explain the menstrual cycle with hormonal changes and daigram ....answer this question in deatil . Which will be accepted by rhugs university... 10 marker according to indu khurahna ....with related daigram tooooo
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content and diagrams. Let me compose the detailed answer in the style Indu Khurana (textbook of physiology) presents it, suitable for a Rajasthan/Rhugs University 10-marker.
The Menstrual Cycle - Hormonal Changes
(10-Mark Answer | Indu Khurana Style | Rhugs University Standard)
DEFINITION
The menstrual cycle is a series of regular, cyclic changes occurring in the female reproductive organs (especially the ovary and uterus) that prepare the uterus for implantation of a fertilized ovum. If fertilization does not occur, the uterine lining is shed as menstruation.
- Duration: 28 days (average; varies from 21-35 days)
- Counted from Day 1 of menstruation to Day 1 of the next
- It begins at menarche (12-13 years) and ends at menopause (~45-50 years)
HORMONES INVOLVED
| Hormone | Source | Role |
|---|---|---|
| GnRH | Hypothalamus | Stimulates FSH & LH release |
| FSH | Anterior pituitary | Follicle development, estrogen production |
| LH | Anterior pituitary | Ovulation trigger, corpus luteum formation |
| Estrogen (Estradiol) | Granulosa cells of follicle | Endometrial proliferation, +ve feedback for LH surge |
| Progesterone | Corpus luteum | Secretory changes in endometrium, thermogenic |
| Inhibin B | Granulosa cells | Negative feedback on FSH |
PHASES OF THE MENSTRUAL CYCLE
The cycle has two major phases from the ovarian perspective, and three phases from the uterine perspective:
A. OVARIAN PHASES
1. FOLLICULAR PHASE (Day 1-14)
Hormonal Events:
- At the start of the cycle, FSH levels rise (due to reduced estrogen & progesterone from the previous corpus luteum - removal of negative feedback)
