Give me 40 ECG cases practice (ICU level and OPD) ECG all details according to disease ECG kaise dekhe with photos case and uses treatment
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram atrial fibrillation interpretation
Searching Images
ECG STEMI myocardial infarction ST elevation
Searching Images
ECG ventricular tachycardia ventricular fibrillation complete heart block
Searching Images
ECG hyperkalemia hypokalemia electrolyte changes
Searching Images
ECG Wolff-Parkinson-White SVT pulmonary embolism right heart strain
Now I have excellent ECG images from the library. Let me compile the comprehensive 40-case guide with all available images.
🫀 40 ECG Cases: ICU + OPD Practice Guide
ECG Kaise Dekhe — Systematic Approach + Cases with Photos & Treatment
📋 ECG DEKHNE KA SYSTEMATIC APPROACH (How to Read an ECG)
Every ECG read in this order:
| Step | Parameter | Normal Value |
|---|---|---|
| 1 | Rate | 60–100 bpm (1 large square = 0.2s; 300 ÷ R-R large squares) |
| 2 | Rhythm | Regular? P before every QRS? |
| 3 | Axis | Lead I +ve, aVF +ve = Normal axis |
| 4 | P wave | Present? Normal? PR = 0.12–0.20s |
| 5 | QRS | <0.12s (3 small squares) |
| 6 | ST segment | Isoelectric? Elevation/Depression? |
| 7 | T wave | Upright in I, II, V3–V6 |
| 8 | QT interval | QTc <440ms men, <460ms women |
| 9 | Special features | Q waves, delta, U waves, etc. |
🔴 ICU LEVEL CASES (Cases 1–20)
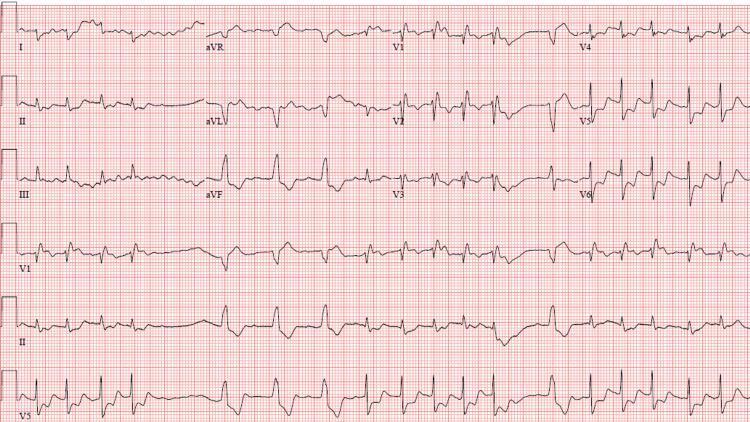
CASE 1 — Anterior STEMI (LAD Occlusion)
Clinical scenario: 55M, chest pain 2h, diaphoresis, BP 90/60
Setting: ICU/Emergency
Setting: ICU/Emergency

ECG Findings:
- ST elevation: V1–V6 (anterior leads) — convex/tombstone morphology
- Reciprocal ST depression: aVR, aVL (lateral reciprocal)
- Hyperacute T waves: V2–V4 (tall, broad)
- QS waves: V2–V3 (necrosis if established)
- Rate: Sinus, may have bradycardia (vagal) or tachycardia (shock)
Territory:
V1–V4 = LAD (anterior) | V4–V6, I, aVL = Cx (lateral) | II, III, aVF = RCA (inferior)
Treatment (ICU):
- STEMI Protocol: Door-to-balloon <90 min
- Aspirin 325mg + Clopidogrel/Ticagrelor
- Heparin UFH bolus IV
- PCI (Primary — gold standard) / Thrombolysis if PCI not available (Streptokinase/Tenecteplase)
- Morphine 2–4mg IV for pain
- Oxygen if SpO2 <90%
- Beta-blocker (if HR >60, no shock, no AV block)
- ACE inhibitor start within 24h
CASE 2 — Anterolateral STEMI
Clinical scenario: 62F, crushing chest pain, ST elevation V1–V6 + I + aVL

ECG Findings:
- ST elevation: V1–V6, Lead I, aVL — proximal LAD occlusion
- Reciprocal depression: II, III, aVF (inferior leads)
- Hyperacute T waves: V2–V4
- Wide QRS in leads with max ST elevation
Key Teaching Point:
Reciprocal changes (ST depression in opposite leads) confirm STEMI diagnosis. If V1–V6 + I + aVL involved → proximal LAD = worst prognosis, may need emergency CABG.
Treatment:
Same as Case 1 + urgent cardiology call for proximal LAD — consider IABP for cardiogenic shock.
CASE 3 — Inferolateral STEMI (RCA/Circumflex)
Clinical scenario: 58M, inferior chest discomfort, diaphoresis, HR 45
ECG Findings:
- ST elevation: II, III, aVF (inferior) + V4–V6 (lateral)
- Reciprocal ST depression: aVL, Lead I
- Hyperacute T waves: merging with ST segment
- Bradycardia: common with inferior MI (vagal + SA node ischemia)
Key Teaching Point:
Always do right-sided leads (V3R–V4R) in inferior MI to rule out Right Ventricular infarction (ST elevation V4R = RV MI → avoid nitrates, give IV fluids).
Treatment:
- PCI/thrombolysis
- Atropine 0.5mg IV for symptomatic bradycardia
- Avoid nitrates if RV involvement
- IV fluid bolus for hypotension with RV MI
CASE 4 — Tombstone STEMI (LAD, Extensive)
Clinical scenario: 70M, out-of-hospital cardiac arrest, resuscitated, ICU admission
ECG Findings:
- Massive ST elevation V2–V5 — "tombstone" pattern
- Convex-upward (coved) morphology
- Reciprocal: II, III, aVF with ST depression
- Indicates proximal LAD occlusion with large territory at risk
Tombstone Pattern:
ST elevation so prominent it merges with QRS and T wave, forming a "tombstone" shape. Very high mortality. Associated with cardiogenic shock.
