My case is chronic unreduced posterolateral elbow disslocation but ucl and annular ligament with reduction was done why lucl is not repaired here
"elbow dislocation" AND "lateral ulnar collateral ligament" AND repair
chronic posterolateral elbow dislocation LUCL repair vs UCL annular ligament reconstruction surgical rationale
https://cdn.mdedge.com/files/s3fs-public/Document/September-…
Why Was the LUCL Not Repaired in Your Case of Chronic Posterolateral Elbow Dislocation?
The Short Answer
Anatomy and Role of the LUCL
- Originates on the posterior lateral epicondyle
- Inserts on the crista supinatoris of the proximal ulna
- Is the primary restraint to posterolateral rotatory instability (PLRI)
- Incompetence of the LUCL leads to PLRI - the ulna externally rotates on the trochlea with posterior subluxation of the radial head
Why LUCL Repair Is Different from LUCL Reconstruction
- The LUCL is usually avulsed from the lateral epicondyle with collagen fibers largely intact
- Primary repair back to the humeral origin is feasible and successful
- Tissue quality is acceptable for suture anchor reattachment
- The LUCL has retracted, scarred, and lost structural integrity
- There is no identifiable native ligament tissue suitable for direct repair
- The chronic dislocation creates abundant hypertrophic scar tissue that replaces the original ligament anatomy - making primary repair technically impossible
- The web-extracted operative case report confirms: in a 6-week-old chronic dislocation, surgeons found "no lateral ligamentous complex identifiable" - they had to reconstruct the LUCL using a split semitendinosus allograft in a figure-of-8 technique
Why UCL and Annular Ligament Were Repaired Instead
- Relocate and stabilize the radial head concentrically
- Prevent recurrent radial head instability
- Restore normal proximal radioulnar joint kinematics
What Happened to the LUCL Then?
| Scenario | Explanation |
|---|---|
| Stability achieved without LUCL reconstruction | After UCL repair + annular ligament repair + reduction, intraoperative fluoroscopy showed concentric, stable reduction. If the elbow was stable through full ROM intraoperatively, separate LUCL reconstruction was not added (adds surgical time and graft harvest morbidity). |
| LUCL was not identifiable | As noted above, in chronic cases the LUCL tissue is often indistinguishable from scar tissue. |
| LUCL reconstruction deferred | Some surgeons stage the procedure - establish reduction and bony stability first, then address ligamentous insufficiency in a second stage if PLRI symptoms persist. |
