All i need to know about Rheumatoid arthritis us,
All about Rheumatoid arthritis with usmle high yield pearls. Add buzzwords lists in last
"rheumatoid arthritis"[MeSH Terms] AND treatment
rheumatoid arthritis USMLE high yield 2024 2025 pathophysiology diagnosis treatment
Rheumatoid Arthritis (RA) - Complete USMLE Guide
1. Epidemiology
- Prevalence: ~1% of adults worldwide; women:men ratio is 2-3:1
- Peak onset: 4th-6th decade, but can occur at any age
- HLA association: HLA-DR4 (and HLA-DR1) - the "shared epitope" on HLA-DRB1 is the strongest genetic risk factor
- Smoking is the major environmental risk factor (triggers citrullination of proteins, generating autoantigens)
- Associated with increased cardiovascular mortality (leading cause of excess death in RA)
2. Pathophysiology
- Trigger: Environmental exposures (especially cigarette smoke) induce citrullination of proteins in susceptible individuals (HLA-DR4 shared epitope)
- Autoantibodies generated: Anti-citrullinated protein antibodies (ACPA/anti-CCP) and Rheumatoid Factor (RF = IgM against IgG Fc)
- Immune cascade:
- APCs activate CD4+ T helper cells (Th1, Th17) in the synovium
- T cells activate B cells → plasma cells → RF and ACPA production
- Macrophages release TNF-α, IL-1, IL-6 → drive synovial inflammation
- IL-17 from Th17 cells upregulates VEGF and MMPs → cartilage degradation
- RANKL (produced by T cells) → osteoclast activation → bone erosion
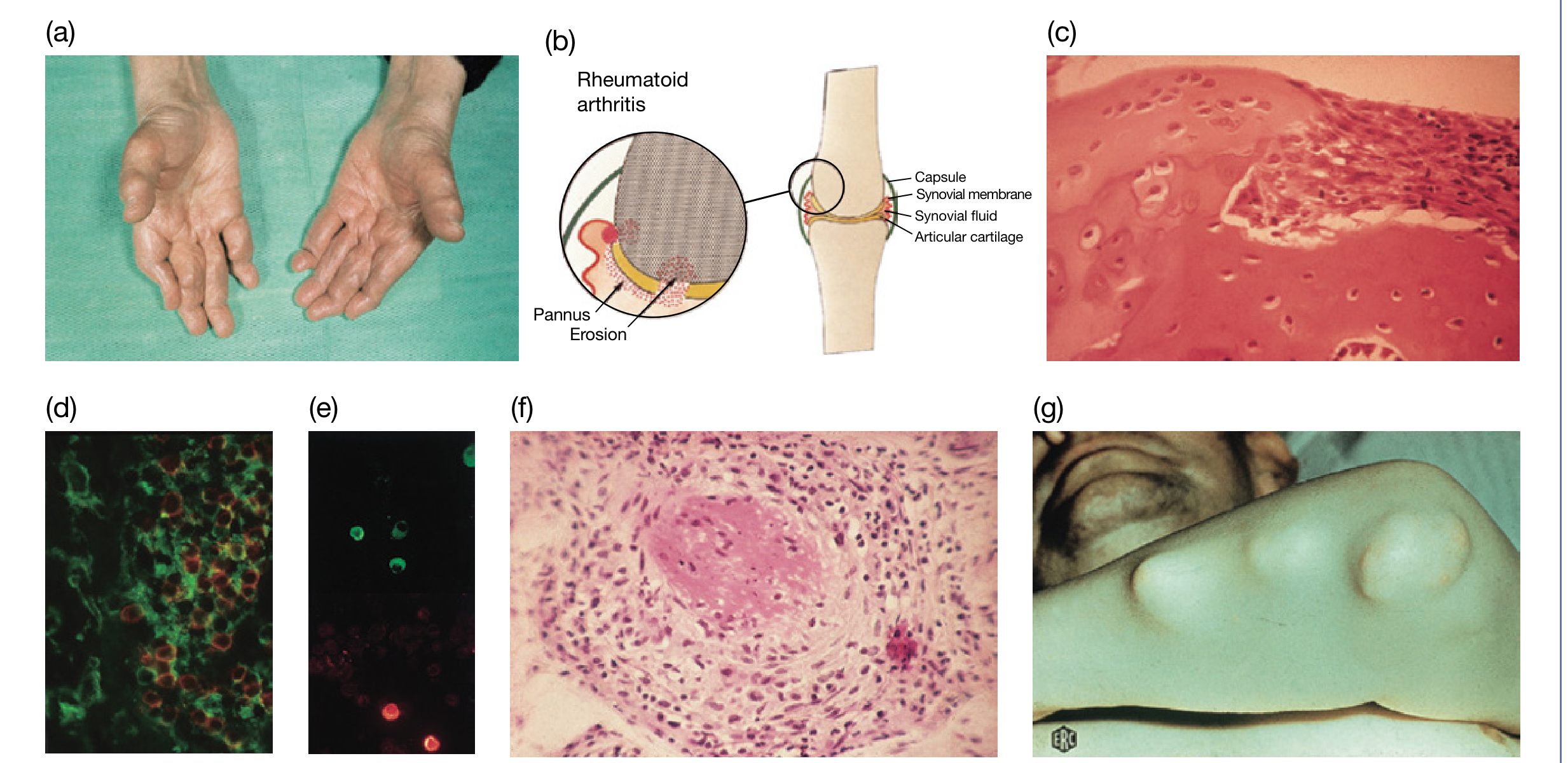
- Pannus: Proliferating synovial tissue (fibroblast-like synoviocytes) invades cartilage and bone → irreversible joint destruction
- Synovial fluid: Inflammatory - WBC 2,000-100,000 cells/μL (mostly PMNs), low glucose, low complement, elevated LDH
"In rheumatoid arthritis the chronically inflamed synovium is densely crowded with activated T-cells... High levels of IL-15 within the synovial membrane can recruit and activate T-cells whose secretion of cytokines and ability to induce macrophage synthesis of TNF contributes significantly to the disease." - Roitt's Essential Immunology
3. Clinical Features
Articular Manifestations
| Feature | Details |
|---|---|
| Joints affected | PIP, MCP, wrists, MTP (symmetric, bilateral) |
| Spared joints | DIP joints, thoracic/lumbar spine |
| Cervical spine | C1-C2 (atlantoaxial) involvement - risk of subluxation → myelopathy |
| Onset | Usually insidious, polyarticular |
| Morning stiffness | >1 hour (cardinal feature; differentiates from OA) |
| Synovitis | Boggy, warm, tender joints |
Classic Hand Deformities
- Ulnar deviation at MCPs (most common)
- Swan-neck deformity: PIP hyperextension + DIP flexion
- Boutonniere deformity: PIP flexion + DIP hyperextension
- Z-thumb: IP flexion + MCP hyperextension of thumb
- Hammer toe / Cock-up toes at MTPs
