Uv organ prolapse
Reading File
Finding Sources
Searching PubMed
"pelvic organ prolapse" management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content to deliver a full answer. Let me compile it.
Uterovaginal (Pelvic Organ) Prolapse
Definition
Pelvic organ prolapse (POP) refers to the protrusion or displacement of one or more pelvic organs from their normal anatomical position into or through the vagina. It affects up to 40% of women at some point in their lifetime and can impair anorectal, urinary, and sexual function.
Bailey and Love's Short Practice of Surgery, 28th Ed., p.1611
Anatomy: Types of Prolapse
The prolapse is classified by which organ/compartment herniates:
| Type | Structure Involved | Direction |
|---|---|---|
| Urethrocele | Urethra | Anterior wall |
| Cystocele | Bladder | Anterior wall |
| Cystourethrocele | Bladder + Urethra | Anterior wall |
| Uterine prolapse / Procidentia | Uterus | Apical/central |
| Enterocele | Peritoneum + bowel (small intestine) | Posterior/apical |
| Rectocele | Rectum | Posterior wall |
| Vaginal vault prolapse | Vaginal vault (post-hysterectomy) | Apical |
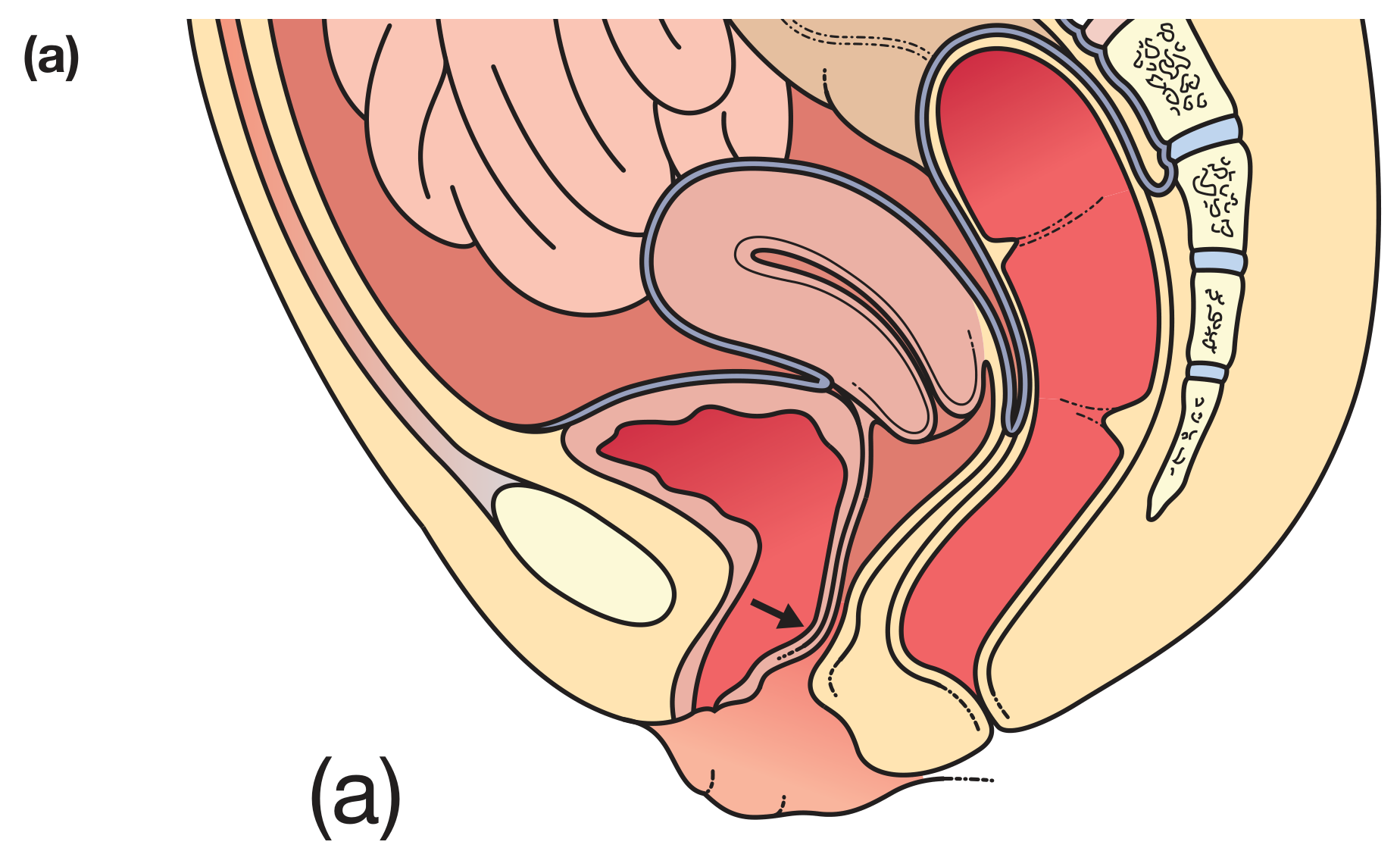
Figure 87.23(a): Urethrocele/Cystocele (arrow) - Bailey & Love
Risk Factors
- Obstetric: Multiparity, prolonged labour, vaginal deliveries
- Age: Postmenopausal women (oestrogen deficiency reduces tissue strength)
- Body: Obesity, chronic constipation, heavy lifting (raised intra-abdominal pressure)
- Connective tissue disorders: Ehlers-Danlos syndrome, Marfan syndrome
- Genetic: Positive family history
Bailey and Love, p.1611
Pathophysiology
The pelvic floor support has three levels (DeLancey's levels):
- Level I (apical) - Uterosacral and cardinal ligaments supporting the uterus/vaginal vault
- Level II (mid-vaginal) - Pubocervical fascia (anterior) and rectovaginal fascia (posterior)
- Level III (distal) - Perineal body and external sphincter complex
Prolapse results from damage to any combination of these levels, through weakening of the pelvic support connective tissue, muscles, and nerves - most commonly from childbirth trauma and oestrogen deficiency.
