Staphylococcus infections
Reading File
Finding Sources
Searching PubMed
"Staphylococcus aureus"[MeSH Terms] AND "infection"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-cited answer. Here is the full response:
Staphylococcus Infections
Overview
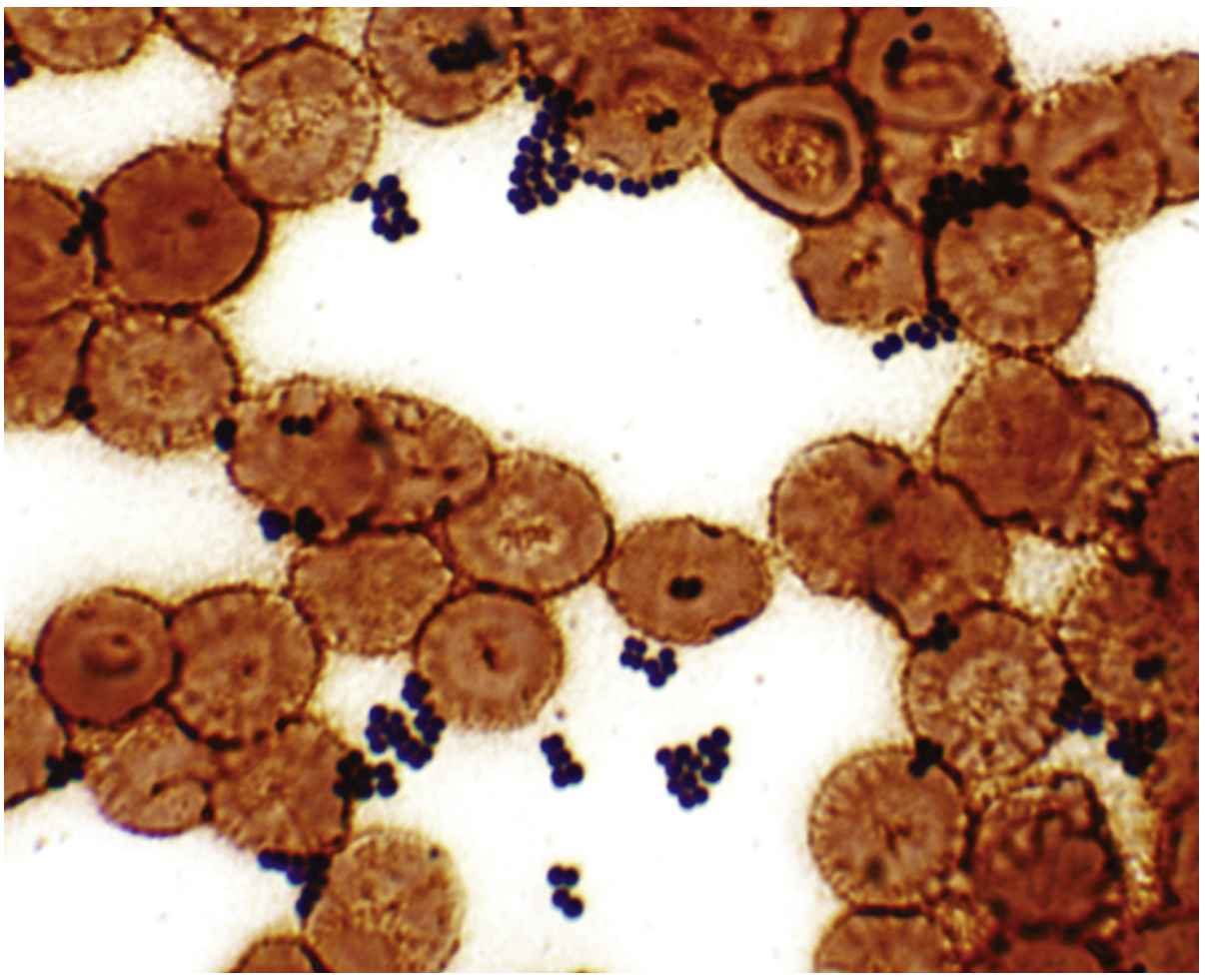
Staphylococci are catalase-positive, gram-positive cocci that grow in characteristic grape-like clusters (see image below). The genus comprises over 80 species, broadly divided into coagulase-positive (S. aureus) and coagulase-negative species (S. epidermidis, S. saprophyticus, etc.). They are facultative anaerobes tolerant of high salt concentrations, extremes of temperature, and dry surfaces - properties that make them resilient environmental and hospital pathogens.
