Mechanism of secretion of gastric juice
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks along with key diagrams. Let me compile the full answer.
Mechanism of Secretion of Gastric Juice
Overview of Gastric Juice Composition
Gastric juice has four major components secreted by specialized cells in the gastric mucosa:
| Component | Secreting Cell | Location |
|---|---|---|
| HCl | Parietal (oxyntic) cells | Fundus/body (oxyntic glands) |
| Pepsinogen | Chief (peptic) cells | Fundus/body (oxyntic glands) |
| Intrinsic factor | Parietal cells | Fundus/body |
| Mucus + HCO3- | Mucous neck cells, surface epithelium | Throughout stomach |
| Gastrin | G cells | Antrum (pyloric glands) |
In the fasting state, the pH of gastric juice is approximately 3.0, and it contains Na+, K+, Mg2+, H+, Cl-, and HPO4 2-. When maximally stimulated, the H+ concentration reaches ~160 mmol/L with a pH of ~0.8 - approximately 3 million times the H+ concentration of arterial blood.
- Costanzo Physiology 7th Edition, p. 365; Ganong's Review of Medical Physiology, 26th Edition, p. 460
Structure of the Gastric (Oxyntic) Gland
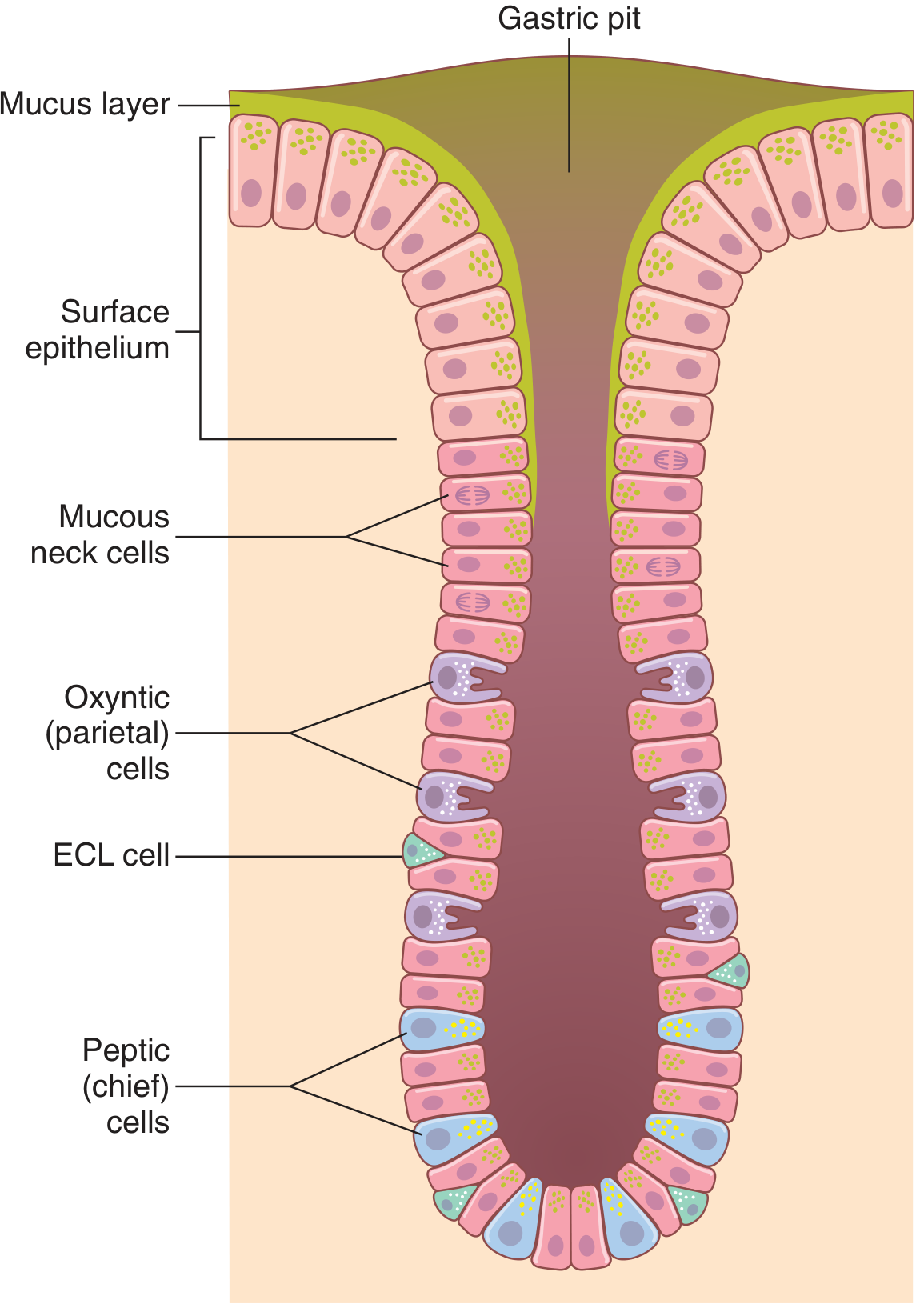
Gastric (oxyntic) gland - Guyton and Hall
The oxyntic glands occupy the fundus and body (proximal 80%). Each gland opens into a gastric pit and contains:
- Mucous neck cells - secrete mucus
- Parietal (oxyntic) cells - secrete HCl and intrinsic factor; contain large branching intracellular canaliculi
- Chief (peptic) cells - secrete pepsinogen
- ECL (enterochromaffin-like) cells - secrete histamine
1. Cellular Mechanism of HCl Secretion (Parietal Cells)
This is the most energy-intensive secretion in the body, requiring >1500 calories per liter of gastric juice.
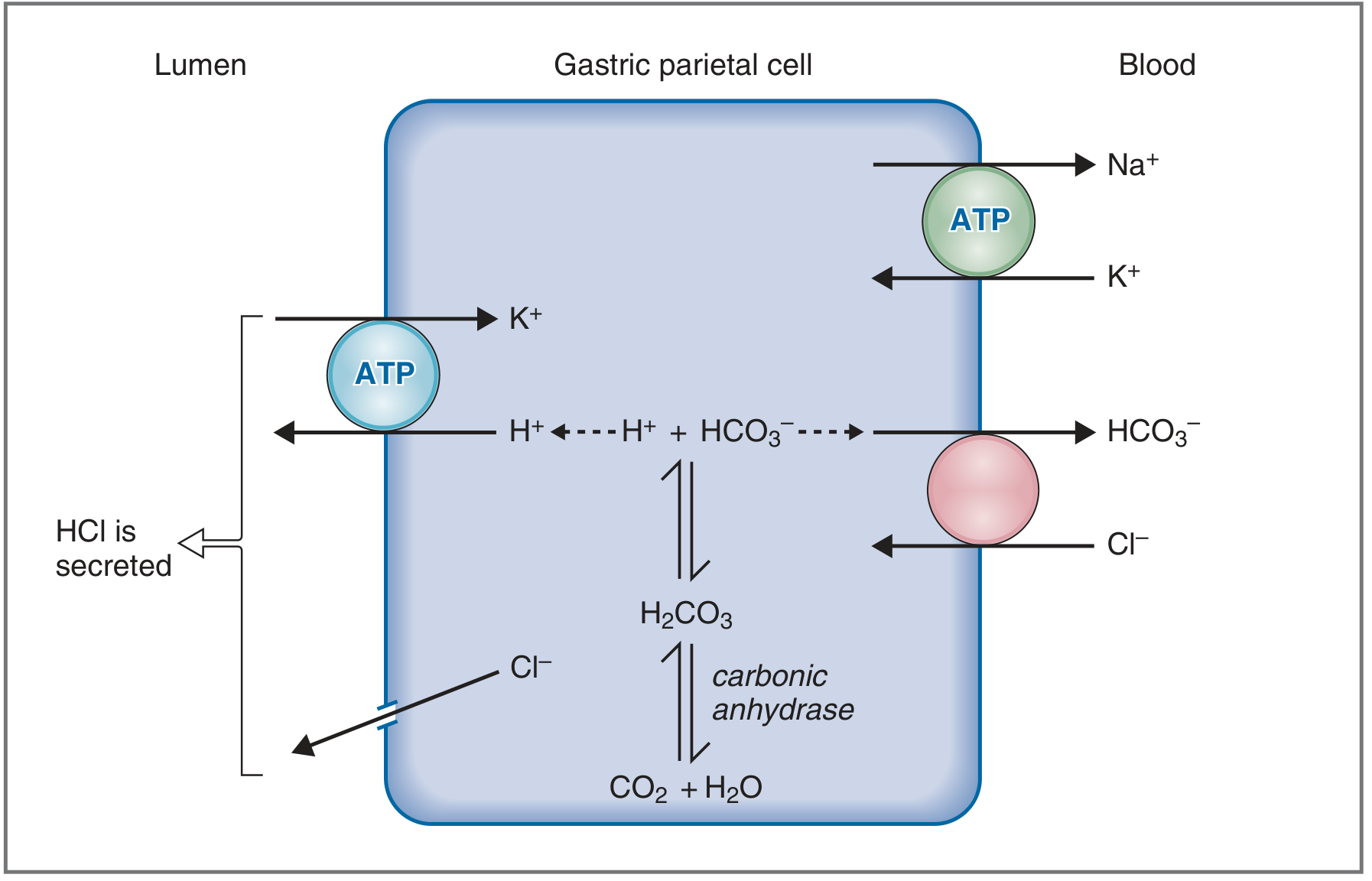
Mechanism of HCl secretion - Costanzo Physiology 7th Edition, Fig. 8.17
The steps are:
Step 1 - CO2 hydration inside the cell:
CO2 (from cellular metabolism or blood) + H2O → H2CO3, catalyzed by carbonic anhydrase inside the parietal cell. H2CO3 immediately dissociates into H+ and HCO3-.
