Hordeolum management
Reading File
Finding Sources
Finding Sources
Searching Images
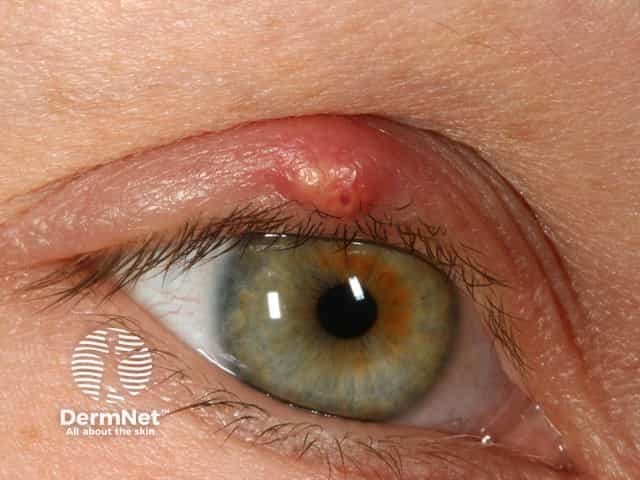
hordeolum stye eyelid
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Here is a synthesis:
Hordeolum (Stye) — Management
Definition & Classification
A hordeolum is an acute bacterial abscess of the eyelid glands, distinguished from a chalazion (lipogranulomatous, usually painless):
| Type | Gland involved | Location |
|---|---|---|
| External (stye) | Zeis or Moll gland | Eyelid margin, near lash follicle |
| Internal | Meibomian gland | Deep to conjunctival surface |
Pathogen: Almost always Staphylococcus aureus or other staphylococcal species. Frequently associated with acute blepharitis.
Natural history: Most drain spontaneously at 5–7 days with resolution of symptoms.
Medical Management (First-line)
-
Warm compresses — at least 10 minutes, 4× daily, with gentle massage over the lesion. This promotes pointing and spontaneous drainage.
-
Lid hygiene — lid scrubs at the base of eyelashes nightly using commercial ocular cleansing pads or half-strength baby shampoo on a cotton swab.
-
Topical antibiotics (for hordeolum specifically):
- Bacitracin, erythromycin, or tobramycin ointment b.i.d. for 1–2 weeks
- Fluoroquinolone drops (moxifloxacin or gatifloxacin) are an alternative
- Note: topical antibiotics have limited penetration into abscess cavities but treat surface colonization and associated blepharitis
-
Oral antibiotics — directed against Staphylococcus if there is significant surrounding cellulitis, failed topical therapy, or systemic signs. Examples: dicloxacillin, cephalexin; if MRSA suspected, trimethoprim-sulfamethoxazole or doxycycline.
-
Doxycycline (low-dose, 20–50 mg daily to b.i.d.) — useful for multiple or recurrent hordeola, particularly when associated with ocular rosacea; provides both antibacterial and anti-inflammatory effect.
Indications for Incision & Drainage (I&D)
- Failure of medical management
- Significant pain
- Visible, localized pus accumulation (pointing/fluctuant)
- Associated eyelid cellulitis (present or previous)
Contraindication: Lesion nasal to the medial canthus → refer to ophthalmology (risk of damaging lacrimal drainage system; also need to exclude dacryocystitis, which can spread to the cavernous sinus).
I&D Technique
- Topical ophthalmic anesthetic (e.g., tetracaine drops), then local infiltration with 2% lidocaine + epinephrine via 30-gauge needle.
- Insert a tongue blade or metal elevator behind the lid to protect the globe.
- Incise from the surface with best access to the pus (internal or external) using a no. 11 scalpel blade.
- Express contents, clean cavity with cotton swabs.
- Apply antibiotic ointment; patch is optional.
Patient counseling: risks include scarring, recurrence, short-term bruising/swelling, spread of infection, and (rarely) lacrimal damage.