Baker Cyst
- Popliteal synovial cyst behind the knee
- Can rupture → calf pain mimicking DVT
Extra-Articular Manifestations (much more common in RF/ACPA-positive patients)
- Rheumatoid nodules (20% of patients) - subcutaneous, firm, non-tender, on extensor surfaces (olecranon), pressure points; histology shows palisading granuloma with central fibrinoid necrosis
- Small vessel vasculitis (brown infarcts of fingers/palms)
- Pleuritis/pleural effusion (exudate, low glucose, low complement)
- Caplan syndrome: RA + pneumoconiosis → large pulmonary nodules
- Interstitial lung disease (ILD) - particularly UIP pattern
- Bronchiolitis obliterans, pulmonary hypertension
- Pericarditis (most common cardiac manifestation)
- Myocarditis, coronary vasculitis
- Keratoconjunctivitis sicca (secondary Sjogren - most common eye finding)
- Scleritis (painful, red - indicates severe disease)
- Episcleritis (milder, self-limited)
- Scleromalacia perforans (painless scleral thinning → severe)
- Carpal tunnel syndrome (median nerve compression - most common peripheral nerve involvement)
- Tarsal tunnel syndrome (tibial nerve at ankle)
- Mononeuritis multiplex (from vasculitis)
- C1-C2 subluxation → cervical myelopathy
- Anemia of chronic disease (most common)
- Felty Syndrome: RA + splenomegaly + neutropenia (triad) - seen in severe, RF-positive, longstanding disease; risk of recurrent bacterial infections
- Fatigue, weight loss, low-grade fever, muscle wasting
- Increased risk of lymphoma (especially diffuse large B-cell lymphoma)
- Amyloidosis (AA type) in chronic untreated disease
4. Diagnosis
2010 ACR/EULAR Classification Criteria (Score ≥6 = RA)
| Domain | Score |
|---|---|
| A. Joint Involvement | |
| 1 large joint | 0 |
| 2-10 large joints | 1 |
| 1-3 small joints | 2 |
| 4-10 small joints | 3 |
| >10 joints (at least 1 small joint) | 5 |
| B. Serology (at least 1 test needed) | |
| Negative RF and negative ACPA | 0 |
| Low-positive RF or low-positive ACPA | 2 |
| High-positive RF or high-positive ACPA | 3 |
| C. Acute-Phase Reactants (at least 1 test needed) | |
| Normal CRP and normal ESR | 0 |
| Abnormal CRP or abnormal ESR | 1 |
| D. Duration of Symptoms | |
| <6 weeks | 0 |
| ≥6 weeks | 1 |
Laboratory Findings
| Test | Findings |
|---|---|
| Rheumatoid Factor (RF) | Positive in ~75%; IgM anti-IgG; not specific (also in SLE, Sjogren, bacterial endocarditis, normal elderly) |
| Anti-CCP (ACPA) | Positive in 60-70%; more specific than RF; positive years before clinical symptoms; predicts erosive/aggressive disease |
| CRP / ESR | Elevated (markers of inflammation, monitor disease activity) |
| CBC | Anemia of chronic disease; thrombocytosis (active disease); neutropenia (Felty) |
| ANA | Positive in ~30% (low titer, non-specific) |
