Impulse oscillometry Full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Searching the Web
impulse oscillometry IOS clinical applications interpretation respiratory medicine MD exam
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
"impulse oscillometry" AND "respiratory" AND "clinical"
Reading File
Loading Image
I now have all the content needed for a comprehensive 15-mark answer. Let me compile it.
Impulse Oscillometry (IOS) - Comprehensive MD Exam Answer (15 Marks)
1. Definition and Principle (2 marks)
Impulse oscillometry (IOS) is a variant of the Forced Oscillation Technique (FOT) used to assess the mechanical properties of the respiratory system. It is a non-invasive, effort-independent test that superimposes external pressure oscillations onto a patient's normal quiet tidal breathing - no forced maneuvers are required.
The underlying principle is measurement of respiratory impedance (Zrs), which is the total opposition to airflow. A loudspeaker mounted at the mouthpiece delivers a composite pressure pulse (square wave impulse) to the airway opening. This impulse contains multiple frequency components simultaneously (typically 5-35 Hz). The ratio of pressure (Pmo) to airflow (Vmo) at the mouth, after Fourier analysis, resolves impedance into two components:
- Resistance (Rrs) - the in-phase component (energy dissipation)
- Reactance (Xrs) - the out-of-phase component (energy storage)
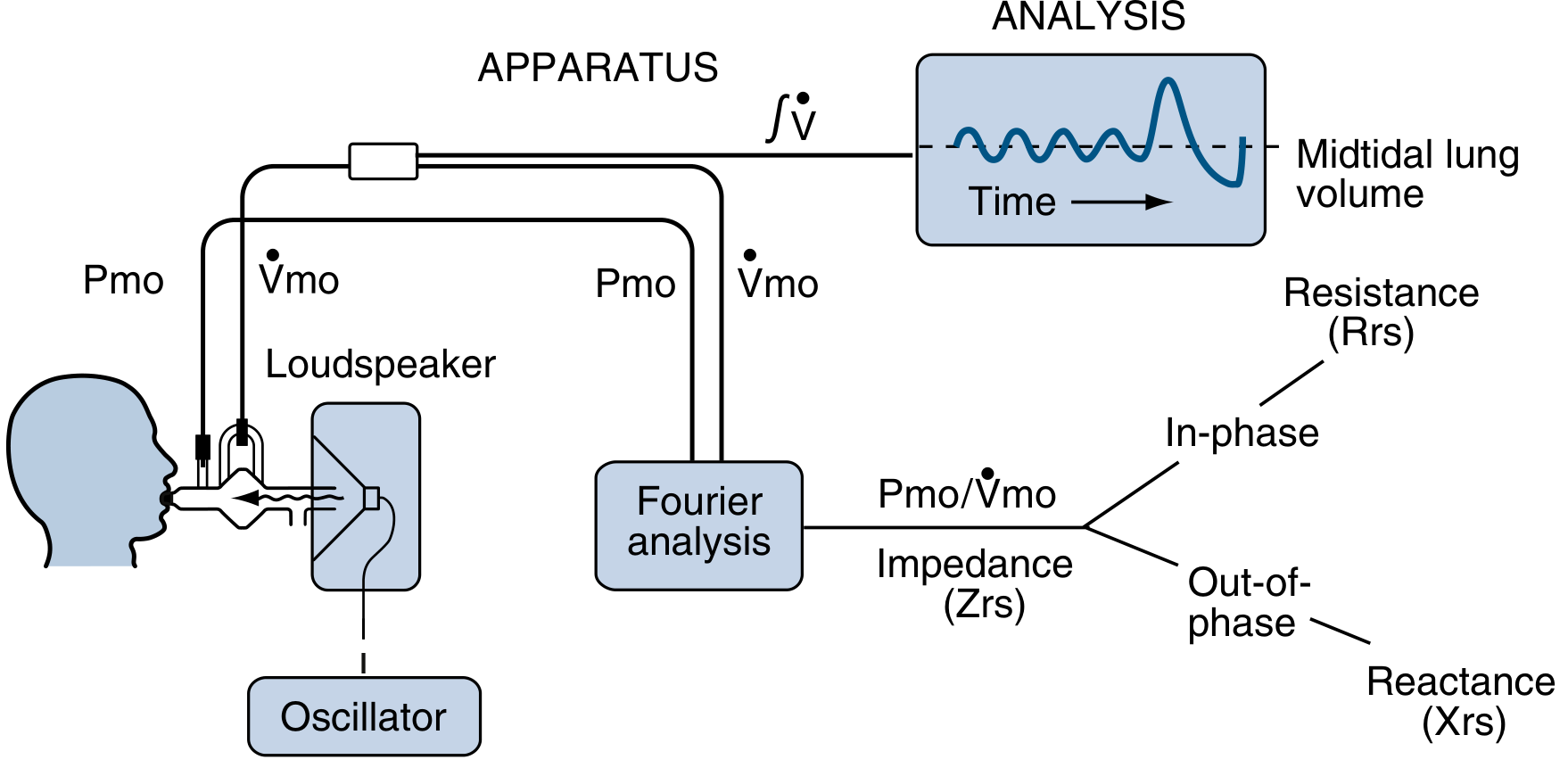
2. Key Parameters Measured (3 marks)
| Parameter | Frequency | What It Represents |
|---|---|---|
| R5 | 5 Hz | Total airway resistance (large + small airways) |
| R20 | 20 Hz | Large (proximal) airway resistance only |
| R5 - R20 | - | Small airway resistance (peripheral resistance) |
| X5 | 5 Hz | Reactance - elastic recoil and compliance of peripheral airways |
| AX | - | Reactance area - integral of reactance between 5 Hz and resonant frequency; marker of small airways disease |
| Fres | - | Resonant frequency - frequency at which reactance = 0; elevated in obstruction |
Physical basis of frequency separation:
- Low-frequency oscillations (5 Hz) travel all the way to the peripheral, small airways (< 2 mm diameter)
- High-frequency oscillations (20 Hz) penetrate only to the proximal, large airways
- This allows anatomic localization of disease within the airway tree
In normal subjects, respiratory resistance is frequency-independent over 5-25 Hz. In airway obstruction, resistance becomes frequency-dependent - R5 rises more than R20, producing a characteristic frequency dependence of resistance (FDR), expressed as R5 - R20.
3. Technique / Procedure (1 mark)