Step 2 - H+ secretion at the apical (luminal) membrane:
H+ is actively pumped into the lumen via H+-K+ ATPase (the proton pump), in exchange for K+. This is a primary active transport mechanism working against a massive electrochemical gradient. K+ that leaks into the lumen via this pump is recycled back into the cell by the same H+-K+ ATPase. Cl- follows H+ passively through Cl- channels in the apical membrane - together forming HCl in the lumen.
Step 3 - HCO3- removal at the basolateral membrane:
HCO3- generated inside the cell is transported out into the blood via a Cl-/HCO3- exchanger on the basolateral membrane. This is responsible for the "alkaline tide" - gastric venous blood has a higher pH than arterial blood after a meal. The Cl- taken up by this exchanger is recycled to the apical side for HCl secretion.
Step 4 - Basolateral Na+-K+ ATPase:
Maintains low intracellular Na+, which drives Na+ reabsorption from the canalicular lumen, leaving H+ and Cl- behind.
Step 5 - Water:
H2O follows by osmosis into the canaliculus.
Final secretion: ~150-160 mEq/L HCl, 15 mEq/L KCl, small amount of NaCl.
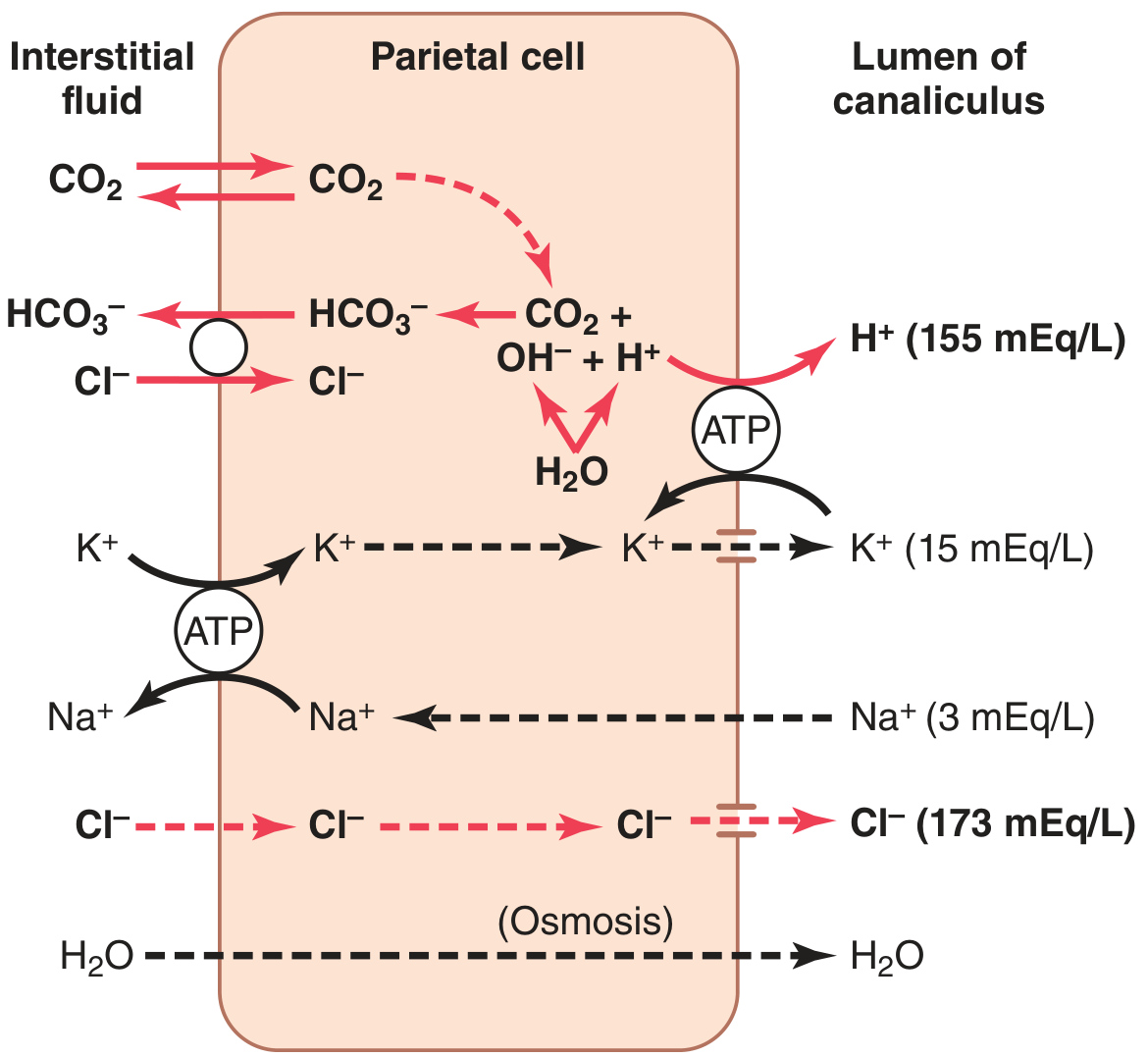
Postulated mechanism of HCl secretion - Guyton and Hall Medical Physiology, Fig. 65.6
Key drug target: H+-K+ ATPase is inhibited by omeprazole (proton pump inhibitors), used clinically to reduce acid secretion. Cimetidine blocks H2 receptors.
- Guyton and Hall Medical Physiology, p. 802; Costanzo Physiology 7th Edition, p. 366
2. Mechanism of Pepsinogen Secretion and Activation
Chief cells secrete pepsinogen (inactive zymogen, MW ~42,500) by exocytosis, stimulated by ACh and gastrin. When pepsinogen contacts HCl in the lumen, it undergoes autocatalytic cleavage to form pepsin (MW ~35,000) - an active protease that initiates protein digestion. Pepsin itself can also activate further pepsinogen (autocatalytic). Pepsin is active at pH 1.8-3.5 and is inactivated at pH >5.