Part 1: Staphylococcus aureus
Microbiology
- Gram-positive cocci in clusters, catalase-positive, coagulase-positive
- Identified by coagulase test, protein A presence, biochemical tests, molecular probes, or mass spectrometry (MALDI-TOF)
- Grows rapidly on non-selective media; selective media (mannitol-salt agar, chromogenic agar) used for contaminated specimens
- Nucleic acid amplification tests (NAATs) used for screening MSSA and MRSA carriage
Epidemiology
S. aureus colonizes the anterior nares, oropharynx, groin, perineum, and perianal area asymptomatically in a large proportion of the population. Infants become colonized from their mothers within weeks of birth. High-risk carriage groups include:
- Atopic dermatitis / eczema / chronic skin ulcers
- Insulin-dependent diabetes
- Patients on dialysis
- HIV infection
- Injection drug users
Transmission is primarily direct contact with infected individuals or asymptomatic carriers, likely via hand carriage. Environmental surface contamination can persist for days. Droplet/aerosol transmission is minimal. Carriers have a several-fold higher risk of developing active infection.
S. aureus causes millions of infections annually in the United States. About 5-10% of infections are invasive, three-fourths of which involve bacteremia. MRSA accounts for roughly half of healthcare-associated S. aureus infections in the US, and is now also prevalent in the community - though MRSA frequency and mortality have been declining in recent years.
- Goldman-Cecil Medicine, p. 3018-3020
Virulence Factors
S. aureus produces over 50 virulence factors encoded on the core chromosome, mobile genetic elements (bacteriophages, pathogenicity islands), and plasmids:
| Factor | Function |
|---|---|
| Coagulase | Converts fibrinogen to fibrin; defines the species |
| Protein A | Binds IgG Fc region; B-cell superantigen; blocks opsonization and antibody-mediated immunity |
| α-Toxin (alpha-hemolysin) | Pore-forming toxin; lyses host cells; drives inflammatory response |
| Panton-Valentine Leukocidin (PVL) | Destroys leukocytes; associated with community-MRSA skin abscesses and necrotizing pneumonia |
| Phenol-soluble modulins | Lyse cells; provoke inflammatory responses; important in CA-MRSA |
| Exfoliative toxins (ET-A, ET-B) | Serine proteases cleaving desmoglein-1; cause Staphylococcal Scalded Skin Syndrome (SSSS) |
| Toxic Shock Syndrome Toxin-1 (TSST-1) | Superantigen; causes massive cytokine release |
| Enterotoxins (A-E, G-J) | Heat-stable; cause food poisoning; act as superantigens |
| Adhesins (MSCRAMMs) | Bind fibronectin, fibrinogen, collagen; facilitate tissue adherence |
| Capsule polysaccharides | Inhibit phagocytosis |
| Hyaluronidase, lipase, protease | Facilitate tissue invasion and spread |
- Goldman-Cecil Medicine, p. 3018-3020; Medical Microbiology 9e
Diseases
S. aureus causes disease by two primary mechanisms: direct tissue invasion and toxin production.
A. Toxin-Mediated Diseases
1. Staphylococcal Food Poisoning
- Caused by heat-stable enterotoxins (resist boiling for 30 min)
- Incubation: 1-6 hours after ingestion of contaminated food
- Clinical: sudden onset severe nausea, vomiting, abdominal cramping, diarrhea
- Self-limiting; resolves within 24 hours
- Treatment is supportive (no antibiotics needed; the toxin is preformed)
2. Toxic Shock Syndrome (TSS)
- Caused by TSST-1 (or enterotoxins B, C in non-menstrual TSS)
- Superantigen activates up to 20% of T-cells simultaneously → massive cytokine storm
- Clinical triad: fever (>38.9°C), diffuse macular erythematous rash, hypotension (SBP <90 mmHg)
- Multi-system involvement: GI, muscular, renal, hepatic, hematologic, CNS
- Desquamation of palms and soles at 1-2 weeks
- Associated with tampon use (menstrual TSS), wound packing, nasal surgery
- Treatment: remove focus of infection + anti-staphylococcal antibiotics + supportive care (IVF, vasopressors); high mortality without prompt treatment
3. Staphylococcal Scalded Skin Syndrome (SSSS)
- Caused by exfoliative toxins (ET-A, ET-B)
- Predominantly in infants and young children (neonates most at risk - "Ritter disease")
- Superficial bullous desquamation - blisters contain NO organisms or leukocytes (toxin acts distally from the site of infection)
- Nikolsky sign positive
- Adults with renal failure at risk (toxins not cleared)
- Treatment: anti-staphylococcal antibiotics; wound care
B. Suppurative (Pyogenic) Infections
Skin and Soft Tissue (SSTI):
| Infection | Description |
|---|---|
| Impetigo | Superficial; pus-filled vesicles on erythematous base |
| Folliculitis | Impetigo involving hair follicles |
| Furuncle (boil) | Large painful pus-filled cutaneous nodule (single follicle) |
| Carbuncle | Coalescence of furuncles extending into subcutaneous tissue; systemic signs (fever, chills, bacteremia) |
| Cellulitis | Spreading infection of dermis and subcutaneous fat |
| Necrotizing fasciitis | Rapidly progressing fascial plane destruction; surgical emergency |
MRSA is now the most common cause of community-acquired skin and soft-tissue infections.