Treatment:
- Immediate PCI (emergent)
- IABP/Impella for cardiogenic shock
- Targeted temperature management if post-cardiac arrest (33–36°C for 24h)
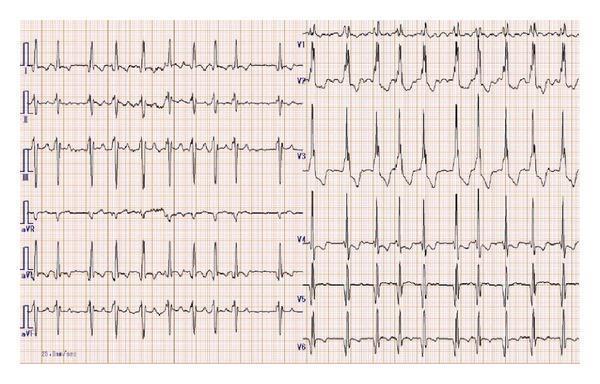
CASE 5 — Atrial Fibrillation with Rapid Ventricular Response (RVR)
Clinical scenario: 65M, palpitations, dyspnea, HR 134, BP 100/70
ECG Findings:
- No P waves — replaced by irregular fibrillatory baseline (f waves)
- Irregularly irregular R-R intervals (key feature)
- Narrow QRS <120ms (supraventricular origin)
- Rate: ~134 bpm (RVR = >100 bpm)
- Poor R-wave progression (PRWP) V1–V3
ECG Kaise Pehchaanein (How to identify AF):
Rule of 3 "Irregulars": Irregular rhythm + Irregular baseline + Irregular QRS intervals = AF until proven otherwise
Treatment (ICU — hemodynamically unstable):
- Synchronized cardioversion 120–200J (if unstable)
- Rate control if stable: IV Metoprolol 5mg slow, or Diltiazem 0.25mg/kg
- Rhythm control: Amiodarone IV 150mg over 10 min, then infusion
- Anticoagulation: Heparin if >48h or unknown duration
- Treat cause: thyroid, infection, hypoxia, electrolytes
CASE 6 — Atrial Fibrillation with Complete Heart Block
Clinical scenario: 72M, syncope, HR 40, irregular P waves but slow regular ventricles
ECG Findings:
- Atrial activity: Fibrillatory waves ~180 bpm (no organized P waves)
- Ventricular rate: ~43 bpm — slow, regular
- AV dissociation: Atrial and ventricular activity completely independent
- Narrow QRS: Junctional escape focus (supra-Hisian)
Key Teaching Point:
In AF, the rhythm is always irregularly irregular. If you see AF with a regular ventricular response — think Complete Heart Block with escape rhythm. This is a high-grade emergency.
Treatment:
- Temporary pacemaker (transcutaneous → transvenous)
- Atropine 0.5–1mg IV (may not work in complete block)
- Dopamine/Adrenaline infusion as bridge
- Permanent pacemaker implantation
CASE 7 — Complete AV Block + VT
Clinical scenario: 68F, syncope, Stokes-Adams attack, HR varies
ECG Findings:
- P waves: Regular, independent of QRS
- Wide QRS complexes at slow escape rate
- Runs of VT: Broad, bizarre QRS complexes at rapid rate
- AV dissociation: Complete
Treatment:
- Immediate temporary pacing
- Amiodarone for VT suppression
- Defibrillation if degenerates to VF
- Urgent electrophysiology consultation
CASE 8 — Atrial Fibrillation with RBBB
Clinical scenario: 70F, palpitations, previous cardiac surgery, wide QRS irregularly irregular
ECG Findings:
- Irregularly irregular rhythm
- No P waves (AF)
- Wide QRS >120ms
- RBBB morphology: rsR' (M-shape) in V1 + broad S waves in I, aVL, V5, V6
- T-wave inversions in right precordial leads (normal with RBBB)
RBBB vs LBBB Quick Tip:
| Feature | RBBB | LBBB |
|---|---|---|
| V1 | rsR' (M pattern) | QS or rS (W pattern) |
| V6/I | Wide S wave | Wide R, no S |
| Cause | RV overload, PE | LV disease, ischemia |
Treatment:
- Treat AF (rate control/anticoagulation)
- RBBB alone: usually no specific treatment unless symptomatic
- Investigate for structural cause
CASE 9 — Torsades de Pointes (TdP)
Clinical scenario: 55M on antipsychotics, recurrent syncope, QTc 580ms
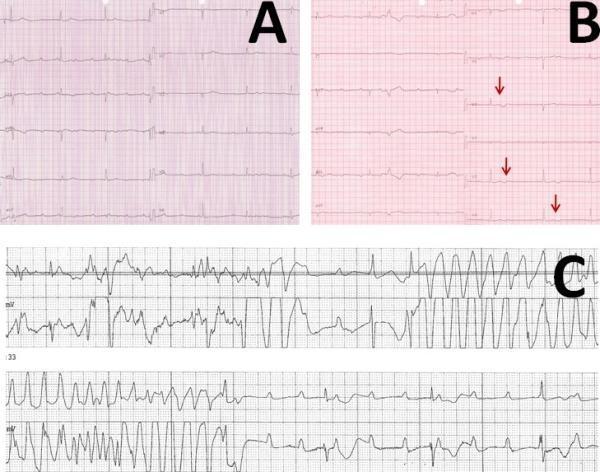
ECG Findings:
- Panel A: Complete AV block with bradycardia
- Panel B: Prolonged QT + notched T waves (warning sign)
- Panel C: TdP — wide QRS complexes twisting around the isoelectric baseline, varying amplitudes and cycle lengths — pathognomonic!
