann)
Varicoceles are found in approximately 35% of men with primary infertility but 75-81% of men with secondary infertility - Campbell-Walsh Urology, p. block37
Causes Particularly Associated with SECONDARY Infertility
These are acquired causes developing after the first pregnancy:
Female:
- Intrauterine adhesions (Asherman syndrome) - most commonly from post-partum or post-abortion D&C, endometritis. Adhesions are a major cause of secondary infertility
- Post-partum endometritis progressing to uterine scarring
- Pelvic inflammatory disease (PID) - STI acquired after the first pregnancy causing tubal scarring
- Endometriosis - progressive disease that worsens with time
- Post-surgical adhesions (from Caesarean section, myomectomy, appendectomy)
- Age-related diminished ovarian reserve - acquired from the first pregnancy onward
- New-onset hyperprolactinemia (post-partum pituitary adenoma)
- Weight gain / new-onset PCOS after first pregnancy
Male:
- Varicocele (progressive testicular damage - explains why varicocele is found in 75-81% of secondary vs. 35% of primary male infertility cases)
- Post-infectious epididymo-orchitis (e.g., mumps orchitis after the first pregnancy)
- Acquired obstruction of vas deferens from prior surgery
Comparison Table
| Feature | Primary Infertility | Secondary Infertility |
|---|---|---|
| Previous pregnancy | Never | Yes (any outcome including miscarriage, ectopic) |
| Typical cause bias | Congenital, structural, longstanding | Acquired, progressive, post-partum complications |
| Varicocele in males | ~35% | ~75-81% |
| Asherman syndrome | Rare | More common (post-D&C, post-partum) |
| Endometriosis | Can present in either; tends to worsen over time | Common cause of worsening after first pregnancy |
| Age-related decline | Less prominent (presentation often younger) | More prominent |
| Prognosis | Generally less favorable (more likely structural) | Often more amenable to treatment |
Evaluation Approach (Applies to Both Types)
The workup is essentially the same regardless of primary vs. secondary status, though secondary infertility prompts particular attention to acquired uterine pathology.
Timing of evaluation:
- <35 years: after 12 months of trying
-
35 years: after 6 months
-
40 years: evaluate immediately
- Earlier if known risk factors (irregular cycles, prior PID, prior pelvic surgery)
Key investigations:
| System | Test |
|---|---|
| Ovulation | Urinary LH surge kit; mid-luteal serum progesterone (day 21); BBT (less reliable) |
| Ovarian reserve | Day 2-3 serum FSH + E2; serum AMH; antral follicle count (AFC) by USS |
| Endocrine | TSH, prolactin, testosterone (if irregular cycles or signs of hyperandrogenism) |
| Tubal | Hysterosalpingogram (HSG) - first-line; laparoscopy + chromotubation - gold standard |
| Uterine cavity | Sonohysterography (SIS) - best for polyps/adhesions; hysteroscopy - gold standard |
| Male partner | Semen analysis x2 (2-7 days abstinence); endocrine evaluation if abnormal |
Not indicated as part of initial workup: diagnostic laparoscopy, postcoital test, endometrial biopsy, thrombophilia testing, immunologic testing, or karyotype (unless specific indications are present) - Harrison's Principles of Internal Medicine, 22e
Fecundability and Age-Related Decline
This is relevant to both types but hits harder in secondary infertility due to elapsed time:
| Age group (female) | Reduction in fecundability vs. age 30-31 |
|---|---|
| 34-35 years | -14% |
| 36-37 years | -19% |
| 40-41 years | -53% |
| 42-44 years | -59% |
The decline after 35 is primarily due to chromosomal abnormalities in oocytes during meiosis. A similar decline is NOT observed in men under 50.
Harrison's Principles of Internal Medicine, 22e, p. 3193
Sources:
- Berek & Novak's Gynecology, pp. 2018-2019
- Tietz Textbook of Laboratory Medicine, 7th Edition, p. 2378
- Harrison's Principles of Internal Medicine, 22e, pp. 3192-3194
- Swanson's Family Medicine Review - Definitions section
- Campbell-Walsh Urology - Varicocele sections
This is a shared conversation. Sign in to Orris to start your own chat.