Acute coronary syndrome
Reading File
Finding Sources
Searching PubMed
"acute coronary syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have rich, comprehensive content from multiple authoritative textbooks plus the management flowchart. Let me compile the full answer.
Acute Coronary Syndrome (ACS)
Definition and Classification
ACS describes the continuum of myocardial ischemia/infarction caused by acute compromise of coronary blood flow. It encompasses three entities distinguished by ECG findings and biomarkers:
| Entity | ST on ECG | Troponin | Key feature |
|---|---|---|---|
| Unstable Angina (UA) | No ST elevation | Negative | New, worsening, or rest angina - no myonecrosis |
| NSTEMI | No ST elevation (may have ST depression/T-wave changes) | Positive | Myonecrosis without persistent ST elevation |
| STEMI | Persistent ST elevation (>20 min) | Positive | Full-thickness injury, complete occlusion |
UA and NSTEMI together are termed NSTE-ACS because they share pathophysiology and initial management. STEMI requires a distinct, time-critical reperfusion strategy.
- Goldman-Cecil Medicine, p. 638
Epidemiology
- ~1.2 million Americans hospitalized annually with ACS
- About two-thirds have NSTE-ACS; one-third have STEMI
-
50% of NSTE-ACS patients are older than 65 years; nearly half are women
- Strong associations with atherosclerosis risk factors, peripheral vascular disease, and chronic inflammatory disorders (rheumatoid arthritis, psoriasis, lupus)
Pathophysiology
Type 1 MI - Plaque Rupture (Most Common)
The central event is atherosclerotic plaque rupture or erosion, followed by platelet aggregation and thrombus formation causing subtotal (NSTEMI/UA) or total (STEMI) coronary occlusion.
Molecular mechanisms driving plaque vulnerability:
- Oxidized LDL deposition triggers macrophage and T-lymphocyte infiltration at the plaque border
- These inflammatory cells secrete cytokines (TNF, IL-1, IFN-γ) that inhibit collagen synthesis and enzymes (matrix metalloproteinases, cathepsins) that degrade collagen and elastin, thinning the fibrous cap
- Sites of low shear stress (vessel bifurcations) accumulate lipids and inflammatory cells, accelerating cap thinning
- Plaque neovascularization (driven by VEGF, FGF, etc.) makes the plaque structurally fragile
ACS is often a diffuse, systemic process - angiographic studies frequently show plaque ulceration at multiple coronary sites simultaneously, not just one culprit lesion.
Type 2 MI - Supply/Demand Mismatch
Occurs without plaque rupture; caused by:
- Reduced supply: hypotension, severe anemia, hypoxemia, coronary vasospasm (Prinzmetal angina), cocaine, triptans, spontaneous coronary artery dissection (SCAD - especially peripartum women)
- Increased demand: tachycardia, severe hypertension, thyrotoxicosis
In Type 2 MI, therapy must target the underlying cause.
- Goldman-Cecil Medicine, p. 638-639
Clinical Presentation
Classic symptoms:
- Substernal chest pain/pressure, often radiating to the left arm, jaw, or back
- Diaphoresis, nausea, dyspnea
Atypical presentations (more common in elderly, women, diabetics):
- Dyspnea alone, syncope, fatigue, weakness, abdominal pain, delirium
- "Classic" chest pain occurs in only ~50% of patients aged ≥85 years
- One-third of women >65 years with AMI present with abdominal pain alone
- Acute heart failure at presentation occurs in ~50% of STEMI patients ≥85 years (vs. 1.7% in those <65)
Physical exam may show: diaphoresis, S3/S4 gallop, new mitral regurgitation murmur (papillary muscle ischemia), signs of cardiogenic shock (hypotension, cool extremities, altered mental status).