Causes of Long QT (mnemonic: ABCDE):
- Antiarrhythmics (amiodarone, sotalol)
- Bradycardia
- Congenital (Romano-Ward, Jervell-Lange-Nielsen)
- Drugs (antipsychotics, antibiotics — azithromycin, antimalarials)
- Electrolytes (↓K, ↓Mg, ↓Ca)
Treatment (ICU Emergency):
- IV Magnesium Sulfate 2g over 5–15 min (first-line even if Mg normal)
- Stop offending drugs
- Correct electrolytes (K >4.5, Mg >2)
- Overdrive pacing at 90–100 bpm to shorten QT
- Isoproterenol infusion (acquired TdP, bradycardia-dependent)
- NOT amiodarone (prolongs QT further)
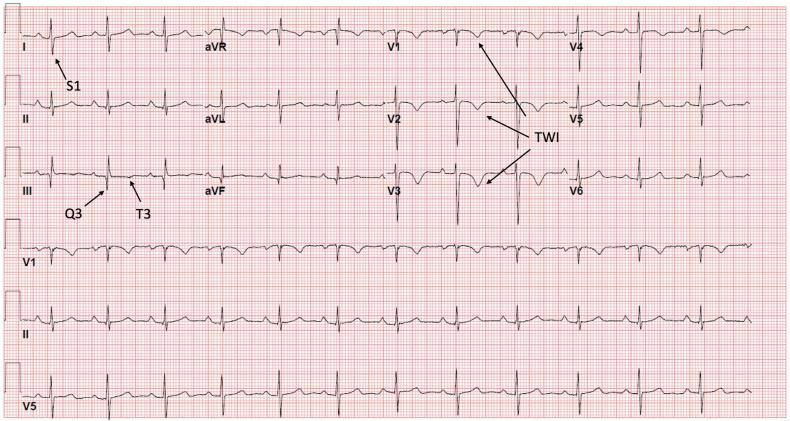
CASE 10 — Pulmonary Embolism (S1Q3T3)
Clinical scenario: 45F, post-surgery day 3, sudden dyspnea, HR 116, SpO2 88%

ECG Findings:
- Sinus tachycardia ~116 bpm (most common finding in PE)
- S1Q3T3 pattern (McGinn-White sign):
- S wave in Lead I (prominent)
- Q wave in Lead III
- T inversion in Lead III
- T-wave inversions V1–V3 (right precordial) = RV strain
- Incomplete RBBB (QRS 110ms, S in V5–V6)
PE ECG Quick Memory Aid:
"SI QIII TIII" = S in I, Q in III, T-inversion in III + sinus tachycardia = Think PE!
Treatment:
- Anticoagulation: Heparin UFH bolus + infusion (or LMWH/DOAC if stable)
- Massive PE + hemodynamic instability: Systemic thrombolysis (Alteplase 100mg over 2h)
- CDT (catheter-directed therapy) if thrombolysis contraindicated
- Surgical embolectomy (last resort)
- Oxygen, IV fluids (cautious — RV overload)
- Vasopressors (Norepinephrine) for shock
CASE 11 — PE with More Extensive RV Strain
Clinical scenario: ICU patient, mechanically ventilated, suddenly deteriorating
ECG Findings:
- S1Q3T3 labeled
- Deep T-wave inversions V1–V6 (severe RV strain)
- Sinus tachycardia
- T inversions extending across ALL precordial leads = submassive/massive PE
Severity Classification of PE by ECG:
| ECG Finding | PE Severity |
|---|---|
| Sinus tachycardia only | Low-moderate |
| S1Q3T3 | Moderate-high |
| T inversions V1–V3 | High (RV strain) |
| T inversions V1–V6 | Massive PE |
| RBBB | High-risk |
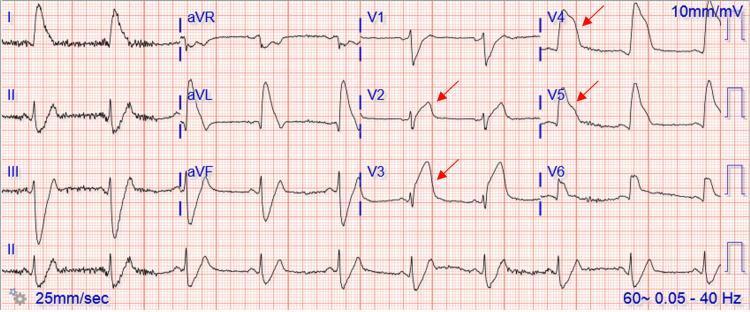
CASE 12 — Hyperkalemia (Peaked T Waves → Sine Wave)
Clinical scenario: 52M, CKD on dialysis, missed session, HR 55, muscle weakness
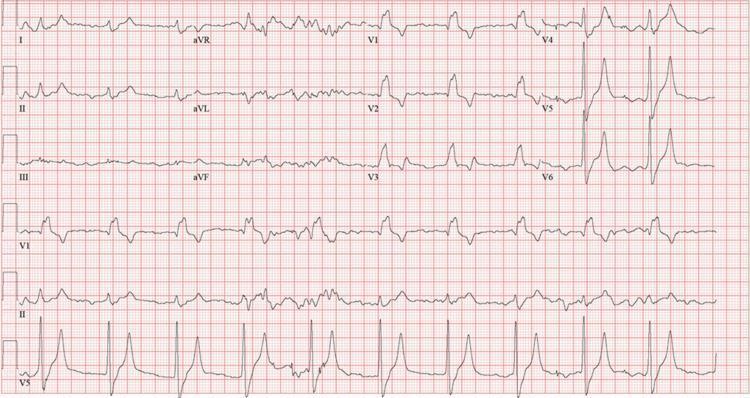
ECG Findings:
- Peaked (tented) T waves V4–V5 — narrow base, symmetric (first sign)
- Prolonged PR interval (1st degree AV block)
- Wide QRS >120ms (RBBB morphology)
- Progressive changes with rising K+:
Hyperkalemia ECG Progression (K+ levels):
| K+ (mEq/L) | ECG Change |
|---|---|
| 5.5–6.0 | Peaked T waves |
| 6.0–6.5 | PR prolongation |
| 6.5–7.0 | Wide QRS, P flattening |
| 7.0–8.0 | Sine wave pattern |
| >8.0 | VF/asystole |
Treatment (ICU Emergency):
- Calcium gluconate 1g IV over 5 min (cardiac membrane stabilization — works in 5 min, lasts 30–60 min)
- Insulin 10 units + Dextrose 50% 50mL (shifts K intracellularly — works in 30 min)
- Salbutamol nebulization 10–20mg (works in 30 min)
- Sodium bicarbonate 50mEq IV (if acidotic)
- Furosemide IV (if urine output present)
- Kayexalate/Patiromer (GI excretion — slow)
- Emergency dialysis (definitive — if oliguric/anuric)
CASE 13 — Electrolyte ECG Comparison Chart
Clinical scenario: ICU monitoring, quick reference for electrolyte disturbances
All 4 Electrolyte Patterns:
| Electrolyte | Key ECG Change | Memory Aid |
|---|---|---|
| Hypokalemia | Flat T + prominent U waves + ST depression | "K goes down, U go up" |
| Hyperkalemia | Peaked (tented) T waves, wide QRS | "High K, High T, Huge QRS" |
| Hypocalcemia | Prolonged ST → Long QT | "Ca down = QT up" |
| Hypercalcemia | Short ST → Short QT | "Ca up = QT down" |
CASE 14 — Hypokalemia (with U Waves)
Clinical scenario: 34F, eating disorder/diuretic abuse, weakness, K = 2.1 mEq/L
ECG Findings:
- Diffuse ST depression
- T-wave flattening (V2–V6)
- Prominent U waves after T waves (best seen V3–V5)
- Prolonged QU interval (appears as long QT)
- T inversion in aVR
U Wave Tips:
U waves are normally present but small. When they become larger than T wave → hypokalemia, bradycardia, digitalis. U waves in V2–V3 best seen at 25mm/s.