- FSH stimulates several primordial follicles to enlarge; one becomes the dominant (Graafian) follicle by Day 6
- The dominant follicle's granulosa cells secrete increasing amounts of estradiol (E2)
- The theca interna cells produce androgens, which are aromatized to estrogen by granulosa cells (two-cell theory)
- Rising estrogen initially exerts negative feedback on FSH (so FSH falls slightly after Day 7)
- Inhibin B (from granulosa cells) also suppresses FSH, helping ensure only one dominant follicle matures
- As estrogen climbs very high near Day 12-13, it switches to positive feedback on the anterior pituitary and hypothalamus
Key Result: A massive LH surge occurs at mid-cycle (Day 13-14), triggering ovulation ~9 hours after the LH peak
2. OVULATION (Day 14)
- Distended Graafian follicle ruptures
- Ovum is extruded into the peritoneal cavity and picked up by the fimbriae of the fallopian tube
- Minor bleeding from follicle rupture can cause mittelschmerz (midcycle pain)
- Basal body temperature (BBT) rises by ~0.5°C after ovulation (due to thermogenic effect of progesterone)
3. LUTEAL PHASE (Day 15-28)
Hormonal Events:
- After ovulation, the ruptured follicle fills with blood (corpus hemorrhagicum), then granulosa and theca cells proliferate under LH influence to form the corpus luteum (yellow, lipid-rich)
- Corpus luteum secretes progesterone (primarily) and estrogen
- Progesterone peaks around Day 21
- Both progesterone and estrogen exert negative feedback on FSH and LH, so pituitary gonadotropins fall
- The corpus luteum is maintained by LH; it has a fixed lifespan of ~14 days
- Without fertilization: corpus luteum degenerates into corpus albicans by Day 26-27; progesterone and estrogen fall sharply