| IJS or external fixation used as substitute | Campbell's 2026 notes that the internal joint stabilizer (IJS) device "largely supplanted the need" for ligament reconstruction in chronic dislocations, because it maintains concentric reduction while soft tissues heal. |
Key Principle: Stability Hierarchy in Elbow Dislocation
- Bony stability (coronoid, radial head - if fractured)
- LUCL (lateral complex - first injured, repaired/reconstructed first)
- UCL (medial complex - repaired only if instability persists after lateral repair)
- The primary goal shifts to achieving reduction (requires extensive soft tissue release, scar debridement, possible V-Y triceps lengthening)
- After reduction is achieved, intraoperative stability assessment determines what ligamentous work is added
- The UCL and annular ligament may be repairable tissue; the LUCL typically is not - hence LUCL reconstruction (not repair) would be the correct term if it were performed
Summary
- In a chronic dislocation, the LUCL tissue is non-viable - fibrosed, retracted, or absent - making primary repair impossible
- What the LUCL would need is reconstruction with a tendon graft (e.g., semitendinosus, palmaris longus)
- If the elbow was stable after UCL repair + annular ligament repair, the surgeon may have judged LUCL reconstruction unnecessary at that stage
- The UCL and annular ligament were chosen for repair because repairable tissue was available on the medial side and at the radial head
No triceps fascia was used for anular ligament
annular ligament reconstruction triceps fascia elbow dislocation technique Bell Tawse
Annular Ligament Reconstruction Using Triceps Fascia: The Bell-Tawse Technique
What Was Done in Your Case
- The native annular ligament is destroyed, non-repairable, or absent (as in chronic dislocations)
- The radial head needs to be stabilized in its reduced position around the capitellum and proximal radioulnar joint
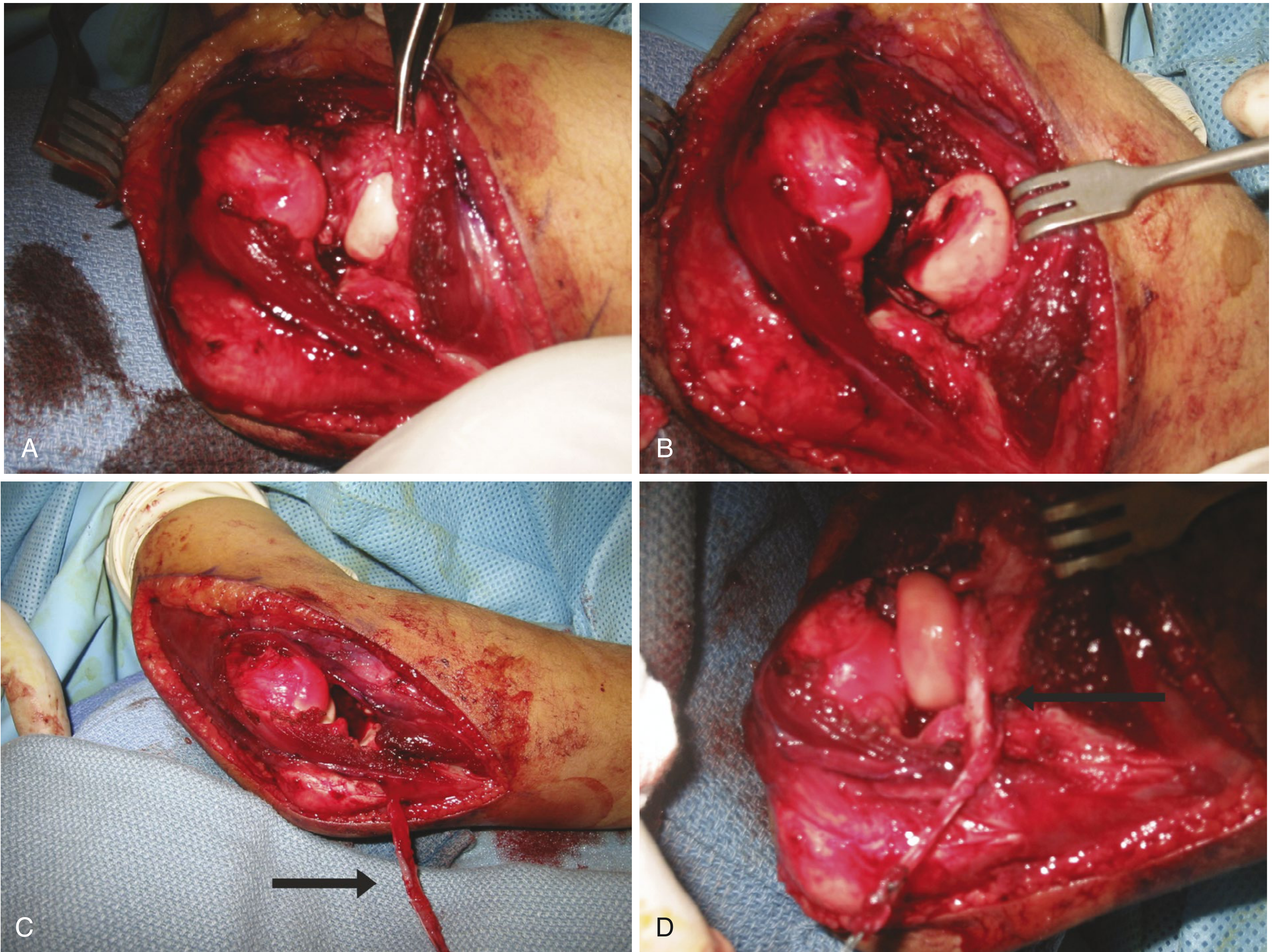
"The triceps fascia has been harvested (C, arrow) and is used to reconstruct the annular ligament (D)."
The Bell-Tawse Technique: How It Works
- Posterolateral approach to the elbow
- Excision of fibrous/capsular block interposed in the radiocapitellar joint
- A longitudinal strip of triceps tendon/fascia is harvested - left attached at its ulnar insertion distally
- The strip is passed around the neck of the radius from behind forward
- Secured through a drill hole in the ulna, creating a neo-annular ligament that encircles the radial neck
- It is in the same operative field - no second incision or donor site needed
- The lateral strip has a rolled edge and is more substantial than a central strip
- It avoids the morbidity of fascia lata harvest from the thigh
- It provides adequate tensile strength to maintain radial head reduction
Now - Why Was the LUCL Still Not Repaired?