- Guyton and Hall Medical Physiology, p. 802-803
3. Regulation of Gastric Secretion - Three Stimulants
Three principal substances stimulate H+ secretion from parietal cells, each via a distinct receptor and second messenger:
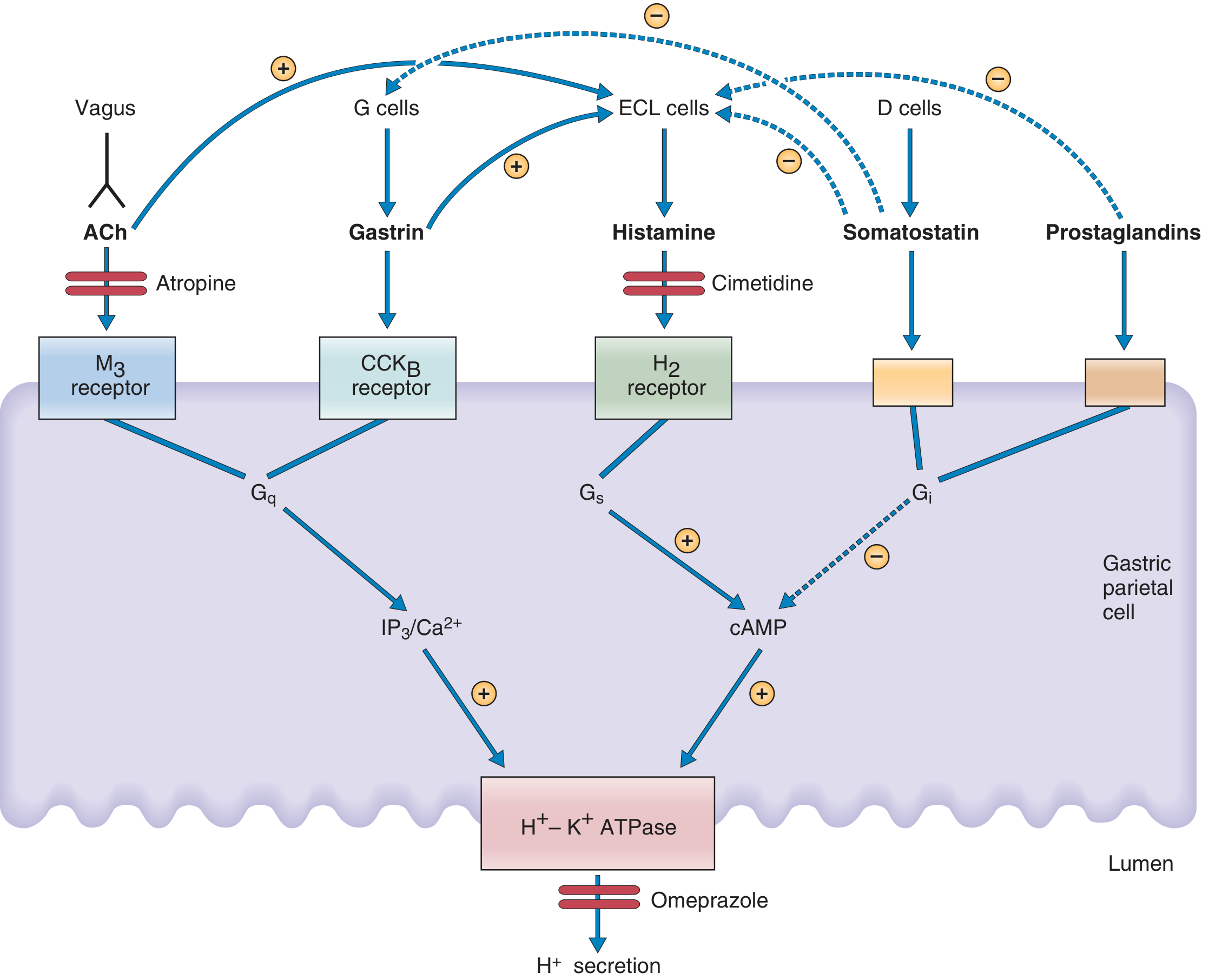
Agents stimulating and inhibiting gastric H+ secretion - Costanzo Physiology 7th Edition, Fig. 8.18
A. Histamine (Paracrine)
- Released by ECL cells in the gastric mucosa
- Binds H2 receptors on parietal cells
- Second messenger: cAMP (via Gs protein → adenylyl cyclase → cAMP → protein kinase A)
- Blocked by: cimetidine (H2 blocker)
B. Acetylcholine (Neurocrine)
- Released by vagus nerve endings in the gastric mucosa
- Binds muscarinic M3 receptors on parietal cells
- Second messenger: IP3/Ca2+ (via Gq → phospholipase C → IP3 → intracellular Ca2+ release)
- Also stimulates peptic cells (pepsinogen) and mucous cells (mucus)
- Blocked by: atropine
- ACh also indirectly stimulates HCl secretion by causing histamine release from ECL cells
C. Gastrin (Endocrine/Hormone)
- Released by G cells in the stomach antrum into the bloodstream (endocrine, not paracrine)
- Binds CCK-B receptors on parietal cells
- Second messenger: IP3/Ca2+ (same pathway as ACh)
- Stimuli for gastrin release: stomach distention, luminal oligopeptides/amino acids, vagal stimulation (via GRP - gastrin-releasing peptide)
- Gastrin also acts on ECL cells to release histamine (indirect H+ stimulation)
Potentiation: The three stimulants potentiate each other's effects - their combined response exceeds the sum of individual responses. This explains why H2 blockers (cimetidine) have a greater-than-expected effect by blocking both direct histamine action AND the indirect histamine-mediated potentiation of ACh and gastrin.