- This hormonal withdrawal triggers menstruation
B. UTERINE (ENDOMETRIAL) PHASES
1. Menstrual Phase (Day 1-5)
- Withdrawal of estrogen + progesterone → vasospasm of spiral arteries (mediated by PGF2α)
- Endometrial necrosis and shedding
- Menstrual flow: ~30-80 mL; contains blood, endometrial debris, prostaglandins, fibrinolysin (prevents clotting)
- Only stratum basale remains; stratum functionale is shed
2. Proliferative Phase (Day 5-14) = Follicular phase
- Estrogen from developing follicle drives endometrial regeneration
- Endometrial thickness increases from 0.5 mm → 3.5 mm
- Endometrial glands elongate but do not secrete
- Cervical mucus becomes thin, watery, elastic (ferning pattern; spinnbarkeit)
- Spiral arteries elongate
3. Secretory Phase (Day 15-28) = Luteal phase
- Progesterone (+ estrogen) from corpus luteum acts on proliferated endometrium
- Uterine glands become tortuous and coiled, accumulate glycogen, increase secretions
- Stroma becomes edematous
- Spiral arteries become more coiled
- Cervical mucus becomes thick, viscid, non-ferning (blocks sperm - fertilization window has passed)
- If implantation occurs: hCG from trophoblast maintains corpus luteum
DIAGRAM 1: Ovarian and Uterine Events During the Menstrual Cycle
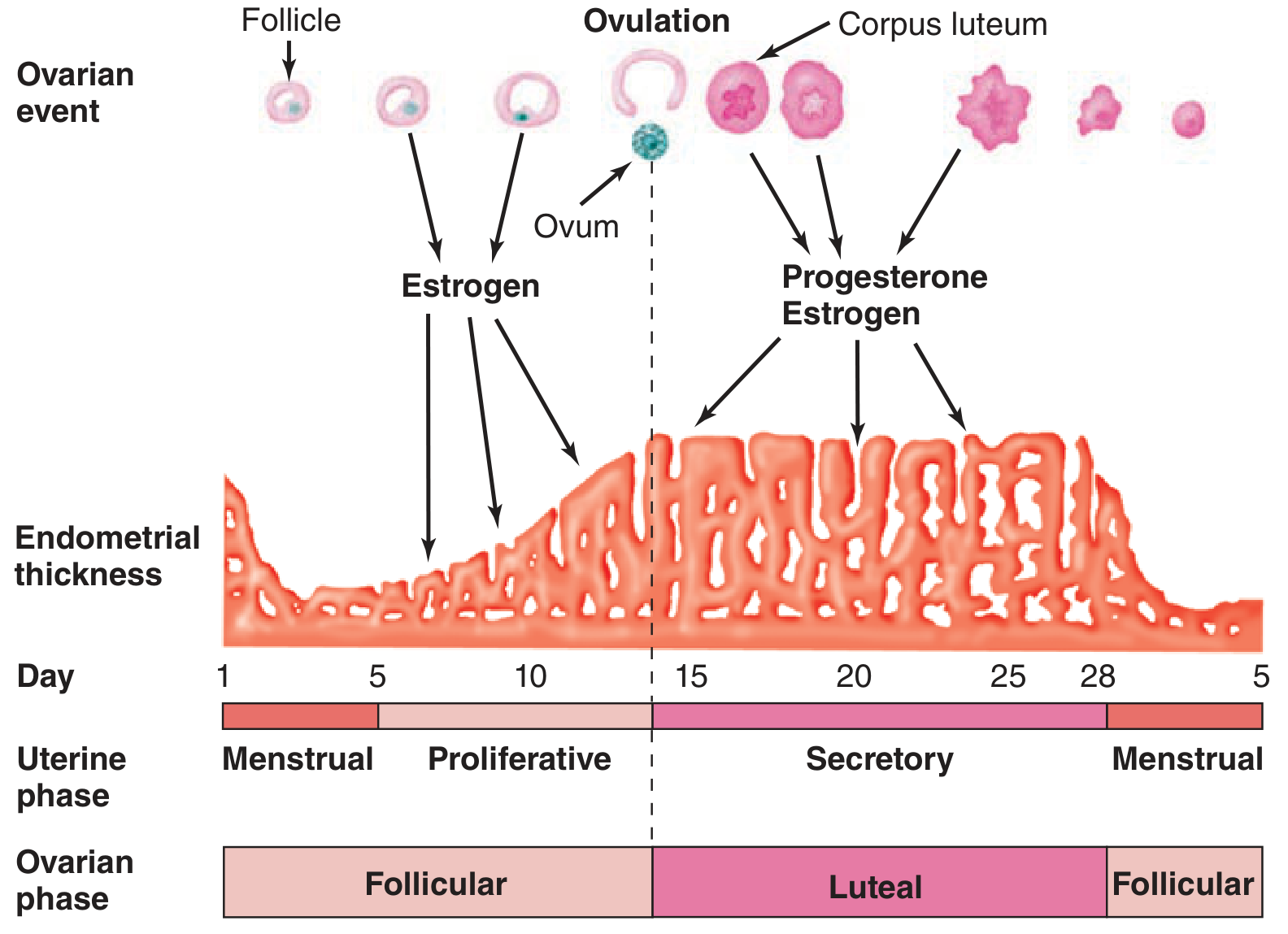
Fig: Relationship between ovarian events (follicle → ovulation → corpus luteum) and uterine endometrial changes across a 28-day cycle. Estrogen drives the proliferative phase; progesterone + estrogen drive the secretory phase. (Ganong's Review of Medical Physiology, 26th Ed.)
DIAGRAM 2: Hormonal Changes During the Menstrual Cycle
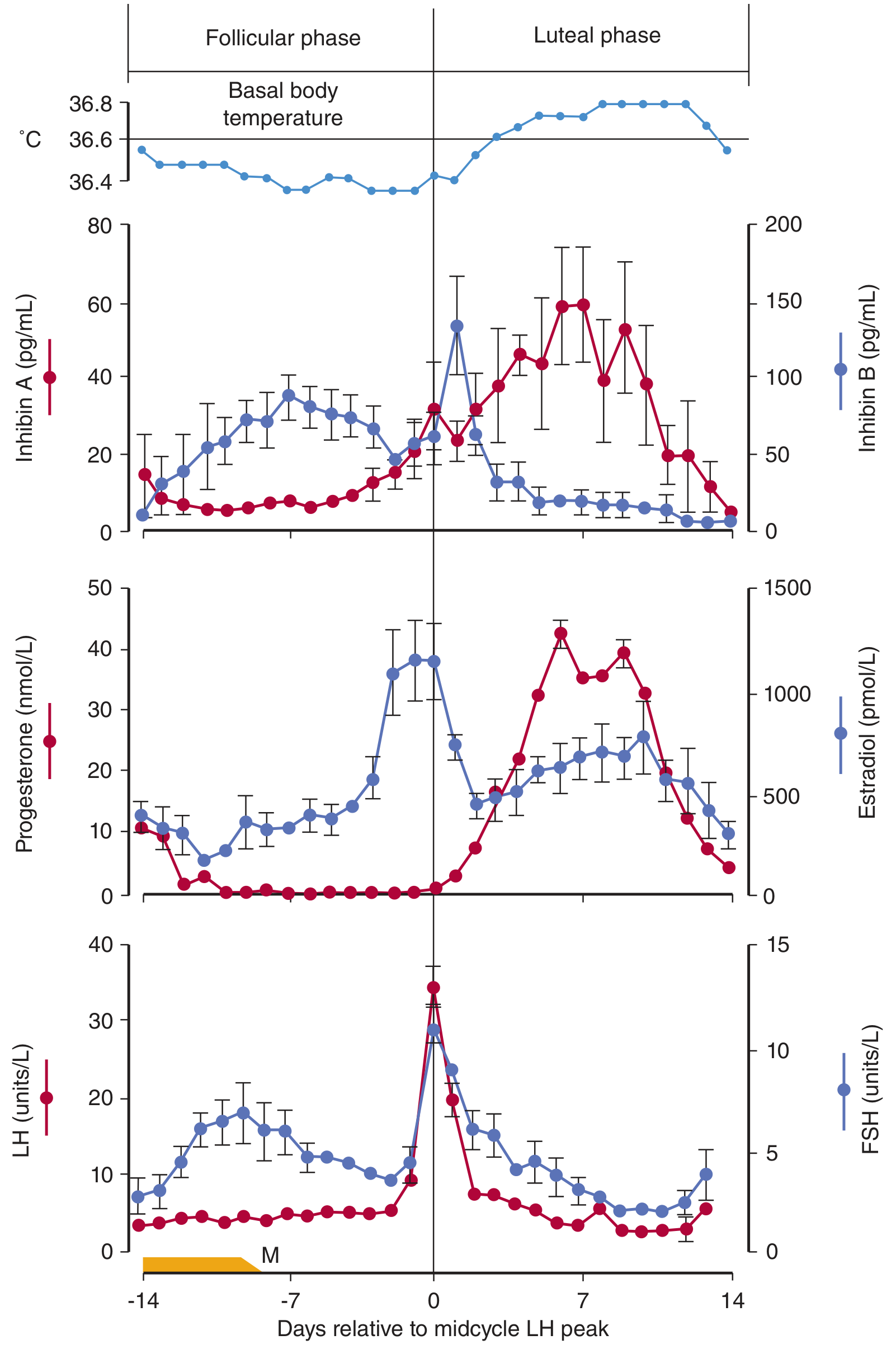