| Structure | Function | What Instability It Prevents |
|---|---|---|
| Annular ligament | Keeps radial head in proximal radioulnar joint | Radial head subluxation / proximal radioulnar instability |
| LUCL | Keeps ulna from rotating posterolaterally on humerus | Posterolateral rotatory instability (PLRI) of whole forearm-ulna unit |
- In chronic dislocation, the LUCL tissue is fibrosed and non-viable - primary repair is impossible
- LUCL reconstruction requires a separate graft (palmaris longus, semitendinosus, or gracilis) passed through drill holes in the lateral epicondyle and crista supinatoris - a distinct additional procedure
- If intraoperative stability was adequate after annular ligament reconstruction + UCL repair + reduction (confirmed by fluoroscopy), the surgeon may have judged LUCL reconstruction unnecessary at that stage to avoid additional surgical complexity
- Some surgeons intentionally defer LUCL reconstruction and reassess for PLRI symptoms at 3-6 months postoperatively - if PLRI persists, a staged LUCL reconstruction is then performed
Summary
- The triceps fascia was used to reconstruct the annular ligament (Bell-Tawse type procedure) - this stabilizes the radial head in the proximal radioulnar joint
- The UCL was repaired medially to restore valgus stability
- The LUCL addresses a completely different plane of instability (posterolateral rotatory) and requires its own reconstruction with a tendon graft through bone tunnels
- In your chronic case, the LUCL was either non-repairable (no viable tissue), or stability was deemed sufficient after the other repairs, or LUCL reconstruction was deferred for reassessment
- If postoperative PLRI (positive lateral pivot-shift test, apprehension with supination-valgus loading) is present, a staged LUCL reconstruction with tendon autograft would be the next step
But it was potserolateral dislocation lcl should have been repaired right
chronic unreduced posterolateral elbow dislocation LCL LUCL not repaired reasons instability management
You Are Right - The LUCL Should Have Been Addressed
The Pathoanatomy Confirms Your Point
- Stage 1 - LCL/LUCL disrupted first (the initiating lesion)
- Stage 2 - anterior and posterior capsule torn, radial head subluxates
- Stage 3 - complete dislocation, MCL also disrupted
What the Literature Actually Says
"It is generally accepted that the LUCL should be repaired or reconstructed if the injury is being treated surgically or if there is chronic symptomatic elbow instability." (Schreiber MD, J Hand Surg 2014)
- LCL repair always first
- MCL repair only if instability persists after LCL is fixed
- Miller's states: "Lateral ligamentous complex always repaired, followed rarely by MCL if instability persists" (p. 2514)
- Primary repair may not be possible (tissue quality)
- But LUCL reconstruction with tendon graft is indicated
- Morrey and Sanchez-Sotelo specifically state: in the chronic setting, "tendon graft reconstruction" is recommended over simple repair
Why Skipping LUCL in Your Case Is Questionable
- UCL was repaired (medial side)
- Annular ligament was reconstructed with triceps fascia (radial head stabilized)
- LUCL was not repaired or reconstructed
- Leaves the primary instability driver (LUCL) unaddressed
- Creates an asymmetric repair - medial side tightened, lateral side still deficient
- Risks persistent PLRI postoperatively - the ulna will still posterolaterally rotate on the humerus
- The annular ligament repair (triceps fascia) only stabilizes the radial head in the proximal radioulnar joint - it does not substitute for LUCL function
Possible Justifications the Surgeon May Have Had
| Justification | Validity |
|---|---|
| No identifiable LUCL tissue in chronic case | Valid - if no tissue was present, reconstruction (not just repair) with a graft was needed |
| Intraoperative stability was adequate after UCL + annular ligament repair | Partially valid - if fluoroscopy showed concentric reduction stable through full ROM in pronation, some surgeons accept this |
| Planned staged LUCL reconstruction if PLRI persists | Valid as a deliberate strategy - though it requires follow-up |
| Relying on the IJS device or external fixator to protect while healing | Valid if a stabilizing device was used |
The Bottom Line
- In posterolateral dislocation, the LCL/LUCL is the first and primary structure injured
- When operating on such a dislocation (acute or chronic), the LCL complex is repaired/reconstructed first
- The UCL is only addressed if instability persists after LCL fixation
- Lateral pivot-shift test - supination + valgus + axial load as elbow flexes
- Chair push-up test - forearm supinated, arms push up from chair
- Table-top relocation test
No but i shoud defend that surgeon was right how to give it very shortly