| Synovial fluid | WBC 2,000-100,000; PMN predominant; low complement |
Imaging
| Modality | Findings |
|---|---|
| X-ray | Juxta-articular osteopenia (early) → joint space narrowing → bony erosions (marginal) → deformity (late) |
| MRI | Most sensitive for early synovitis, bone marrow edema, and erosions |
| Ultrasound | Detects synovitis and erosions; guides injections |
5. Treatment
Goals
- Remission (or lowest possible disease activity) - "treat-to-target" strategy
- Prevent joint damage and disability
- Treat comorbidities (CV risk, osteoporosis, infections)
Step-by-Step Treatment
Step 1: Conventional (Synthetic) DMARDs (csDMARDs)
| Drug | Notes |
|---|---|
| Methotrexate (MTX) | Anchor drug - first-line for most patients; folate supplementation required to reduce side effects (mucositis, cytopenias); monitor LFTs (hepatotoxicity); contraindicated in pregnancy; avoid alcohol |
| Hydroxychloroquine | Mild disease; requires annual ophthalmologic exam (bull's eye retinopathy) |
| Sulfasalazine | Moderate disease; can be combined with MTX + HCQ ("triple therapy") |
| Leflunomide | Alternative to MTX; teratogenic; long half-life (cholestyramine washout if needed) |
Step 2: Biologic DMARDs (bDMARDs) - if csDMARD fails
- Etanercept (soluble TNF receptor-Fc fusion)
- Infliximab, Adalimumab, Certolizumab, Golimumab (anti-TNF antibodies)
- Side effects: Increased risk of TB reactivation (screen with TST/IGRA before use), serious bacterial infections, demyelinating disease, drug-induced lupus (infliximab), CHF exacerbation
| Drug | Target | Notes |
|---|---|---|
| Abatacept | CD80/CD86 (blocks T cell costimulation) | Good in ACPA-positive patients |
| Rituximab | CD20 (B cell depletion) | Good after TNF failure; avoid in active infection; hepatitis B reactivation risk |
| Tocilizumab | IL-6 receptor | Raises cholesterol; masks fever (danger in infection screening) |
| Anakinra | IL-1 receptor | Less used due to injection-site reactions |
Step 3: Targeted Synthetic DMARDs (tsDMARDs) - JAK Inhibitors
| Drug | Dose | Notes |
|---|---|---|
| Tofacitinib | 5 mg BID | Risk: infections (TB, herpes zoster reactivation), malignancy, CV events |
| Baricitinib | Once daily | Better than adalimumab in MTX-inadequate responders |
| Upadacitinib | 15 mg daily | Selective JAK1 inhibitor |
| Filgotinib | 100-200 mg daily |
Glucocorticoids
- Prednisone ≤10 mg/day as bridge therapy while DMARDs take effect (slow onset)
- Rapidly effective but chronic toxicity is extensive (infection risk increases 25-100% at 5-10 mg/day)
- Intra-articular injections useful for flares
- Never use steroids alone without a DMARD
NSAIDs
- Symptomatic relief only - do NOT alter disease course
- Always combine with a DMARD
- COX-2 inhibitors: less GI toxicity but CV risk (especially relevant in RA patients already at high CV risk)
