How to administer subcutaneous infusion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have enough information to provide a comprehensive answer. Here is a complete guide on administering subcutaneous infusion (hypodermoclysis):
Subcutaneous Infusion (Hypodermoclysis)
Subcutaneous infusion — also known as hypodermoclysis — delivers fluids (and some medications) into the subcutaneous tissue for systemic absorption via capillary beds. It is used when IV access is difficult or unavailable, and the patient cannot tolerate oral/nasogastric rehydration.
Indications
- Moderate dehydration when IV access is unobtainable
- Oral/nasogastric routes have failed or are not tolerated
- Common populations: elderly, paediatric patients (≥2 months), palliative/hospice patients
Contraindications
- Severe dehydration / hypovolemic shock (use IO or central venous access instead)
- Overlying cellulitis at the intended insertion site
- Gross oedema or significant electrolyte abnormalities (Na⁺ >150 or <130 mEq/L)
- Coagulation deficits
- Massive burns (no intact skin sites)
Equipment
- IV fluid bag + administration tubing with drip chamber
- Small-gauge butterfly needle (21-gauge or smaller) or 22–25-gauge angiocatheter
- Human recombinant hyaluronidase (HuPH20 / Hylenex) — 150 units
- 1% lidocaine (for local anaesthesia)
- Povidone-iodine or alcohol swabs
- Sterile occlusive dressing
- Gloves
Site Selection
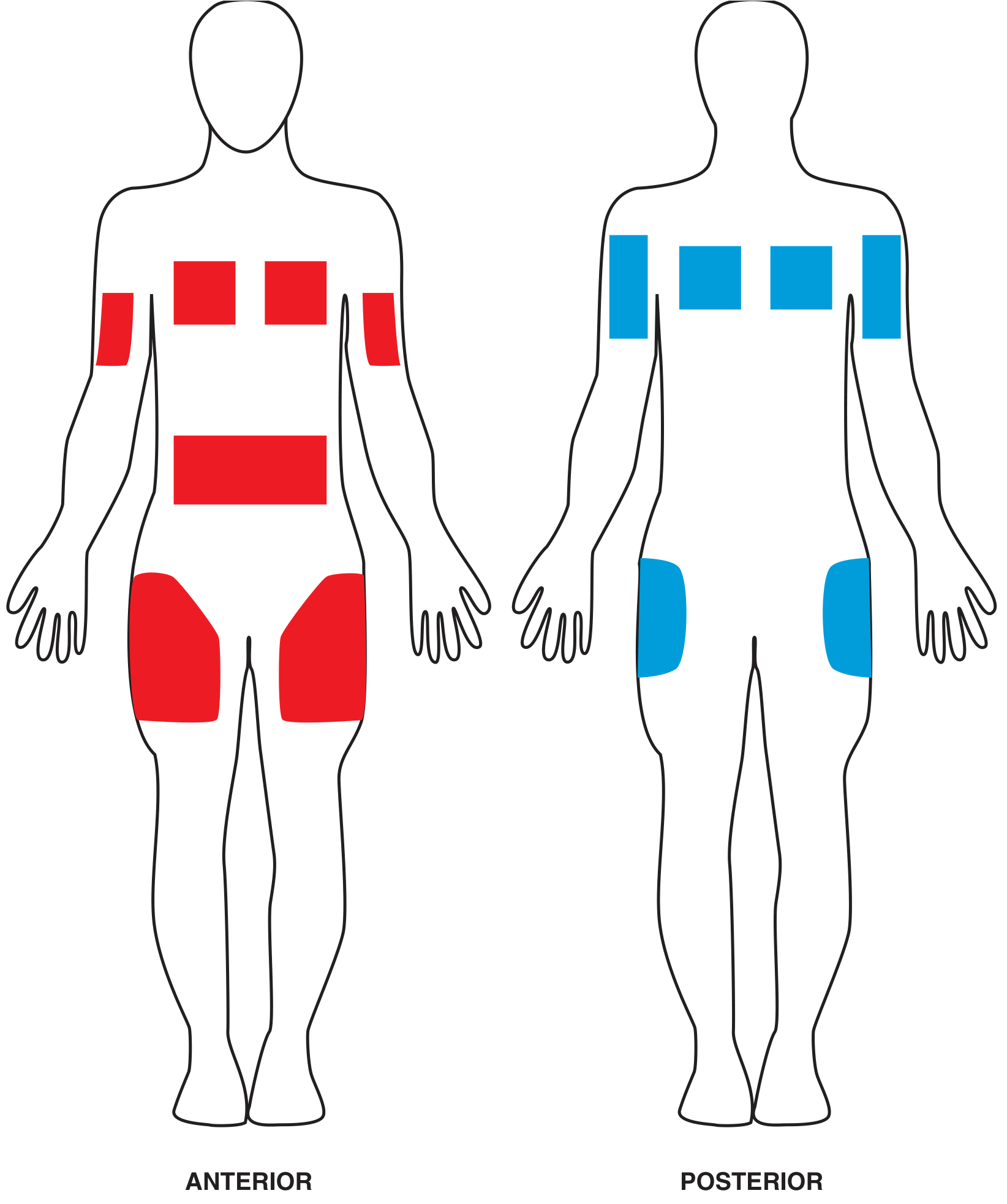
Anatomic sites for hypodermoclysis (anterior in red, posterior in blue). From Roberts and Hedges' Clinical Procedures in Emergency Medicine.
