Research on febuxostat in inflammatory edema
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Based on a thorough search across multiple authoritative pharmacology and medical textbooks, here is a comprehensive research summary on febuxostat in inflammatory edema:
Febuxostat in Inflammatory Edema
Overview
The textbook literature does not describe febuxostat as a primary agent for inflammatory edema — it is approved as a urate-lowering therapy for chronic hyperuricemia in gout. However, its anti-inflammatory relevance in the context of edema arises through several interconnected mechanisms.
1. Mechanism of Action
Febuxostat is a potent, selective, nonpurine inhibitor of xanthine oxidase (XO). Unlike allopurinol (whose active metabolite oxypurinol inhibits only the reduced form of XO), febuxostat forms a stable complex with both the reduced and oxidized forms of xanthine oxidase, providing more complete and sustained inhibition.
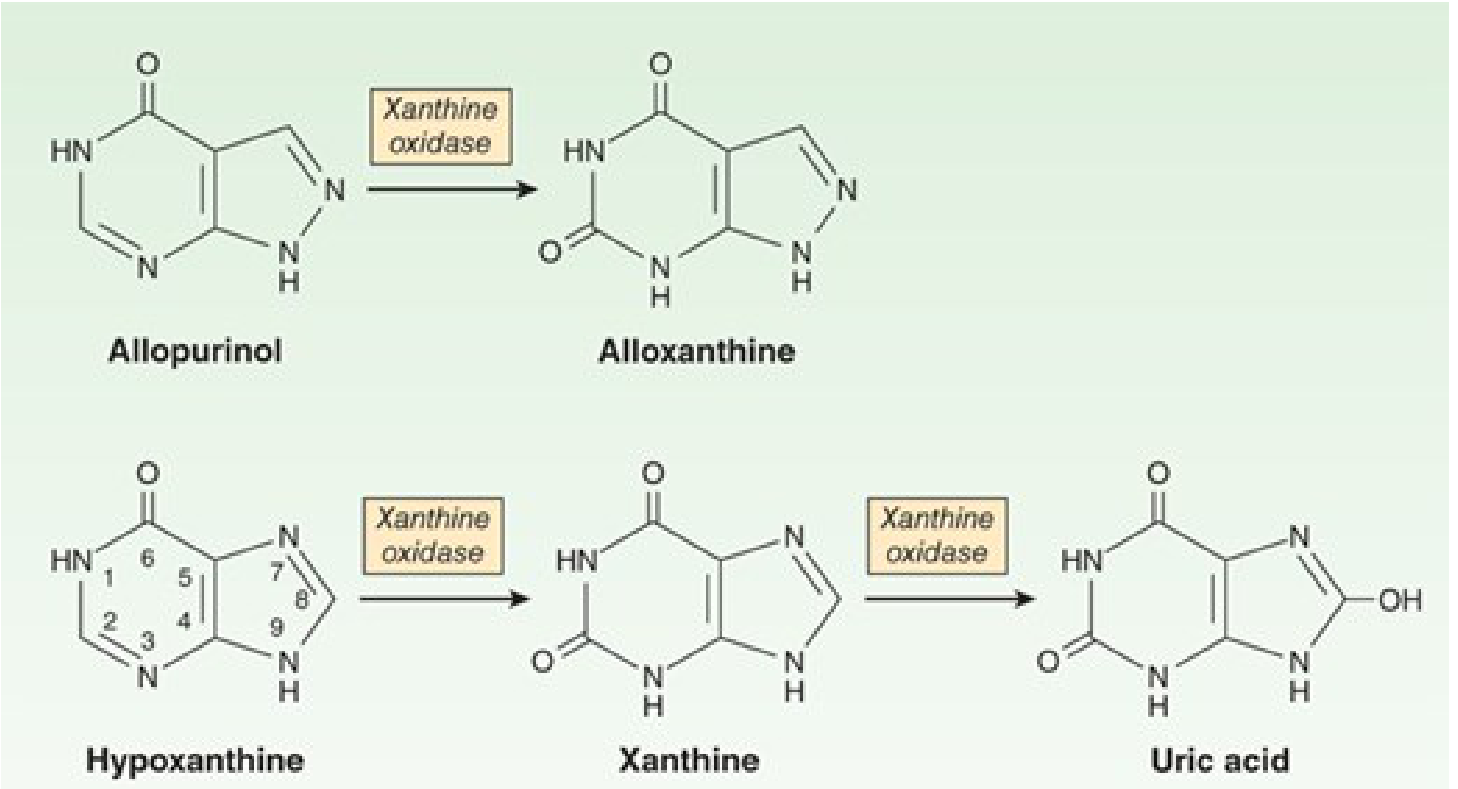
Xanthine oxidase converts hypoxanthine → xanthine → uric acid. Febuxostat blocks both steps. — Katzung's Basic and Clinical Pharmacology, 16th Ed.