6. Monitoring Disease Activity
- DAS28 (Disease Activity Score with 28 joints) - includes tender/swollen joint counts, ESR or CRP, patient global assessment
- CDAI, SDAI, ACR20/50/70 response criteria (used in clinical trials)
7. Complications & Comorbidities
| Complication | Key Points |
|---|---|
| Cardiovascular disease | #1 cause of excess mortality in RA; treat aggressively; MTX + TNF inhibitors reduce CV mortality |
| Osteoporosis | Common; treat early (calcium, vitamin D, bisphosphonates) |
| Infections | All DMARDs/biologics increase risk; pneumococcal + flu vaccines recommended |
| Lymphoma | Increased risk (especially DLBCL); related to chronic inflammation |
| ILD | Particularly with MTX (MTX pneumonitis) and progressive fibrosing ILD |
| Atlantoaxial subluxation | C1-C2 subluxation → cervical cord compression; flex/extension films needed before surgery/intubation |
8. Special Scenarios
Seronegative RA
- ~25% of RA patients are RF and ACPA negative
- Tend to have milder articular disease
- Less extra-articular manifestations
- Nodules in a seronegative patient → consider tophaceous gout or other diagnosis
Drug-Induced Lupus from RA Treatment
- Infliximab (anti-TNF) can cause drug-induced lupus (anti-histone antibodies positive)
Pregnancy
- RA often improves during pregnancy (due to immune tolerance shift)
- Usually flares postpartum
- Methotrexate and leflunomide are teratogenic - must stop before conception
- Hydroxychloroquine and sulfasalazine are relatively safe in pregnancy
Juvenile Idiopathic Arthritis (JIA)
- RF-positive polyarticular JIA = essentially juvenile RA
- ANA-positive girls with oligoarthritis → highest risk of uveitis (anterior; silent)
9. Differential Diagnosis
| Condition | Key Differentiator |
|---|---|
| Osteoarthritis | DIP involvement, Heberden nodes (DIP), Bouchard (PIP), morning stiffness <30 min, non-inflammatory fluid |
| SLE | Jaccoud arthropathy (non-erosive), positive ANA, dsDNA, multi-organ involvement, malar rash |
| Psoriatic arthritis | DIP involvement, "sausage digit" (dactylitis), nail pitting, skin plaques, asymmetric |
| Reactive arthritis (formerly Reiter) | Can't see, can't pee, can't climb a tree; HLA-B27, follows GI/GU infection |
| Septic arthritis | Monoarthritis, WBC >50,000 in joint, fever |
| Gout | First MTP (podagra), negatively birefringent crystals, tophus (vs nodules) |
| Viral arthritis (parvovirus B19, hepatitis B/C, rubella) | Self-limited (<2-3 weeks), RF can be transiently positive |
| Ankylosing Spondylitis | Axial > peripheral, sacroiliitis, HLA-B27, bamboo spine |
10. USMLE High-Yield Pearls
- RF is NOT specific - positive in SBE, Sjogren, SLE, chronic infections, normal elderly (5-10% of healthy adults)
