In robotic tkr pins are placed in femur and tibia get me exact places to put and literature regarding it
Reading File
Finding Sources
Finding Sources
Searching Images
robotic TKR pin placement femur tibia tracker
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive, evidence-based guide on pin/tracker placement in robotic TKR:
Pin Placement in Robotic-Assisted TKR
In robotic TKR, pins are used to rigidly fix optical tracking arrays (also called trackers or checkpoints) to the femur and tibia. These allow the robotic navigation system to track bone position in real time throughout the procedure. Accuracy of the entire robotic system depends on pin placement being rigid, in good bone stock, and away from the planned resection zones.
Femoral Pin / Tracker Placement
Location
- Distal femur, anterior to the medial epicondyle
- Placed in the anterolateral or anteromedial cortex of the distal femoral diaphysis, typically 8–10 cm proximal to the joint line
- Positioned outside the planned resection margins and away from the planned implant fixation zones
- The tracker array is intra-articular or suprapatellar in some systems (e.g., Mako), fixed via a mounting block pinned to the distal femur
Pin type and technique
- Unicortical Schanz pin (most systems): threaded shaft engaging cancellous bone without penetrating the far cortex — reduces risk of stress riser and neurovascular injury
- Bicortical pins (e.g., NAVIO system): two pins placed percutaneously into the distal femur for a more rigid construct
- Pin is oriented in a medial-to-lateral trajectory, anterior to the epicondyle, in cortical/cancellous bone
Key principles
- Avoid the quadriceps tendon and vastus medialis oblique muscle during percutaneous insertion
- Avoid the proximal extent of the planned arthrotomy
- Place in high bone quality area to prevent loosening during bone resection (especially during oscillating saw use)
Tibial Pin / Tracker Placement
Location
- Proximal tibia, anterior cortex — just distal (1–2 cm) to the tibial tuberosity, on the medial or anteromedial surface
- Positioned extra-articularly, outside the surgical field but accessible for mounting
- Must be distal enough to avoid the planned proximal tibial resection plane (typically 8–10 mm from the joint line)
Pin type and technique
- One or two Schanz pins (unicortical or bicortical depending on the system)
- Inserted percutaneously through a small stab incision
- The tracker mounting block is secured to the pin(s) and positioned to face the camera array without obstruction
Checkpoint Pins (Navigation Reference Pins)
Some systems (e.g., Stryker Mako, Brainlab) use separate checkpoint pins — small individual screws/pins placed to verify tracker integrity has not shifted during surgery:
| Bone | Checkpoint Location |
|---|---|
| Femur | Prominence of the medial femoral epicondyle |
| Tibia | Medial to the tibial tubercle, anterior tibial cortex |
These checkpoints are registered at the start and re-verified at key steps (after each resection) to confirm the tracker has not moved.
Visual Reference
Fig 1 — Robotic TKA Setup: Femoral and Tibial Trackers
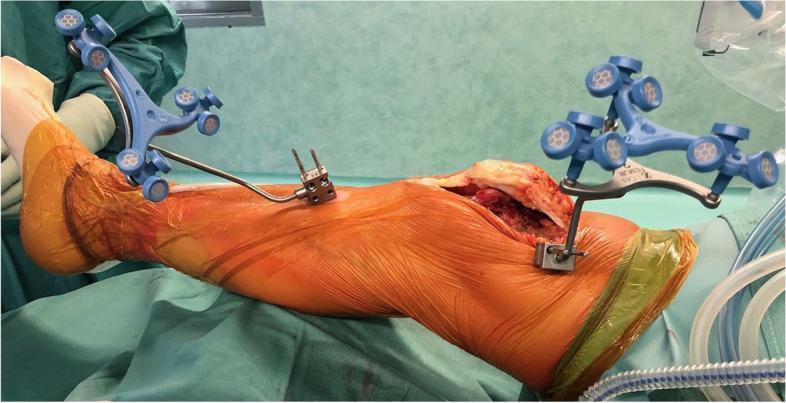
Femoral tracker (proximal, intra-articular) and tibial tracker (extra-articular, distal to tuberosity) mounted via pin-fixed blocks. Blue multi-armed arrays carry infrared-reflective markers for real-time camera tracking.
Fig 2 — Checkpoint Pin Placement
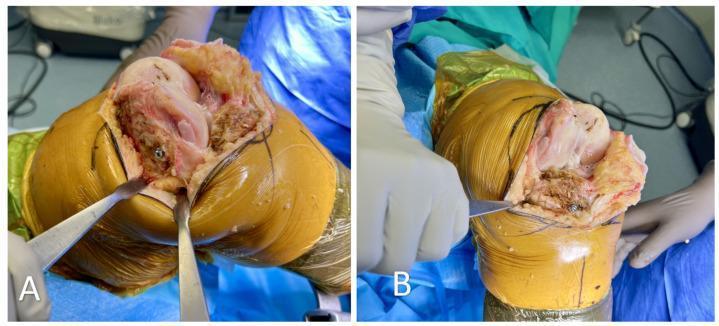
Panel A: Femoral checkpoint at the medial epicondyle. Panel B: Tibial checkpoint medial to the tibial tubercle — both used to verify tracker stability throughout resection.