Treatment:
- IV KCl replacement max 40mEq/h via central line
- Oral K if mild (K>3.0 and asymptomatic)
- Replace Magnesium first (hypoMg causes refractory hypoK)
- Monitor ECG continuously
CASE 15 — Hypokalemia with VPCs (Before/After K Replacement)
Clinical scenario: 60M, post-op day 2, K = 2.4, frequent irregular beats

ECG Findings:
- Top panel: Sinus rhythm + multifocal VPCs + R-on-T phenomenon, QTc 485ms
- Bottom panel: After K+ replacement — VPCs completely resolved, QTc normalized to 422ms
R-on-T Phenomenon:
When a premature ventricular beat falls on the vulnerable period of T wave (relative refractory period) → can trigger VF. Very dangerous with hypokalemia!
Treatment:
- Aggressive K replacement + Magnesium
- Continuous ECG monitoring
- Avoid QT-prolonging drugs
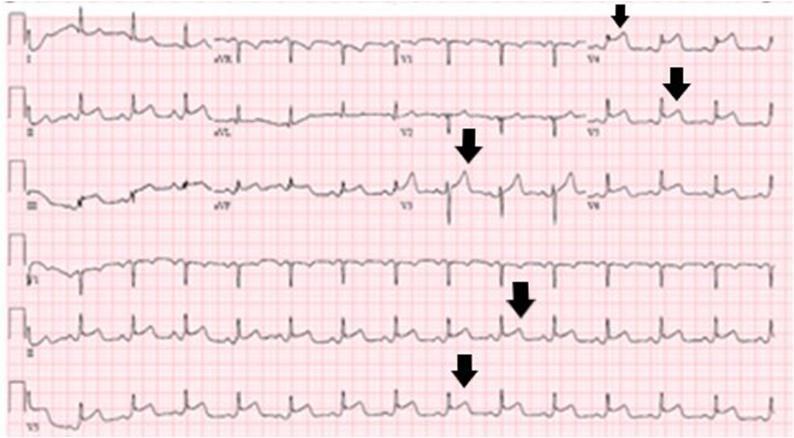
CASE 16 — Hypokalemia with Annotated Features
Clinical scenario: 28F, vomiting x 5 days, severe weakness, K = 2.0
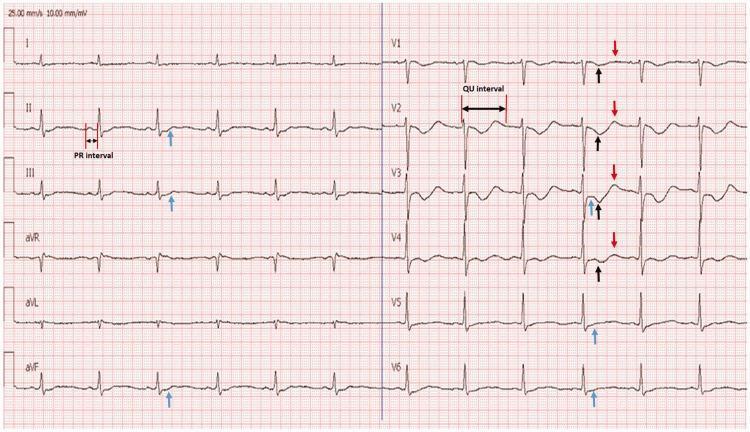
ECG Findings (Annotated with Arrows):
- Blue arrows: ST depression (V1–V4)
- Black arrows: T-wave inversion
- Red arrows: Prominent U waves
- Double arrow: Prolonged QU interval in V2
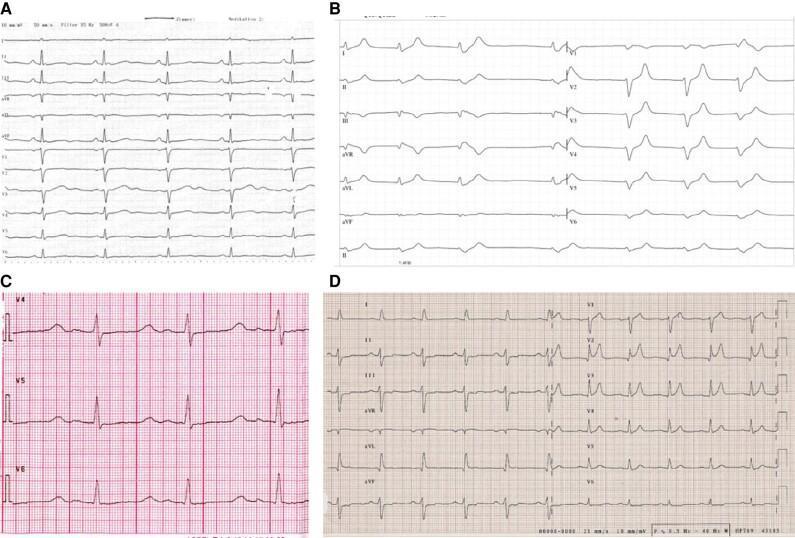
CASE 17 — Dilated Cardiomyopathy: AF + Complete AV Block + CRTD
Clinical scenario: 55M, LMNA mutation, heart failure, syncope, complex arrhythmias
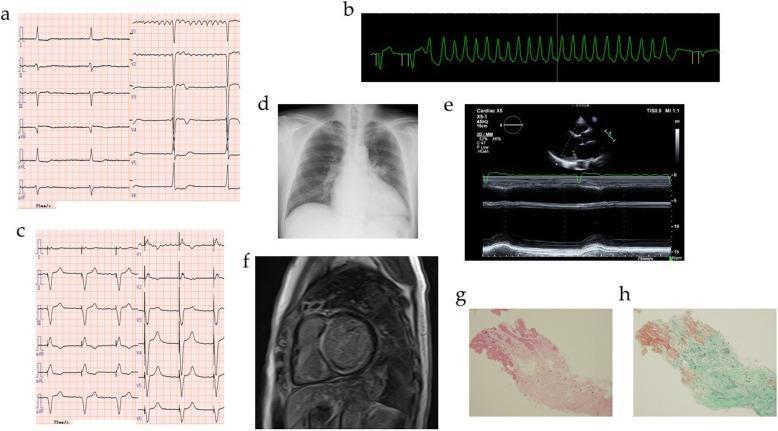
ECG Findings (Panels a–c):
- Panel a: AF + complete AV block (bradycardia 40 bpm)
- Panel b: NSVT (non-sustained VT runs)
- Panel c: Regular paced rhythm after CRTD implantation
Indications for Device Therapy (ICU/Cardiology):
| Device | Indication |
|---|---|
| Pacemaker | Symptomatic bradycardia, AV block |
| ICD | EF <35%, VT/VF survivor |
| CRT-D | EF <35%, LBBB, QRS >150ms, NYHA II–IV |
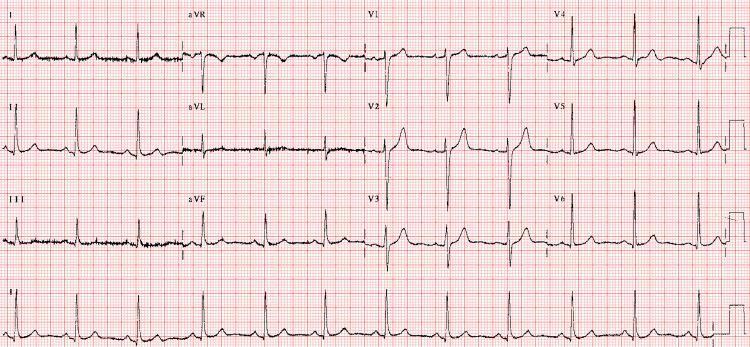
CASE 18 — Atrial Fibrillation with PVC
Clinical scenario: 67M, known AF, single episode of sudden hard beat
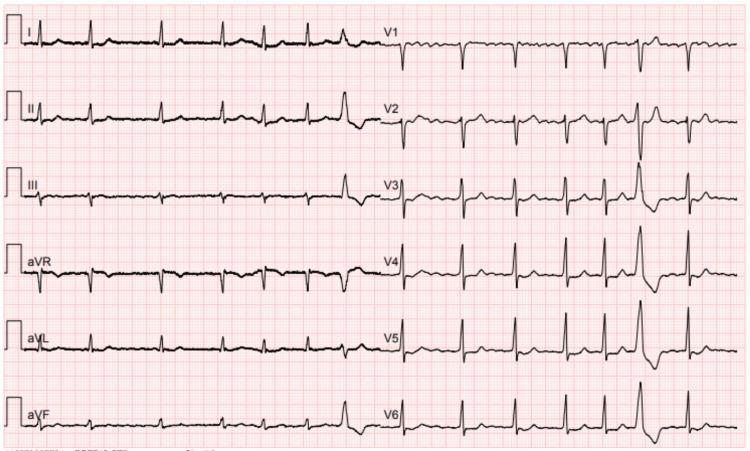
ECG Findings:
- AF baseline: Irregular rhythm, no P waves, fine fibrillatory waves (inferior leads, V1)
- Narrow QRS majority (normal conduction)
- Single wide, bizarre QRS at end = PVC (premature ventricular complex)
- Compensatory pause after PVC
- T waves concordant with QRS
PVC on ECG — Identification:
Wide QRS >120ms, bizarre morphology, no preceding P wave, compensatory pause = PVC
CASE 19 — AF with RVR (Rapid Rate, Fine Fibrillation)
Clinical scenario: Thyrotoxicosis, 40F, palpitations, HR 123, tremors
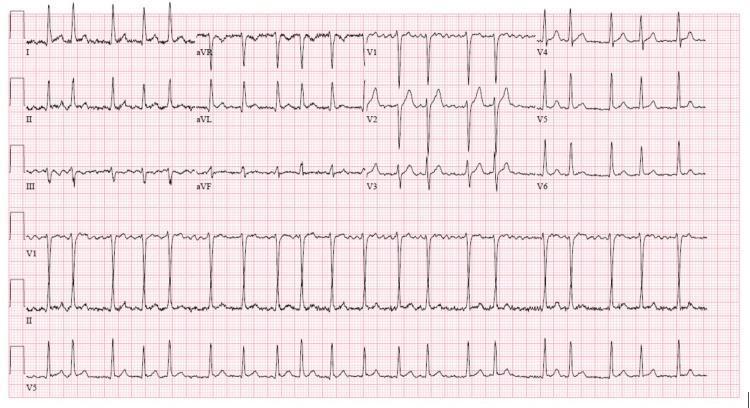
ECG Findings:
- Irregularly irregular rhythm, HR ~123 bpm
- No P waves — undulating fibrillatory (f) waves in V1 baseline
- Narrow QRS (<120ms) — normal conduction
- No ST changes suggesting acute ischemia
Thyrotoxicosis + AF Treatment:
- Beta-blocker (propranolol preferred — also controls thyroid symptoms)
- Digoxin (less effective in high-adrenergic states)
- Carbimazole/PTU for hyperthyroidism
- Cardioversion only after euthyroid state achieved
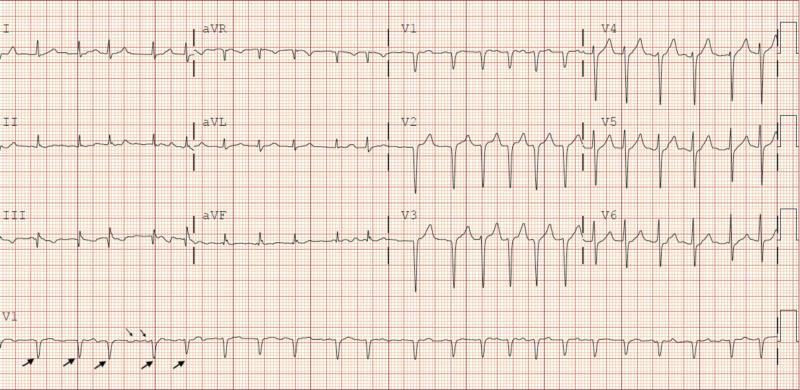
CASE 20 — AF with Auto-Interpretation (Outpatient Telemetry)
Clinical scenario: 70M, remote cardiac monitoring, detected abnormal rhythm
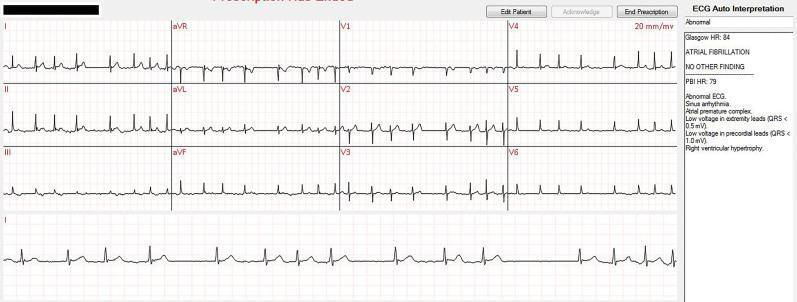
ECG Findings:
- AF — absent P waves, irregularly irregular
- RVH (right ventricular hypertrophy) — reported by auto-interpretation
- HR: 79–84 bpm
- Clinical correlation required — auto-interpretation is a screening tool only
🟡 OPD-LEVEL CASES (Cases 21–40)
CASE 21 — Sinus Tachycardia
Clinical scenario: 28F, anxiety, HR 110, chest pain
ECG Findings:
- Rate: >100 bpm
- P wave: Present, upright in II, inverted in aVR
- PR interval: Normal
- QRS: Narrow, normal
- Rhythm: Regular
Causes (FLATED):
- Fever, Low BP (hypovolemia), Anemia, Thyroid (↑), Emotion/pain, Drugs (salbutamol, caffeine)
Treatment:
- Treat underlying cause
- Beta-blocker if symptomatic (anxiety, thyrotoxicosis)
CASE 22 — Sinus Bradycardia
Clinical scenario: 50M athlete, HR 48, asymptomatic
ECG Findings:
- Rate: <60 bpm
- P wave: Normal, present before each QRS
- Rhythm: Regular
- QRS: Narrow
Causes:
- Athlete's heart, hypothyroidism, inferior MI, beta-blockers, vagal tone, hypothermia
Treatment:
- Asymptomatic + athlete → reassure
- Symptomatic: Atropine 0.5mg IV, consider pacemaker
CASE 23 — First-Degree AV Block
Clinical scenario: 65M, routine ECG, on beta-blocker
ECG Findings:
- PR interval: >0.20s (>1 large square = >200ms)
- All P waves conducted
- Normal QRS (narrow)
- Rate: Normal
Causes:
- Beta-blockers, digoxin, inferior MI, Lyme disease, elderly/fibrosis
Treatment:
- Usually benign, no treatment
- Stop offending drug if symptomatic
CASE 24 — Second-Degree AV Block Mobitz Type I (Wenckebach)
Clinical scenario: 55M, inferior MI, progressive PR prolongation then dropped beat
ECG Findings:
- Progressive PR lengthening until one P wave NOT followed by QRS
- Grouped beating pattern
- Narrowing R-R before dropped beat
Memory Aid:
"Longer, longer, longer — DROP, then shorter" = Wenckebach
Treatment:
- Often benign (especially in inferior MI — usually reversible)
- Atropine if symptomatic
- Temporary pacemaker if persistent/symptomatic
CASE 25 — Second-Degree AV Block Mobitz Type II
Clinical scenario: 60F, anterior MI, sudden syncope
ECG Findings:
- Constant PR interval — suddenly a P wave not followed by QRS
- No warning (unlike Wenckebach)
- Often with wide QRS (infranodal block)
- 2:1, 3:1 conduction ratios may occur
Key Difference:
| Feature | Mobitz I | Mobitz II |
|---|---|---|