- Anti-CCP is most specific test for RA (>95% specific); also predicts erosive disease and positive years before clinical onset
- Morning stiffness >1 hour = inflammatory arthritis (RA); <30 min = OA
- DIP joints SPARED in RA (involved in OA and psoriatic arthritis)
- Methotrexate = anchor drug for RA; must add folic acid to prevent toxicity
- Screen for latent TB before starting any biologic (especially TNF inhibitors)
- Cervical spine is the only axial spine involved in RA (C1-C2 atlantoaxial); rest of axial spine spared
- Felty syndrome = RA + splenomegaly + neutropenia (severe, seropositive, longstanding disease)
- Caplan syndrome = RA + occupational dust exposure + pulmonary nodules (coal workers' pneumoconiosis)
- Baker cyst rupture mimics DVT; synovial cyst in popliteal fossa
- Cardiac: pericarditis is most common cardiac manifestation
- Eye: keratoconjunctivitis sicca (secondary Sjogren) is most common; scleritis = severe disease
- Pleural effusion in RA = exudate with LOW glucose (characteristic), low complement
- Hydroxychloroquine causes bull's eye retinopathy → annual eye exam required
- Tocilizumab (IL-6R blocker) raises serum cholesterol and can mask fever
- JAK inhibitors (tofacitinib, baricitinib) increase risk of herpes zoster reactivation
- RA improves in pregnancy, flares postpartum
- Rheumatoid nodule histology = central fibrinoid necrosis surrounded by palisading histiocytes
- Amyloidosis (AA type) can complicate longstanding untreated RA (secondary amyloidosis)
- X-ray sequence: periarticular osteopenia → joint space narrowing → marginal erosions → deformity
11. USMLE Buzzword List
- Pannus formation
- Synovial hypertrophy
- Anti-CCP / ACPA (anti-citrullinated protein antibody)
- Rheumatoid factor (IgM anti-IgG Fc)
- HLA-DR4 / shared epitope
- TNF-α, IL-1, IL-6, IL-17, RANKL
- CD4+ T cells, Th1, Th17
- Symmetric polyarthritis
- PIP + MCP involvement (DIP spared)
- Morning stiffness >1 hour
- Ulnar deviation (MCPs)
- Swan-neck deformity (PIP hyperextension + DIP flexion)
- Boutonniere deformity (PIP flexion + DIP hyperextension)
- Z-thumb
- Baker cyst (popliteal)
- C1-C2 atlantoaxial subluxation
- Cricoarytenoid joint involvement → hoarseness/stridor
- Rheumatoid nodule (extensor surface, olecranon, palisading granuloma)
- Felty syndrome (RA + splenomegaly + neutropenia)
- Caplan syndrome (RA + pneumoconiosis + large lung nodules)
- Scleritis / scleromalacia perforans
- Keratoconjunctivitis sicca (secondary Sjogren)
- Carpal tunnel syndrome
- Mononeuritis multiplex
- Pericarditis
- Low glucose pleural effusion
- AA amyloidosis
- RF positive (not specific)
- Anti-CCP positive (highly specific; predicts erosive disease)
- Elevated ESR, CRP
- Anemia of chronic disease
- Synovial WBC 2,000-100,000 (PMN predominant)