- Patient seated upright, nose clip applied
- Patient breathes normally and quietly at tidal volume through the mouthpiece - no forced effort needed
- Cheeks and floor of mouth supported by patient's hands (to minimize upper airway wall shunting)
- Oscillatory impulses delivered simultaneously at multiple frequencies from the loudspeaker
- Pressure and flow signals recorded at the mouth opening
- Fourier transform applied to extract resistance and reactance at each frequency
- Typically 30-45 seconds of recording; 3 acceptable measurements averaged
- Can be performed before and after bronchodilator to assess reversibility
Acceptability criteria: Absence of leaks, regular tidal breathing, no swallowing or vocalization, coherence value > 0.9.
4. Interpretation of Results (2 marks)
Normal pattern:
- R5 ≈ R20 (flat resistance vs. frequency - frequency independent)
- X5 close to zero or slightly negative
- Low Fres (typically < 10 Hz in adults)
Obstructive disease (e.g., asthma, COPD):
- R5 elevated, R5 > R20 - frequency dependence of resistance (FDR)
- R5 - R20 increased - indicates small airways involvement
- X5 more negative (increased magnitude) - reduced peripheral compliance
- Fres elevated - resonant frequency shifts up
- AX increased
Pattern differences by disease type:
| Finding | Asthma | COPD/Emphysema | Restrictive |
|---|---|---|---|
| R5 | Elevated | Elevated | Elevated |
| R5 - R20 | Elevated (small airway) | Elevated | Normal/mildly elevated |
| X5 | More negative | More negative | Less negative (stiffer) |
| Bronchodilator response | R5 ↓ ≥ 40%, X5 ↓ ≥ 50% | Partial | Absent |
Bronchodilator response thresholds:
- A decrease in R5 by 30-35% in children is considered a positive bronchodilator response (Murray & Nadel)
- A 50% decrease in X5 is roughly equivalent to a 20% decrease in FEV1 in children
5. Advantages Over Spirometry (2 marks)
| Feature | IOS | Spirometry |
|---|---|---|
| Patient effort required | None - tidal breathing only | Maximal forced effort |
| Age suitability | Works in children ≥ 2 years | Difficult < 5-6 years |
| Detects small airways disease | Yes - R5-R20, X5, AX directly measure it | Only indirectly (FEF25-75) |
| Effort-independent | Yes | No |
| Sensitivity for early airway disease | Higher (detects abnormality with normal spirometry) | Lower |
| Localization of disease | Yes (central vs. peripheral) | No |
| Duration | 30-45 seconds | Several minutes |
A key advantage: IOS can detect peripheral airway dysfunction when spirometry is still normal. Abnormal R5-R20 or X5 may occur with a preserved FEV1/FVC, reflecting early small airways disease - the "silent zone" of the lung.