Suitable sites (choose one with at least 1 inch of pinchable fat):
| Site | Notes |
|---|---|
| Interscapular / intrascapular | Preferred in children or uncooperative patients — reduces dislodgement risk |
| Abdomen (left iliac fossa) | Commonly used in adults |
| Upper chest / above the breast | Over an intercostal space |
| Lateral thighs | Good fat fold in most patients |
| Outer upper arm | Accessible but less padding |
Step-by-Step Procedure
-
Prepare and prime the line — Assemble the IV bag, tubing, and add 150 units of hyaluronidase to the priming flush.
-
Skin preparation — Swab the chosen site with povidone-iodine or alcohol. Allow to dry.
-
Local anaesthesia — Inject a small amount of 1% lidocaine intradermally at the insertion point.
-
Insert the needle — Pinch the skin between two fingers. Insert the butterfly needle or angiocatheter bevel up at a 45–60° angle (30–45° for smaller angiocatheters in paediatrics) into the subcutaneous tissue.
-
Confirm placement — Aspirate to confirm absence of blood return (ensures you are not in a vessel).
-
Administer hyaluronidase — Inject 150 units of human recombinant hyaluronidase into the subcutaneous space through the catheter. This breaks down hyaluronan in the intercellular matrix, transiently increasing tissue permeability and allowing fluid to spread and absorb.
-
Secure the needle — Place a small gauze under the hub to maintain the angle, then cover with a sterile occlusive dressing.
-
Start the infusion — Connect the primed line and start the fluid. Isotonic fluids (0.9% NaCl) are standard. Fluids containing dextrose and potassium can also be given.
-
Titrate the rate:
- Allow ~15 minutes for hyaluronidase to take full effect — start slowly then titrate up
- Target ~20 mL/kg/hour in children (range: 18.9–38.4 mL/kg over 1–4 hours)
- If the infusion pump signals occlusion, reduce the rate by 10 mL/hour
What to Expect
- An erythematous swelling at the insertion site is normal in the first few minutes — it will reduce after ~5 minutes and resolve completely within 1–2 hours of stopping the infusion.
- Maximal diffusion into the IV compartment occurs within 1 hour.
- A single hyaluronidase dose remains effective for up to 48 hours, allowing maintenance fluids to continue.
Troubleshooting
| Problem | Action |
|---|---|
| Catheter dislodged | Restart in the same area — no additional hyaluronidase needed |
| Infusion pump occlusion | Reduce rate by 10 mL/hour |
| Site becomes firm, indurated, and painful | Administer an additional 150-unit dose of hyaluronidase |
| Child fails outpatient therapy | Continue infusion through the same catheter for up to 48 hours |
Complications
- Pain or swelling at the infusion site (common, usually self-limiting)
- Cellulitis at the insertion site (rare)
- Allergic reactions — not reported with recombinant hyaluronidase (HuPH20); were a concern with older animal-derived preparations
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapters 19 & 26
This is a shared conversation. Sign in to Orris to start your own chat.