- Costanzo Physiology 7th Edition, pp. 366-368
4. Inhibitors of Gastric Secretion
| Inhibitor | Source | Mechanism |
|---|---|---|
| Somatostatin | D cells (antrum/fundus) | Binds Gi protein → inhibits adenylyl cyclase → lowers cAMP; also inhibits gastrin release from G cells and histamine from ECL cells |
| Prostaglandins (PGE2) | Gastric mucosa | Bind Gi protein on parietal cells → reduce cAMP |
| Low luminal pH (<3) | Feedback | Stimulates somatostatin release from D cells → inhibits G cells (negative feedback loop) |
| GIP, secretin | Duodenum | Inhibit gastrin release during intestinal phase |
- Costanzo Physiology 7th Edition, p. 368; Ganong's Review, p. 461
5. Phases of Gastric Secretion
Cephalic Phase (~30% of total)
- Triggered by sight, smell, taste, and thought of food
- Mediated entirely by vagus nerve (CN X)
- Vagal outflow releases ACh and GRP → stimulates parietal cells directly (via M3) and G cells (via GRP → gastrin release)
- Can be abolished by vagotomy or atropine
Gastric Phase (~60% of total) - quantitatively most important
- Triggered once food enters the stomach
- Stimuli: stomach distention (activates stretch receptors → vago-vagal and local myenteric reflexes) + luminal peptides/amino acids (directly stimulate G cells to release gastrin)
- Food buffers gastric acidity, removing the feedback inhibition and allowing more secretion
- Results in large-volume acid secretion
Intestinal Phase (~10% of total)
- Triggered as chyme enters the duodenum
- Initially brief stimulation by amino acids absorbed from duodenum
- Quickly dominated by inhibition: secretin (released by acid in duodenum), GIP, CCK, and the enterogastric reflex all suppress gastric secretion as acid enters the intestine
- Ganong's Review of Medical Physiology 26th Edition, pp. 460-461; Guyton and Hall, p. 803
6. Mucus-Bicarbonate Barrier (Cytoprotection)
Surface epithelial cells and mucous neck cells secrete an alkaline mucus gel containing HCO3-. This layer:
- Maintains a pH gradient from ~2.0 at the lumen surface to ~7.0 at the cell surface
- Prevents autodigestion of the mucosa
- Also contains trefoil peptides that stabilize the mucus-HCO3- layer
Damage to this barrier (by aspirin, alcohol, NSAIDs, H. pylori) allows acid backdiffusion into the mucosa, causing peptic ulcer disease.
- Guyton and Hall Medical Physiology, p. 803; Ganong's Review, p. 460
Summary Flowchart
Stimuli (cephalic/gastric/intestinal)
↓
Vagus (ACh) + G cells (Gastrin) + ECL cells (Histamine)
↓
Parietal cell receptors (M3, CCK-B, H2)
↓
Second messengers (IP3/Ca2+ or cAMP)
↓
H⁺-K⁺ ATPase activation (apical membrane)
↓
H⁺ secreted into lumen + Cl⁻ follows = HCl
↓
HCO₃⁻ exits into blood (alkaline tide)
Inhibition: Somatostatin, prostaglandins, low pH feedback → reduce H+-K+ ATPase activity.
This is a shared conversation. Sign in to Orris to start your own chat.