- Rosen's Emergency Medicine, p. 4015-4021
Diagnosis
ECG
- STEMI: New ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads (or new LBBB)
- NSTEMI/UA: ST depression, T-wave inversions, or normal ECG
- Serial ECGs should be obtained if initial is non-diagnostic
Biomarkers
- High-sensitivity troponin (hsTn) is the cornerstone biomarker - can detect myonecrosis within 1-3 hours of symptom onset
- Serial measurements at 0h and 1-3h (or 0h/3h/6h depending on assay)
- Unstable angina: troponin remains negative throughout
Risk Stratification Scores
TIMI Score (UA/NSTEMI) - 7 variables, scored 0-7:
- Age ≥65, ≥3 CAD risk factors, prior coronary stenosis ≥50%, ST deviation on ECG, ≥2 anginal events in prior 24h, aspirin use in prior 7 days, elevated cardiac markers
- Score 0-2 = low risk; 3-4 = intermediate; 5-7 = high risk
- Advantage: simple integer sum, calculable at bedside without a computer
GRACE Score - uses age, Killip class, heart rate, systolic BP, creatinine, ST deviation, cardiac arrest at admission, troponin
-
Derived from a large international registry (less-selected population)
-
Score ≥140 = high risk; better calibration between predicted and observed mortality than TIMI
-
Includes renal insufficiency as a variable (an advantage over TIMI)
-
Available at gracescore.org
-
Fuster and Hurst's The Heart, 15th Ed.; Sabiston Textbook of Surgery
Management
Immediate General Measures (MONA-B framework)
- Monitoring: continuous ECG, pulse oximetry, IV access
- Oxygen: only if SpO2 <90%
- Nitrates: sublingual/IV for ongoing ischemia (contraindicated if hypotension, RV infarction, or PDE5 inhibitor use within 24-48h)
- Aspirin: 325 mg chewed loading dose immediately for all ACS
- Beta-blockers: oral, within 24h if no signs of HF, low-output state, or AV block (reduce heart rate and myocardial oxygen demand)
Antithrombotic Therapy
Antiplatelet (dual antiplatelet therapy - DAPT)
- Aspirin 75-100 mg/day indefinitely
- P2Y12 inhibitor added to aspirin for 12 months:
- Ticagrelor (preferred over clopidogrel - faster onset, more potent, shown to reduce mortality in PLATO trial)
- Prasugrel (use for PCI patients; avoid if history of TIA/stroke, age >75, weight <60kg)
- Clopidogrel (alternative, especially if ticagrelor/prasugrel contraindicated or not available)
Anticoagulation
- Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH, e.g., enoxaparin), fondaparinux, or bivalirudin
- LMWH/fondaparinux preferred over UFH for NSTE-ACS in most patients (lower bleeding risk)
- Anticoagulation continued through PCI or until hospital discharge in medically managed patients
GP IIb/IIIa inhibitors (eptifibatide, tirofiban): reserved for high-risk patients undergoing PCI or with evidence of ongoing ischemia despite DAPT
Invasive Strategy Timing (NSTE-ACS)
This is guided by clinical risk (see flowchart):
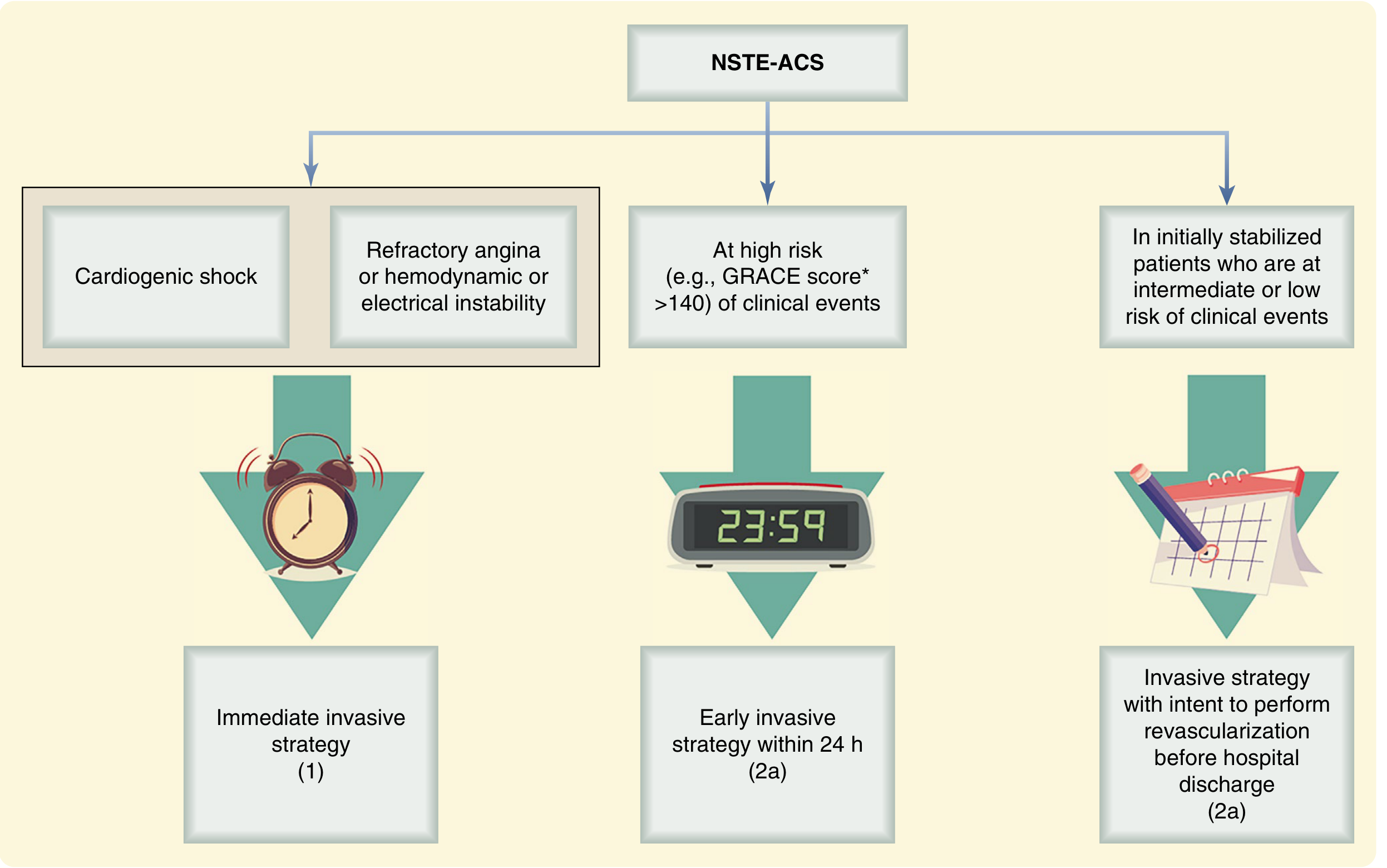
From Sabiston Textbook of Surgery, based on 2021 ACC/AHA/SCAI Revascularization Guidelines
| Risk Level | Timing | Indications |
|---|---|---|
| Immediate (<2h) | Immediate invasive | Cardiogenic shock, refractory angina, hemodynamic/electrical instability |
| Early (<24h) | Early invasive | GRACE score >140, troponin elevation, new ST depression |