| PR before drop | Progressively longer | Constant |
| QRS width | Narrow | Usually wide |
| Location | AV node | Bundle of His/branches |
| Risk | Low | HIGH — may progress to CHB |
Treatment:
- Requires pacemaker (high risk of complete heart block)
CASE 26 — Left Bundle Branch Block (LBBB)
Clinical scenario: 72M, dyspnea, newly discovered LBBB
ECG Findings:
- QRS >120ms (wide)
- V1: QS or rS (W-shaped)
- V6, I, aVL: Broad, notched R wave, no Q or S wave
- Lead I: Broad M-shaped R
- Concordant ST/T changes (ST/T opposite to QRS direction = normal for LBBB)
Clinical Significance:
New LBBB + chest pain = STEMI equivalent (Sgarbossa criteria) → treat as STEMI!
Sgarbossa Criterion 1: ST elevation >1mm concordant with QRS = very specific for MI
Treatment:
- If new LBBB + symptoms: urgent cardiology
- Old LBBB: investigate for cardiomyopathy, CAD
- Symptomatic + EF<35% + QRS>150ms: CRT consideration
CASE 27 — Right Bundle Branch Block (RBBB)
Clinical scenario: 45M, routine pre-op ECG
ECG Findings:
- QRS >120ms
- V1: rsR' (M or "rabbit ears" pattern)
- V6, I: Broad S wave (slurred)
- T inversions V1–V3 (secondary — normal)
Causes:
- Normal variant (isolated RBBB common)
- PE, RV pressure overload, ASD, ischemia, Brugada syndrome
Treatment:
- Isolated RBBB without symptoms: no treatment
- Investigate for PE if new onset + dyspnea
CASE 28 — Left Ventricular Hypertrophy (LVH)
Clinical scenario: 55F, hypertension 10 years, ECG for assessment
ECG Findings:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 >35mm
- Cornell criteria: R in aVL >11mm, or S in V3 + R in aVL >20mm (F) / >28mm (M)
- ST depression + T inversion in I, aVL, V5–V6 (strain pattern)
- Left axis deviation
Memory Aid:
"Deep S in V1 + Tall R in V5/V6" = LVH
Treatment:
- Aggressive BP control (target <130/80)
- ACE inhibitor / ARB (best for LVH regression)
- Lifestyle modification
CASE 29 — Right Ventricular Hypertrophy (RVH)
Clinical scenario: 32F, pulmonary arterial hypertension
ECG Findings:
- Tall R in V1 (R>S in V1)
- Deep S in V5, V6, I (right axis deviation >+90°)
- T inversion V1–V3 (strain)
- P pulmonale: Peaked P wave >2.5mm in II, III, aVF (RA enlargement)
Causes:
- PAH, COPD, MS, ASD, VSD, Tetralogy of Fallot
Treatment:
- Treat underlying cause
- PAH: phosphodiesterase inhibitors, prostacyclin, endothelin antagonists
CASE 30 — Wolff-Parkinson-White (WPW) Syndrome
Clinical scenario: 22M, recurrent palpitations, HR 200 during episode
ECG Findings (Baseline):
- Short PR interval <120ms
- Delta wave: Slurred initial upstroke of QRS
- Wide QRS (>120ms due to delta wave)
- Pseudo-ST changes and T-wave changes (secondary)
WPW Quick Identification:
"Short PR + Wide QRS + Delta wave" = WPW
Danger:
WPW + AF = Most dangerous combination. Accessory pathway conducts fast → VF!