Pulmonary:
- Pneumonia: consolidation + abscess formation; seen in the very young, elderly, post-viral (influenza), or immunocompromised
- Necrotizing pneumonia with septic shock - a severe form associated with PVL-positive CA-MRSA strains; very high mortality
- Empyema
Cardiovascular:
- Bacteremia: S. aureus is a leading cause of bloodstream infection; major complication is seeding of distant sites
- Infective Endocarditis (IE): Acute presentation; damages valve endothelium; often requires surgical intervention; particularly common in IV drug users (right-sided, tricuspid valve)
Bone and Joint:
- Osteomyelitis: Destruction primarily at metaphysis of long bones; hematogenous in children, contiguous in adults
- Septic arthritis: Purulent joint effusion; most common causative organism in adults
CNS:
- Meningitis (associated with shunt infections)
- Brain abscess
Special Populations:
-
Foreign body infections: Even small inocula can establish infection with a prosthesis, catheter, or shunt (foreign body reduces the bacterial count needed to cause infection by 1,000-fold)
-
Immunocompromised: Patients with Job syndrome (hyper-IgE), Wiskott-Aldrich syndrome, or chronic granulomatous disease are specifically susceptible
-
Medical Microbiology 9e; Goldman-Cecil Medicine; Murray & Nadel's Textbook of Respiratory Medicine
Part 2: MRSA - Methicillin-Resistant S. aureus
Mechanism of Resistance
MRSA harbors the mecA gene (on the SCCmec mobile genetic element), which encodes a modified penicillin-binding protein PBP2a (also called PBP2'). PBP2a has very low affinity for all beta-lactam antibiotics, rendering the organism resistant to penicillins, anti-staphylococcal penicillins (oxacillin, nafcillin), and cephalosporins (with rare exceptions like ceftaroline).
Community-MRSA (CA-MRSA) vs. Healthcare-MRSA (HA-MRSA)
| Feature | CA-MRSA | HA-MRSA |
|---|---|---|
| SCCmec type | IV, V (smaller) | I, II, III (larger) |
| PVL | Often present | Usually absent |
| Common clone (USA) | USA300 | USA100 |
| Clinical syndromes | Skin abscesses, necrotizing pneumonia | BSI, pneumonia, wound infections |
| Antibiotic resistance | Narrower | Often multi-drug resistant |
| Circulation | Community + healthcare | Primarily healthcare |
- Goldman-Cecil Medicine, p. 3019-3020
Part 3: Coagulase-Negative Staphylococci (CoNS)
CoNS are normal skin and mucosal flora. They are relatively avirulent but important opportunistic pathogens in the presence of foreign bodies due to their ability to produce biofilm ("slime layer") - which:
- Allows adherence to prosthetic material
- Protects against phagocytosis
- Reduces antibiotic penetration
Key Species
| Species | Main Clinical Niche |
|---|---|
| S. epidermidis | Intravascular catheters, prosthetic valves/joints, CSF shunts, pacemakers |
| S. saprophyticus | Urinary tract infections in young sexually active women |
| S. lugdunensis | More virulent CoNS; can cause aggressive native valve endocarditis |
| S. haemolyticus | Nosocomial infections; often multi-drug resistant |
Infections
-
Subacute endocarditis (particularly on prosthetic valves - most common cause of early prosthetic valve endocarditis)
-
Catheter-related bloodstream infections
-
Prosthetic joint infections
-
CSF shunt infections
-
Urinary tract infections
-
Medical Microbiology 9e
Part 4: Diagnosis
| Test | Use |
|---|---|
| Gram stain | Useful for pyogenic infections; NOT reliable for bacteremia or toxin-mediated disease |
| Culture | Gold standard; grows rapidly on non-selective blood agar |
| Coagulase test | Distinguishes S. aureus (positive) from CoNS (negative) |
| Mannitol-salt / chromogenic agar | Selective for S. aureus in contaminated specimens |