Fig: Basal body temperature and plasma hormone concentrations during the normal human menstrual cycle. Note: LH surge at Day 0 (midcycle), estradiol peak just before LH surge, progesterone peak in mid-luteal phase (~Day +7), FSH rise at start and small secondary peak at ovulation, BBT rise after ovulation. M = menses. (Ganong's Review of Medical Physiology, 26th Ed.)
SUMMARY TABLE: Hormonal Changes at a Glance
| Phase | Dominant Hormone | FSH | LH | Estrogen | Progesterone |
|---|---|---|---|---|---|
| Menstrual (Day 1-5) | None | Rising | Low | Low | Low |
| Proliferative (Day 5-13) | Estrogen | Falls gradually | Low | Rising | Low |
| Ovulation (Day 14) | LH surge | Small peak | Surge | Peak | Starting to rise |
| Secretory (Day 15-26) | Progesterone | Low | Low | Moderate | High (peaks Day 21) |
| Premenstrual (Day 27-28) | Falling | Starting to rise | Low | Falling | Falling |
KEY POINTS FOR EXAM (Important for 10-Marker)
- Positive feedback of estrogen triggers the LH surge - this is the key mechanism of ovulation
- Corpus luteum lifespan is ~14 days - explains the constant secretory phase (14 days) vs. variable follicular phase
- Progesterone is thermogenic - causes rise in BBT after ovulation (used in natural family planning)
- Prostaglandin PGF2α causes vasospasm of spiral arteries → menstruation
- Inhibin B (follicular phase) and Inhibin A (luteal phase) both suppress FSH
- Ferning of cervical mucus = estrogen effect (follicular phase); non-ferning = progesterone effect (luteal)
- Anovulatory cycles are common at menarche and premenopause - no corpus luteum formed, no progesterone, hence no secretory phase
- hCG from implanted embryo "rescues" the corpus luteum if fertilization occurs - prevents menstruation
Sources: Ganong's Review of Medical Physiology 26th Ed.; Costanzo Physiology 7th Ed.; Berek & Novak's Gynecology - all consistent with standard Indu Khurana physiology curriculum
This is a shared conversation. Sign in to Orris to start your own chat.