| Selective (before discharge) | Invasive strategy | Initially stabilized, low/intermediate risk |
The TIMACS and VERDICT trials confirmed early invasive management (<24h) notably lessens cardiovascular complications in high-risk patients.
STEMI-Specific Management
- Primary PCI is the gold standard - target door-to-balloon time <90 minutes (or <120 minutes if transferred)
- Fibrinolysis (alteplase, tenecteplase) if PCI not available within 120 minutes of first medical contact; followed by "pharmaco-invasive" strategy (coronary angiography within 24h)
Other Medications
- High-intensity statins (atorvastatin 40-80 mg or rosuvastatin 20-40 mg): started in-hospital, continued indefinitely - stabilize plaque, reduce LDL
- ACE inhibitors/ARBs: for all patients with EF <40%, hypertension, or diabetes
- Aldosterone antagonists (eplerenone): if EF <40% post-MI, no significant renal impairment or hyperkalemia
Complications
| Complication | Timing | Notes |
|---|---|---|
| Arrhythmias (VF, VT) | Early (first 24-48h) | Leading cause of early death; continuous monitoring essential |
| Cardiogenic shock | Within hours to days | ~7-10% of STEMI; high mortality; require urgent PCI + hemodynamic support |
| Acute mitral regurgitation | Days 2-7 | Papillary muscle rupture; severe pulmonary edema; needs urgent surgery |
| Free wall rupture | Days 3-5 | Catastrophic; pericardial tamponade |
| Ventricular septal defect | Days 3-7 | New harsh systolic murmur; cardiogenic shock |
| Right ventricular infarction | Accompanies inferior STEMI | Hypotension + clear lungs; avoid nitrates/diuretics; fluids are treatment |
| Dressler syndrome | Weeks post-MI | Pericarditis, pleuritis, fever; autoimmune; treat with NSAIDs/colchicine |
Secondary Prevention (Post-ACS)
- Aspirin indefinitely
- P2Y12 inhibitor for 12 months (duration may be adjusted based on bleeding vs. ischemic risk)
- High-intensity statin indefinitely
- Beta-blocker (especially if reduced EF)
- ACE inhibitor/ARB
- Cardiac rehabilitation
- Risk factor modification: smoking cessation, BP control, diabetes management, weight loss
Recent Evidence Updates (2024-2026)
Three recent systematic reviews/meta-analyses are notable:
-
DAPT de-escalation (Valgimigli et al., Lancet 2024, PMID 39226909): De-escalation to ticagrelor monotherapy (dropping aspirin after 1-3 months) vs. 12 months of DAPT - individual patient-level meta-analysis showing reduced bleeding without excess ischemic risk.
-
Elderly ACS - invasive vs. conservative (Reddy et al., JAMA Intern Med 2025, PMID 40549394): Meta-analysis of early invasive vs. conservative strategy in older patients with ACS - supports early invasive approach in selected elderly patients.
-
Aspirin vs. P2Y12 monotherapy post-PCI (Laudani et al., JACC Cardiovasc Interv 2025, PMID 40803759): Network meta-analysis comparing aspirin monotherapy vs. P2Y12 inhibitor monotherapy after PCI for ACS - ongoing evolution of post-PCI antithrombotic strategy.
Primary sources: Goldman-Cecil Medicine International Edition; Sabiston Textbook of Surgery; Fuster and Hurst's The Heart, 15th Ed.; Rosen's Emergency Medicine
Give in a colorful and using images
Asking for Preferences
Generating Image
This is a shared conversation. Sign in to Orris to start your own chat.