| NAAT / PCR | Rapid screening for MRSA/MSSA colonization (e.g., nasal swabs) |
| MALDI-TOF mass spectrometry | Rapid species identification from culture |
| Susceptibility testing | MIC-based; essential for guiding therapy |
- Henry's Clinical Diagnosis and Management by Laboratory Methods; Medical Microbiology 9e
Part 5: Treatment
Antibiotic Therapy
MSSA (Methicillin-Susceptible S. aureus)
- Drug of choice: Nafcillin or oxacillin (2 g IV q4h) - beta-lactams are superior to vancomycin for MSSA; desensitization preferred when allergy is reported
- Alternative (penicillin allergy without anaphylaxis): Cefazolin (2 g IV q8h)
- For endocarditis: 6 weeks for native valve; right-sided IV drug user endocarditis may be treated with 2 weeks if no complications
MRSA
- IV drug of choice: Vancomycin (15 mg/kg IV q12h, targeting AUC/MIC ratio or trough 15-20 mcg/mL)
- Alternative IV: Daptomycin (≥8 mg/kg/day) - NOTE: do NOT use daptomycin for pulmonary infections (inactivated by surfactant); monitor CK
- Other IV alternatives: Linezolid, tigecycline
- Oral options: TMP-SMX, doxycycline/minocycline, clindamycin (check local resistance - up to 40% resistant), linezolid
- Vancomycin MIC creep: isolates with vancomycin MIC of 4-8 mcg/mL (hVISA/VISA) - 1-3% of MRSA - may fail vancomycin treatment; alternative agents needed
Prosthetic Valve Endocarditis (PVE) - Staphylococci
-
MSSA/MSSE: Oxacillin + rifampin (300 mg PO q8h) + gentamicin (first 2 weeks only) for ≥6 weeks
-
MRSA/MRSE: Vancomycin + rifampin + gentamicin (first 2 weeks) for ≥6 weeks
-
Rifampin improves biofilm penetration; gentamicin provides synergy in early weeks
-
Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22E; Medical Microbiology 9e
Non-Antibiotic Management
- Skin abscesses: Incision and drainage (I&D) is primary treatment; antibiotics added for spreading cellulitis, systemic signs, or immunocompromise
- Foreign body infections: Removal of the foreign body is often required for treatment success alongside antibiotics
- Blood cultures: Obtain daily until clearance of bacteremia is documented; persistent bacteremia (>3-4 days) requires evaluation for endocarditis, septic emboli, or metastatic foci
Monitoring
- Persistent or worsening bacteremia despite therapy should prompt repeat echocardiography and search for undrained foci
- Clinical improvement expected within 3-10 days of initiating therapy
- Monitor vancomycin levels (goal trough 15-20 mcg/mL or AUC-guided dosing)
- Monitor CK weekly in patients on daptomycin
Part 6: Prevention and Infection Control
- Hand hygiene: Thorough handwashing is the most effective prevention measure in healthcare settings
- Contact precautions: Gowns + gloves for MRSA-positive patients
- Decolonization: Mupirocin nasal ointment ± chlorhexidine bathing for high-risk patients (pre-operative, ICU, dialysis patients) reduces S. aureus infections
- Wound care: Proper cleansing and use of disinfectant
- Catheter bundles: Sterile technique, routine assessment of line necessity, chlorhexidine-impregnated dressings
Summary Table
| Feature | S. aureus (MSSA) | S. aureus (MRSA) | CoNS |
|---|---|---|---|
| Coagulase | + | + | - |
| Hallmark resistance | Penicillinase (plasmid) | mecA (PBP2a) | Variable |
| Key toxins | TSST-1, ET, enterotoxins, PVL | PVL (CA-MRSA) | Biofilm |
| Primary drug | Nafcillin/oxacillin | Vancomycin/daptomycin | Vancomycin |
| Key clinical niches | SSTI, bacteremia, endocarditis, pneumonia, osteomyelitis | SSTI, HA infections, necrotizing pneumonia | Prosthetics, catheters, UTI |
Sources: Medical Microbiology 9e | Goldman-Cecil Medicine | Washington Manual of Medical Therapeutics | Harrison's Principles of Internal Medicine 22E | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.