Never give AV nodal blockers (Adenosine, Verapamil, Diltiazem, Digoxin) in WPW+AF → may cause VF!
Treatment:
- SVT in WPW: Adenosine (if no AF), Procainamide/Flecainide
- WPW + AF: DC cardioversion or Procainamide IV
- Definitive: Radiofrequency ablation of accessory pathway (curative ~95%)
CASE 31 — Supraventricular Tachycardia (SVT / AVNRT)
Clinical scenario: 30F, sudden onset palpitations, HR 180, abrupt start and stop
ECG Findings:
- Rate: 150–250 bpm
- Regular narrow complex tachycardia
- P waves: Hidden in QRS or just after QRS (retrograde P)
- No visible P wave before QRS
Vagal Maneuvers:
Carotid sinus massage, Valsalva, ice-water face immersion → may terminate SVT
Treatment:
- Vagal maneuvers first
- Adenosine 6mg IV rapid push (flush with 20mL saline) → if no response: 12mg
- Verapamil 5mg IV (if no WPW, no hypotension)
- DC cardioversion if hemodynamically unstable
- Long-term: Beta-blocker, flecainide, or catheter ablation
CASE 32 — Atrial Flutter
Clinical scenario: 58M, palpitations, HR 150 regular
ECG Findings:
- Sawtooth baseline (flutter waves) — best in II, III, aVF
- Atrial rate: ~300 bpm
- 2:1 block most common → ventricular rate ~150 bpm
- Regular rhythm (unless variable block)
- No isoelectric baseline between flutter waves
Memory Aid:
"Regular HR of 150 in older patient" = Think flutter 2:1 block
Treatment:
- Rate control: Beta-blocker, Diltiazem, Digoxin
- Cardioversion: Synchronized DC shock (low energy 50–100J — very responsive)
- Ablation: Cavotricuspid isthmus ablation (highly effective, >95% cure)
- Anticoagulation similar to AF
CASE 33 — Premature Ventricular Complexes (PVCs)
Clinical scenario: 45M, occasional irregular heartbeat, otherwise healthy
ECG Findings:
- Premature, wide QRS (>120ms)
- No preceding P wave
- Compensatory pause after PVC
- Bizarre morphology — different from sinus beats
- T wave opposite to QRS direction
Benign vs Malignant PVCs:
| Feature | Benign | Malignant |
|---|---|---|
| Frequency | <10/hr | Frequent, runs |
| Pattern | Isolated | Couplets, VT runs |
| Setting | No heart disease | Post-MI, low EF |
| R-on-T | Absent | Present |
Treatment:
- Isolated PVCs, no structural disease: reassure, avoid caffeine/alcohol
- Frequent symptomatic PVCs: Beta-blocker
- PVCs >10,000/day causing cardiomyopathy: ablation
CASE 34 — Pericarditis
Clinical scenario: 25M, sharp pleuritic chest pain, fever, pericardial rub
ECG Findings (4 Stages):
| Stage | ECG Change | Timing |
|---|---|---|
| I | Diffuse concave ST elevation (saddle-shaped), PR depression | Days 1–2 |
| II | ST normalizes, T-wave flattening | Days 3–7 |
| III | T-wave inversions globally | Weeks |
| IV | ECG normalizes | Months |
Pericarditis vs STEMI Differentiation:
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST elevation | Diffuse, concave (saddleback) | Focal, convex |
| Reciprocal changes | Absent (except aVR) | Present |
| PR depression | Present (pathognomonic) | Absent |
| Q waves | Absent | Develop |
| Distribution | All leads | Coronary territory |
Treatment:
- NSAIDs (Ibuprofen 600mg TID or Aspirin 750–1000mg TID) for 1–2 weeks
- Colchicine 0.5mg BD × 3 months (reduces recurrence)
- Avoid anticoagulants (risk of hemorrhagic tamponade)
- Steroids only if recurrent/refractory
CASE 35 — Early Repolarization Syndrome
Clinical scenario: 28M athlete, routine ECG, no symptoms, J-point elevation found
ECG Findings:
- J-point elevation ≥1mm with concave ST elevation
- Notching/slurring at terminal QRS
- Best seen in lateral leads (V4–V6)
- No reciprocal changes
- Tall peaked T waves
Early Repolarization vs STEMI:
Early repolarization: concave, benign, young athletes
STEMI: convex, focal territory, reciprocal changes, symptoms
Management:
- Young athlete, no symptoms: reassure
- If associated with VF/cardiac arrest → ICD implantation (rare, malignant form)
CASE 36 — Digitalis (Digoxin) Toxicity
Clinical scenario: 75F, on digoxin for AF, now bradycardia + nausea + xanthopsia
ECG Findings:
- "Salvador Dali moustache" / Reverse tick: ST segment scooping/sagging (typical digoxin effect — not toxicity per se)
- PR prolongation
- Regularization of AF (AV block increasing)
- Bidirectional VT (pathognomonic for severe toxicity)
- Various arrhythmias: PAT with block, junctional rhythms, AV blocks
Digoxin ECG Effects vs Toxicity:
| Effect (therapeutic) | Toxicity |
|---|---|
| ST scooping | Bidirectional VT |
| PR prolongation | PAT with AV block |
| T flattening | Complete AV block |
Treatment:
- Digoxin immune Fab (Digibind) — specific antidote
- Treat hyperkalemia (worsens toxicity)
- Temporary pacemaker for severe bradycardia
- Avoid cardioversion (induces VF in digoxin toxicity)
CASE 37 — Hypothermia
Clinical scenario: 72M, found unconscious outdoors in winter, temp 28°C
ECG Findings:
- Osborn (J) waves: Positive deflection at J-point (junction of QRS and ST) — pathognomonic!