6. Clinical Applications (3 marks)
a) Asthma
- Diagnosis in children (especially < 5 years) where spirometry is not feasible
- IOS has outperformed spirometry in sensitivity and specificity for diagnosing asthma in young children compared to methacholine challenge
- Monitoring treatment response and bronchodilator reversibility
- Detecting small airways disease (R5-R20 elevated) even with normal FEV1
- During bronchoprovocation testing - IOS changes correlate well with FEV1 changes
b) COPD
- Early detection of peripheral airway involvement before spirometric abnormality
- IOS parameters (particularly R5-R20 and X5) correlate with CT evidence of air trapping and emphysema
- 2025 systematic review (PMID 39362193) confirms IOS parameters are elevated in COPD vs. controls
c) Non-CF Bronchiectasis
- Elevated R5 and R5-R20, reduced X5 detected in active disease
- 2025 systematic review (PMID 40995772) confirms IOS utility
d) Interstitial Lung Disease (ILD)
- Distinct pattern: X5 less negative or near zero (stiff lungs have less elastic energy storage)
- Fres may be normal or low
e) Upper Airway Obstruction
- R5 and R20 both elevated equally (no frequency dependence), distinguishing from lower airway disease
- Useful in vocal cord dysfunction, tracheal stenosis
f) Obesity
- Detects expiratory flow limitation and small airways compression
- Changes in IOS with posture (supine) reflect lower zone airway closure
g) Patients unable to perform spirometry
- Neuromuscular disease, post-surgical, very young or elderly, cognitive impairment
7. Limitations (1 mark)
- Upper airway artifact - shunting through cheeks and pharynx can falsely lower measured resistance (mitigated by cheek support)
- Leaks around the mouthpiece invalidate the test
- Variable coherence with noisy breathing or secretions
- Lack of standardized reference equations for all ethnic populations; Oostveen (2013) equations validated for White adults
- Less established than spirometry in international guidelines (though ERS Technical Standards 2020 now provide guidance)
- Interpretation requires experience; less widely known than spirometry
- Cannot replace spirometry for standard lung function classification (obstruction grading, GOLD staging)
8. Comparison with Other Tests of Small Airways (1 mark)
| Test | Method | Comments |
|---|---|---|
| IOS (R5-R20, X5, AX) | Tidal breathing oscillometry | Effort-independent, most practical |
| FEF25-75 | Spirometry | Effort-dependent, high variability |
| Frequency dependence of compliance | Esophageal balloon | Invasive, research tool |
| Nitrogen washout (closing volume) | Single/multiple breath | Sensitive but technically demanding |
| CT air trapping | Imaging | Anatomic, no functional info |
Summary Table (Quick Revision)
| Feature | Detail |
|---|---|
| Principle | Loudspeaker delivers pressure impulse during tidal breathing; Fourier analysis extracts Rrs and Xrs |
| Key output | R5 (total R), R20 (central R), R5-R20 (peripheral R), X5 (reactance), AX, Fres |
| Normal | Frequency-independent resistance; X5 near zero |
| Obstruction | R5 > R20; frequency-dependent resistance; X5 more negative; Fres ↑ |
| Bronchodilator response | R5 ↓ ≥30-35% or X5 ↓ ≥50% |
| Best for | Children, small airways disease, effort-independent assessment |
| Advantage | Detects early/small airways disease before spirometry becomes abnormal |
References:
- Fishman's Pulmonary Diseases and Disorders (Section: Forced Oscillation Technique and Impulse Oscillometry, block 7)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapters 31, 32: Provocative Challenges, Respiratory Mechanics)
- Peng J et al. Clinical Value of Impulse Oscillometry in COPD: A Systematic Review and Meta-Analysis. Respiration, 2025 [PMID: 39362193]
- Andrade F et al. Impulse oscillometry in non-CF bronchiectasis: A systematic review. Pulmonology, 2025 [PMID: 40995772]
- King GG et al. Technical standards for respiratory oscillometry. Eur Respir J. 2020
This is a shared conversation. Sign in to Orris to start your own chat.