Complications to Watch For
| Complication | Features | Action |
|---|---|---|
| Preseptal cellulitis | Spreading periorbital erythema, edema, warmth | Oral (or IV) antibiotics; urgent ophthalmology |
| Dacryocystitis | Swelling nasal to medial canthus | Ophthalmology referral |
| Orbital cellulitis | Proptosis, restricted/painful EOM, fever, toxaemia | Emergency ophthalmology/ENT |
| Recurrent/atypical lesion | Same location, elderly, madarosis | Biopsy to exclude sebaceous carcinoma |
Follow-Up
- Routine follow-up not needed if treating medically — unless lesion persists beyond 3–4 weeks.
- If I&D performed: reassess as needed.
- Recurrent chalazia/hordeola at the same site in older adults warrant histopathological examination to exclude malignancy.
Sources: Wills Eye Manual, 6.2; Pfenninger & Fowler's Procedures for Primary Care; Goldman-Cecil Medicine, Ch. 391
amoxiclav in Hordeolum management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have the full picture. Here is a focused answer:
Amoxicillin-Clavulanate (Amoxiclav) in Hordeolum Management
Short answer: Not a first-line drug for an uncomplicated hordeolum
Textbooks are consistent — the routine hordeolum is managed with warm compresses + topical antibiotics (erythromycin, bacitracin, or tobramycin ointment). Amoxicillin-clavulanate is not recommended for uncomplicated hordeolum because:
- Most hordeola are caused by Staphylococcus aureus, and the preferred oral agents are anti-staphylococcal penicillins (dicloxacillin, cephalexin) or topical preparations that target surface colonization.
- Amoxicillin-clavulanate's primary niche is in mixed infections with gram-negative and anaerobic organisms — not the typical staphylococcal lid abscess.
When amoxiclav is appropriate: Hordeolum complicated by preseptal cellulitis
A hordeolum is a known precipitant of preseptal cellulitis. When the infection spreads anterior to the orbital septum (spreading erythema, edema, warmth beyond the lid margin), oral antibiotics become necessary — and amoxicillin-clavulanate is an established first-line choice here:
| Setting | Amoxiclav dose | Duration |
|---|---|---|
| Adults (mild preseptal cellulitis, afebrile, reliable follow-up) | 875/125 mg p.o. q12h | 10–14 days |
| Children (>5 yrs, >40 kg, afebrile) | 25–45 mg/kg/day p.o. in 2 divided doses (max 90 mg/kg/day) | 10–14 days |
Goldman-Cecil gives the same regimen: amoxicillin-clavulanate 500 mg p.o. every 8 hours for 10 days as a commonly used option for preseptal cellulitis.
Why amoxiclav works in this context
The clavulanate component inhibits beta-lactamases produced by S. aureus and H. influenzae (relevant in unimmunized children), giving it broader coverage than amoxicillin alone. Its spectrum covers:
- Methicillin-sensitive S. aureus (MSSA)
- Streptococcal species
- H. influenzae (in children)
- Anaerobes (relevant if bite history or necrotic tissue)
It does NOT cover MRSA — if MRSA is suspected (see risk factors below), substitute or add TMP-SMX or clindamycin.
MRSA risk factors (switch to TMP-SMX or clindamycin instead)
- Prior MRSA infection/colonization
- Recurrent skin infections
- Healthcare facility admission within past year
- IV drug use, hemodialysis, or long-term indwelling catheter
- Close contact with known MRSA carrier
- Incarceration within past 12 months
Escalation criteria (admit for IV antibiotics)
- Moderate-to-severe preseptal cellulitis
- Toxic-appearing patient or high fever
- Child ≤5 years old
- Concern for orbital extension (proptosis, restricted EOM, pain on eye movement) → orbital cellulitis — ophthalmology emergency
Sources: Wills Eye Manual, §6.2 & §6.10; Goldman-Cecil Medicine, Ch. 391
This is a shared conversation. Sign in to Orris to start your own chat.