- PR prolongation, QRS widening
- Prolonged QT
- Bradycardia
- AF common
- Shivering artifact
Temperature Correlation with ECG:
| Temp | ECG |
|---|---|
| <35°C | Sinus bradycardia |
| <32°C | Osborn waves, AF |
| <30°C | VF risk |
| <28°C | Asystole risk |
Treatment:
- Passive rewarming (mild) / Active rewarming (severe)
- VF in hypothermia: defibrillate (may need multiple attempts as temp rises)
- Warm IV fluids, warm humidified O2
- ECMO for refractory hypothermic cardiac arrest
CASE 38 — Brugada Syndrome
Clinical scenario: 38M, syncope during sleep, family history of sudden death
ECG Findings:
- Type 1 (diagnostic): Coved ST elevation ≥2mm in V1–V2, followed by negative T wave — "shark fin" pattern
- Type 2: "Saddle-back" ST elevation in V1–V2
- Type 3: <1mm ST elevation
- RBBB-like pattern
Brugada vs Normal RBBB:
Normal RBBB: rsR' in V1 with descending ST
Brugada: rsR' with elevated ST going up then coved (like a shark fin/dome shape)
Treatment:
- ICD (only proven effective treatment)
- Avoid sodium channel blockers (flecainide, procainamide, ajmaline — can unmask)
- Quinidine (adjunct)
- Avoid fever (worsens Brugada pattern — paracetamol for fever)
CASE 39 — Long QT Syndrome (Congenital)
Clinical scenario: 16F, exercise-induced syncope, mother had sudden death
ECG Findings:
- QTc >440ms (men), >460ms (women) = prolonged
- QTc >500ms = high risk
- Abnormal T-wave morphology: bifid T, broad T, notched T
QT Calculation:
QTc = QT ÷ √R-R interval (Bazett formula)
Quick tip: At 60 bpm, QT should be <440ms; at 100 bpm, <380ms
Causes:
- Congenital: LQT1 (K channel, exercise-triggered), LQT2 (K channel, emotional/auditory trigger), LQT3 (Na channel, sleep/rest-triggered)
- Acquired: Drugs, electrolytes (see Case 9)
Treatment:
- Beta-blocker (especially LQT1, LQT2)
- ICD if high risk, prior cardiac arrest
- Avoid QT-prolonging drugs
- Mexiletine for LQT3
- Genetic counseling, family screening
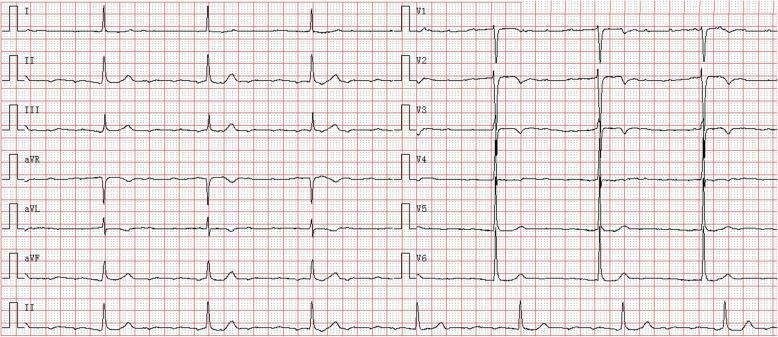
CASE 40 — Normal Sinus Rhythm (Reference)
Clinical scenario: 30F, routine health check, no complaints
ECG Findings — Normal Values:
| Parameter | Normal |
|---|---|
| Rate | 60–100 bpm |
| Rhythm | Regular |
| P wave | Upright II, inverted aVR; <0.12s, <2.5mm |
| PR interval | 0.12–0.20s (3–5 small squares) |
| QRS | <0.12s (<3 small squares) |
| QRS axis | −30° to +90° (I and aVF both positive) |
| ST segment | Isoelectric ±0.5mm |
| T wave | Upright I, II, V3–V6; inverted aVR, V1 |
| QTc | <440ms men, <460ms women |
| U wave | Small, upright, <1mm |
📊 QUICK REFERENCE SUMMARY TABLE
| # | Condition | Rate | Rhythm | Key ECG Feature | First Treatment |
|---|---|---|---|---|---|
| 1–4 | STEMI variants | Variable | Sinus | ST elevation (territory-specific) | PCI / Thrombolysis |
| 5 | AF with RVR | >100 | Irreg. irreg. | No P waves | Metoprolol IV / Cardioversion |
| 6 | AF + CHB | 40–43 | Slow regular | AF + AV dissociation | Temporary pacemaker |
| 7 | CHB + VT | Varies | Dissociated | P-QRS dissociation + wide VT | Pacing + Amiodarone |
| 9 | TdP | Varies | Irregular | Twisting QRS | MgSO₄ 2g IV |
| 10–11 | PE | >100 | Sinus | S1Q3T3 + RV strain | Heparin / Thrombolysis |
| 12 | Hyperkalemia | Slow | Sinus | Peaked T waves | Ca gluconate IV |
| 14 | Hypokalemia | Normal | Sinus | Flat T + U waves | KCl replacement |
| 26 | New LBBB | Normal | Sinus | Wide QRS, W in V1 | Treat as STEMI |
| 30 | WPW | 200 | Regular | Short PR + delta wave | RF ablation |
| 31 | SVT | 150–250 | Regular | Narrow regular, no P | Adenosine 6mg IV |
| 32 | Atrial flutter | 150 | Regular | Sawtooth waves | Cardioversion/ablation |
| 34 | Pericarditis | Normal | Sinus | Diffuse concave ST + PR dep | NSAIDs + Colchicine |
| 37 | Hypothermia | Slow | AF/sinus | Osborn J waves | Rewarming |
| 38 | Brugada | Normal | Sinus | Coved ST V1–V2 | ICD |
| 39 | Long QT | Normal | Sinus | QTc >460ms | Beta-blocker |
🧠 ECG DEKHNE KA SHORTCUT (Bedside Mnemonic)
"RRAPQRST"
- Rate — fast/slow/normal?
- Rhythm — regular/irregular?
- Axis — normal/left/right deviation?
- P waves — present? morphology? PR interval?
- QRS — width? pathological Q?
- R wave — progression V1→V6?
- ST segment — elevation/depression?
- T waves — upright/inverted? peaked?
Note: All ECG images are from peer-reviewed clinical literature. Always correlate ECG findings with clinical history, examination, and laboratory values. This guide is for educational purposes; management should follow current institutional and international guidelines (ACC/AHA/ESC).
This is a shared conversation. Sign in to Orris to start your own chat.