- Low complement in synovial/pleural fluid
- Juxta-articular osteopenia (first X-ray sign)
- Marginal erosions (later X-ray sign)
- Joint space narrowing
- Methotrexate (anchor drug) + folic acid
- Hydroxychloroquine (bull's eye retinopathy)
- Sulfasalazine
- Leflunomide (teratogenic; cholestyramine washout)
- TNF inhibitors (TB screening mandatory)
- Abatacept (CTLA4-Ig; blocks T cell costimulation)
- Rituximab (anti-CD20)
- Tocilizumab (anti-IL-6R; raises cholesterol; masks fever)
- Tofacitinib / Baricitinib / Upadacitinib (JAK inhibitors)
- Drug-induced lupus → infliximab
- Herpes zoster reactivation → JAK inhibitors
- Treat-to-target (goal = remission)
- RA vs OA: DIP spared in RA, involved in OA
- RA vs Psoriatic: RA symmetric, no DIP; Psoriatic asymmetric, DIP + dactylitis
- RA vs SLE: RA erosive; SLE non-erosive (Jaccoud)
- RA vs Septic: synovial WBC >50,000 + fever → septic
- RA vs Gout: negatively birefringent crystals in gout; tophi vs nodules
Generate a comparison poster: RA vs OA vs Psoriatic vs Viral Arthritis
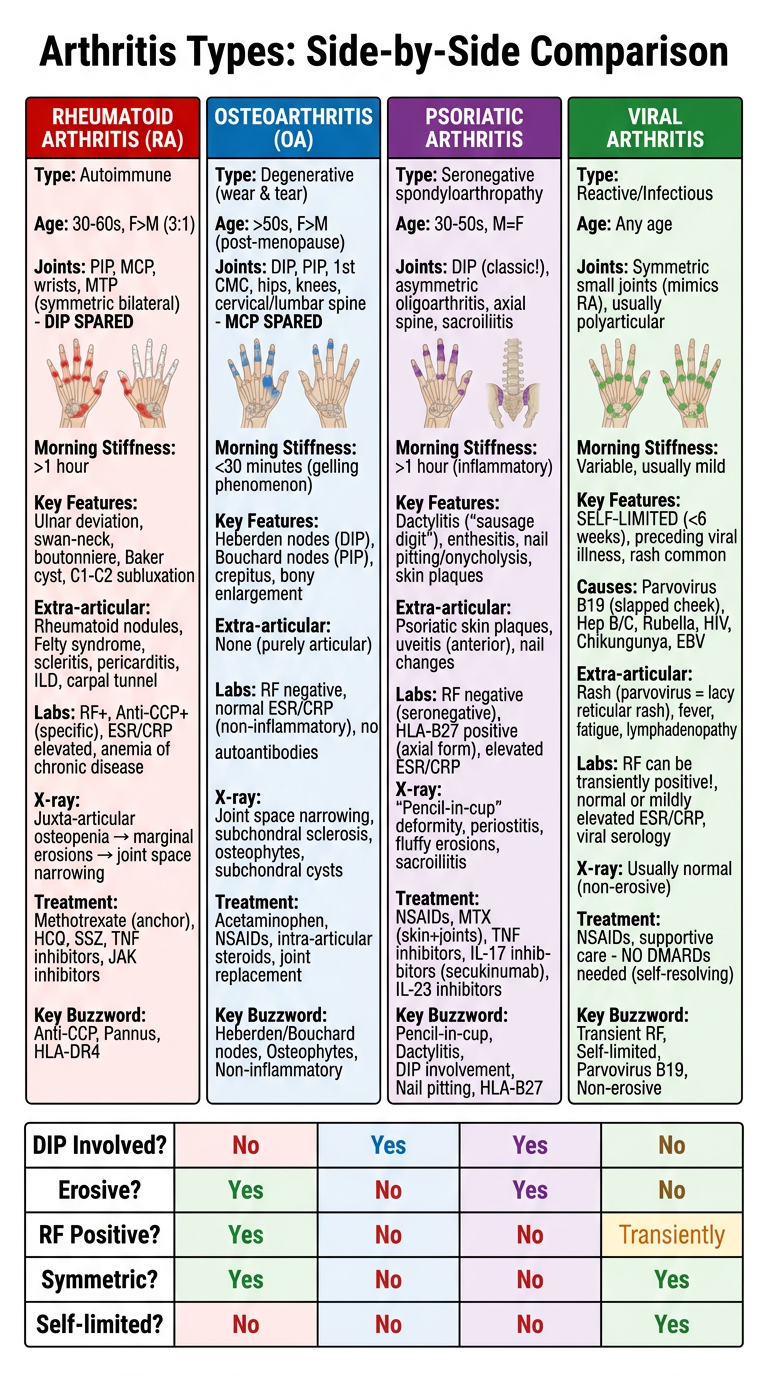
A detailed medical comparison poster titled "Arthritis Types: Side-by-Side Comparison" with 4 columns comparing Rheumatoid Arthritis (RA), Osteoarthritis (OA), Psoriatic Arthritis, and Viral Arthritis. Each column has a distinct color header (RA = red, OA = blue, Psoriatic = purple, Viral = green). The poster is clean, professional, clinical style on a white background. Each column contains the following rows with clear section labels and bullet points: RHEUMATOID ARTHRITIS (Red header): - Type: Autoimmune - Age: 30-60s, F>M (3:1) - Joints: PIP, MCP, wrists, MTP (symmetric bilateral) - DIP SPARED - Morning Stiffness: >1 hour - Key Features: Ulnar deviation, swan-neck, boutonniere, Baker cyst, C1-C2 subluxation - Extra-articular: Rheumatoid nodules, Felty syndrome, scleritis, pericarditis, ILD, carpal tunnel - Labs: RF+, Anti-CCP+ (specific), ESR/CRP elevated, anemia of chronic disease - X-ray: Juxta-articular osteopenia → marginal erosions → joint space narrowing - Treatment: Methotrexate (anchor), HCQ, SSZ, TNF inhibitors, JAK inhibitors - Key Buzzword: Anti-CCP, Pannus, HLA-DR4 OSTEOARTHRITIS (Blue header): - Type: Degenerative (wear & tear) - Age: >50s, F>M (post-menopause) - Joints: DIP, PIP, 1st CMC, hips, knees, cervical/lumbar spine - MCP SPARED - Morning Stiffness: <30 minutes (gelling phenomenon) - Key Features: Heberden nodes (DIP), Bouchard nodes (PIP), crepitus, bony enlargement - Extra-articular: None (purely articular) - Labs: RF negative, normal ESR/CRP (non-inflammatory), no autoantibodies - X-ray: Joint space narrowing, subchondral sclerosis, osteophytes, subchondral cysts - Treatment: Acetaminophen, NSAIDs, intra-articular steroids, joint replacement - Key Buzzword: Heberden/Bouchard nodes, Osteophytes, Non-inflammatory PSORIATIC ARTHRITIS (Purple header): - Type: Seronegative spondyloarthropathy - Age: 30-50s, M=F - Joints: DIP (classic!), asymmetric oligoarthritis, axial spine, sacroiliitis - Morning Stiffness: >1 hour (inflammatory) - Key Features: Dactylitis ("sausage digit"), enthesitis, nail pitting/onycholysis, skin plaques - Extra-articular: Psoriatic skin plaques, uveitis (anterior), nail changes - Labs: RF negative (seronegative), HLA-B27 positive (axial form), elevated ESR/CRP - X-ray: "Pencil-in-cup" deformity, periostitis, fluffy erosions, sacroiliitis - Treatment: NSAIDs, MTX (skin+joints), TNF inhibitors, IL-17 inhibitors (secukinumab), IL-23 inhibitors - Key Buzzword: Pencil-in-cup, Dactylitis, DIP involvement, Nail pitting, HLA-B27 VIRAL ARTHRITIS (Green header): - Type: Reactive/Infectious - Age: Any age - Joints: Symmetric small joints (mimics RA), usually polyarticular - Morning Stiffness: Variable, usually mild - Key Features: SELF-LIMITED (<6 weeks), preceding viral illness, rash common - Causes: Parvovirus B19 (slapped cheek), Hep B/C, Rubella, HIV, Chikungunya, EBV - Extra-articular: Rash (parvovirus = lacy reticular rash), fever, fatigue, lymphadenopathy - Labs: RF can be transiently positive!, normal or mildly elevated ESR/CRP, viral serology - X-ray: Usually normal (non-erosive) - Treatment: NSAIDs, supportive care - NO DMARDs needed (self-resolving) - Key Buzzword: Transient RF, Self-limited, Parvovirus B19, Non-erosive Bottom of poster includes a bold comparison summary table with rows: "DIP Involved?", "Erosive?", "RF Positive?", "Symmetric?", "Self-limited?" with Yes/No answers for each arthritis type in matching column colors. The poster uses a clean sans-serif font, has clear dividing lines between rows and columns, uses medical illustration style, and includes small anatomical hand diagrams showing which joints are affected for each type.
| Feature | RA | OA | Psoriatic | Viral |
|---|---|---|---|---|
| DIP involved? | No | Yes | Yes (classic) | Variable |
| Erosive? | Yes | No | Yes (pencil-in-cup) | No |
| RF positive? | Yes (~75%) | No | No (seronegative) | Transiently |
| Symmetric? | Yes | Variable | Asymmetric (often) | Yes |
| Self-limited? | No | No | No | Yes (<6 weeks) |
| Morning stiffness | >1 hr | <30 min | >1 hr | Variable |
| Key marker | Anti-CCP | Osteophytes | Dactylitis/nail pitting | Viral serology |
- RF can be positive in viral arthritis (transiently) - don't jump to RA if the illness is acute and <6 weeks
- DIP involvement rules out RA - if DIP is the dominant joint, think OA or psoriatic
- Psoriatic is seronegative (RF negative) despite being inflammatory and erosive - the "pencil-in-cup" X-ray and dactylitis are the distinguishing clues