2. Link Between Xanthine Oxidase, Oxidative Stress, and Inflammatory Edema
Xanthine oxidase is a key generator of reactive oxygen species (ROS), particularly superoxide and hydrogen peroxide, during purine catabolism. The relevance to inflammatory edema is mechanistic:
- XO-derived ROS amplify endothelial cell dysfunction, increasing vascular permeability — the principal pathophysiologic driver of inflammatory edema.
- Increased XO activity has been documented in conditions associated with oxidative stress and vascular injury (heart failure, pulmonary hypertension, hypertension, ischemia-reperfusion).
- Reduced nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, uncoupled NO synthase, and xanthine oxidase together constitute the major enzymatic sources of ROS in inflamed tissues. — Braunwald's Heart Disease, p. 1207
- XO-derived ROS have been shown to display biphasic effects on endothelial cell adhesion and FAK signaling, linking XO activity directly to the inflammatory cascade that leads to tissue edema. — Fishman's Pulmonary Diseases and Disorders
By inhibiting XO, febuxostat reduces not only uric acid production but also ROS generation, potentially attenuating endothelial permeability and inflammatory edema.
3. Inflammatory Edema in Gout — The Clinical Context
The most direct and clinically validated association between febuxostat and inflammatory edema is in gout:
- Gouty inflammation is characterized by acute inflammatory edema of joints triggered by monosodium urate crystal deposition. These crystals activate macrophages and the NLRP3 inflammasome, releasing IL-1β, TNF, and other cytokines that promote local vasodilation and edema.
- Febuxostat lowers serum uric acid, reducing the urate burden available for crystal deposition and preventing recurrent episodes of inflammatory edema (acute gouty attacks).
- Gout flares (inflammatory edema flares) are paradoxically more common at treatment initiation, because rapid reduction in serum urate mobilizes urate from tissue deposits, triggering crystal-induced inflammation. Prophylactic colchicine or NSAIDs are therefore co-prescribed at the start of therapy. — Goodman & Gilman's, p. 600; Katzung's, p. 1031
4. Pharmacokinetics Relevant to Edema Settings
| Parameter | Detail |
|---|---|
| Absorption | >80% oral bioavailability; Tmax ~1 hour |
| Half-life | 4–8 hours; once-daily dosing effective |
| Metabolism | Extensive hepatic (UGT + CYP1A2, 2C8, 2C9) |
| Elimination | Hepatic + renal; no dose adjustment needed in mild-to-moderate CKD |
| Renal safety | Safe in moderate CKD — unlike allopurinol, which requires dose reduction |
The hepatic-predominant elimination is clinically important in patients with nephrotic syndrome or heart failure-associated edema, where renal clearance is compromised. — Goodman & Gilman's, p. 590; Brenner and Rector's The Kidney, p. 1739
5. Adverse Effects Relevant to Edema
- Gout flares (paradoxical inflammatory edema) at treatment initiation — mitigated by prophylaxis
- Liver function abnormalities, nausea, rash, diarrhea, headache
- Cardiovascular risk: A boxed warning exists for possible increased cardiovascular death vs. allopurinol (higher rates of MI and stroke seen in some trials, though more recent data has not confirmed increased MACE). This is relevant in edematous patients (e.g., heart failure), where cardiovascular monitoring is already critical. — Goodman & Gilman's, p. 600; Katzung's, p. 1031
6. Drug Interactions Relevant to Inflammatory Settings
- Azathioprine / mercaptopurine: Febuxostat is contraindicated with these agents (XO inhibition raises plasma levels of XO-metabolized immunosuppressants to toxic levels) — relevant when treating inflammatory conditions with these drugs.
- Theophylline: Febuxostat inhibits XO-catalyzed metabolism of 1-methylxanthine, elevating its urinary excretion, but does not significantly alter theophylline pharmacokinetics at 80 mg/day. — Goodman & Gilman's, p. 605
Summary Table
| Aspect | Key Points |
|---|---|
| Primary indication | Chronic hyperuricemia in gout |
| Mechanism in edema | XO inhibition → ↓ uric acid → ↓ crystal-induced inflammation; ↓ ROS → ↓ endothelial permeability |
| Clinical edema relevance | Reduces recurrent gouty inflammatory edema; paradoxical flares at initiation |
| Advantage over allopurinol | Safe in moderate CKD; inhibits both XO redox states; alternative in allopurinol-intolerant patients |
| Key caution | Cardiovascular risk (boxed warning); contraindicated with azathioprine/mercaptopurine |
| Prophylaxis at initiation | Colchicine or NSAID to suppress early mobilization-related edema flares |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic and Clinical Pharmacology 16th Ed., Lippincott Illustrated Reviews Pharmacology, Brenner and Rector's The Kidney, Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.