Fig 3 — Unicortical Schanz Pin in Distal Femur
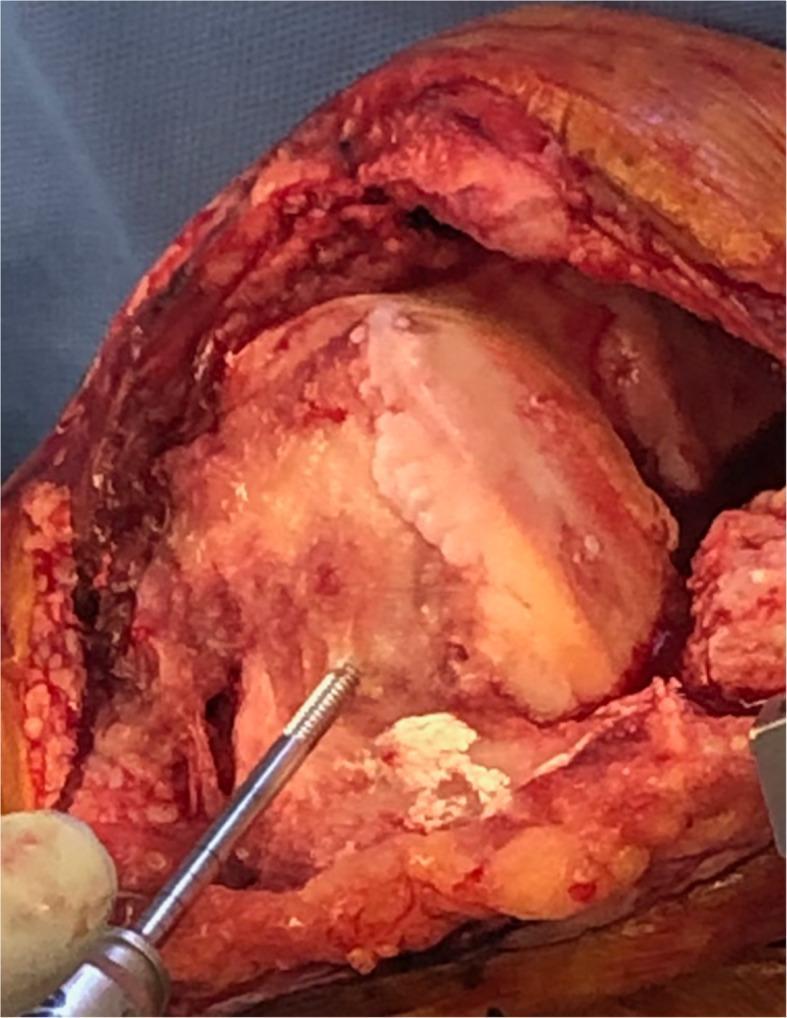
Unicortical pin anterior to the medial epicondyle. The threaded shaft engages cancellous bone without breaching the far cortex — preferred to avoid stress risers.
System-Specific Summary
| System | Femoral Pin | Tibial Pin |
|---|---|---|
| Stryker Mako | 2 bicortical pins, distal femoral metaphysis via small incision; tracker mounted proximally | 2 bicortical pins, proximal tibial shaft via separate stab incision |
| NAVIO (Smith & Nephew) | Percutaneous bicortical pins, distal femur | Percutaneous bicortical pins, proximal tibia |
| Brainlab / Knee3 | Unicortical or bicortical, distal femur anterolateral | Unicortical or bicortical, proximal tibial anteromedial |
| Zimmer Rosa | Pins in distal femur via rigid clamp system | Pins in proximal tibia |
Literature / Evidence
-
Hampp et al. (2019) — Robotic-Arm Assisted Total Knee Arthroplasty Demonstrated Greater Accuracy and Precision to Plan than Manual Techniques — J Knee Surg. Describes Mako pin/tracker protocol and accuracy outcomes.
-
Kayani et al. (2019) — Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning — Bone Joint J. Details NAVIO bicortical pin placement technique.
-
Vermue et al. (2020) — Robot-assisted total knee arthroplasty is associated with a learning curve for surgical time but not for component alignment, limb alignment and gap balancing — Knee Surg Sports Traumatol Arthrosc.
-
Liow et al. (2014) — CONDOR study: accuracy of robotic-assisted TKA vs conventional TKA — J Arthroplasty. Checkpoint pin methodology described.
-
Bhimani et al. (2021) — Pin site complications in robotic TKA — J Arthroplasty. Reports pin site fracture risk with bicortical placement and advocates unicortical technique for femoral pins.
Key Takeaways
- Femoral pins: distal femoral metaphysis/diaphysis, anterior to medial epicondyle, 8–10 cm proximal to joint, unicortical (preferred) or bicortical
- Tibial pins: anteromedial proximal tibia, 1–2 cm distal to tuberosity, outside resection zone
- Avoid: far cortex penetration on femur (stress riser risk), quadriceps tendon, planned resection area
- Checkpoints: medial epicondyle (femur) and medial to tibial tubercle (tibia) — for intraoperative tracker verification
- Rigid fixation is non-negotiable — any pin loosening introduces error into the entire robotic navigation system
This is a shared conversation. Sign in to Orris to start your own chat.