Berek & Novak's Gynecology, p.1593
Clinical Features (Symptoms)
| Prolapse Type | Symptoms |
|---|---|
| Cystocele/Urethrocele | Lump in vagina, urinary urgency (OAB), stress incontinence, recurrent UTIs |
| Uterine prolapse | Dragging sensation, lump per vagina; in procidentia: vaginal discharge, mucosal ulceration, bleeding |
| Rectocele | Difficulty defecating, incomplete emptying, need to digitally reduce prolapse to defecate (splinting) |
| Enterocele | Pelvic pressure, vaginal protrusion, constipation, sexual dysfunction |
| Vaginal vault | Lump post-hysterectomy, urinary/bowel symptoms |
Minor prolapses may be entirely asymptomatic.
Grading: POP-Q System
The Pelvic Organ Prolapse Quantification (POP-Q) system grades prolapse based on the most distal portion relative to the hymen:
| Grade | Description |
|---|---|
| 0 | No prolapse |
| 1 | Most distal portion >1 cm above hymen |
| 2 | Most distal portion ≤1 cm above or below hymen |
| 3 | Most distal portion >1 cm below hymen but 2 cm less than total vaginal length |
| 4 | Maximal descent (complete procidentia) |
Management
Non-Surgical (Conservative)
- Lifestyle modification: Weight loss, treat constipation, avoid heavy lifting
- Pelvic floor muscle training (PFMT): Physiotherapy for at least 16 weeks - recommended for grade 1 and 2 prolapse
- Topical oestrogen: Improves tissue strength and elasticity in postmenopausal women
- Vaginal pessaries: The ring pessary is most commonly used - inserted between the posterior fornix and pubic bone. Changed every 3-6 months. Complications include vaginal ulceration, infection, discharge and bleeding.
Surgical Management
Surgery aims to restore uterovaginal anatomy. Approach can be vaginal, abdominal (open or laparoscopic).
| Condition | Surgery | Key Complications |
|---|---|---|
| Urethrocele/Cystocele | Anterior colporrhaphy (no mesh) | Bleeding, infection, voiding dysfunction, fistula, occult SUI unmasked |
| Uterine prolapse | Vaginal hysterectomy ± sacrospinous fixation (if family complete); Uterus-preserving: Manchester repair (cervical amputation + cardinal ligament plication), McCall suture (uterosacral ligament plication), Sacrohysteropexy (mesh to sacral promontory) | Bleeding, bladder/bowel/ureter injury, dyspareunia |
| Enterocele | Hernial sac repair via vaginal approach | Bowel injury, recurrence |
| Vaginal vault prolapse | Sacrospinous fixation (vaginal) or Sacrocolpopexy (abdominal/laparoscopic, using mesh) | Right buttock pain, sexual dysfunction, bowel/ureter injury |
| Rectocele | Posterior colpoperineorrhaphy (no mesh) | Dyspareunia, fistula, recurrence |
Note: For women who no longer wish penetrative intercourse, a colpocleisis (vaginal obliteration) can be offered.
Recurrence rate: Approximately 30% of women report symptom recurrence after surgery.
Bailey and Love's Short Practice of Surgery, 28th Ed., p.1612
Special Notes
- Rectocele = herniation of rectal mucosa through a defect in the posterior vaginal fibromuscular wall (can be transverse or longitudinal).
- Enterocele is more common following hysterectomy and retropubic urethropexy.
- Descending perineum syndrome: Perineum descends beyond ischial tuberosities on Valsalva; can cause pudendal neuropathy and is associated with constipation, fecal incontinence, rectocele, and solitary rectal ulcer syndrome.
- Manchester repair is uterus-preserving but carries specific risks: infertility, miscarriage, and dystocia.
Berek & Novak's Gynecology, p.1664
Recent Evidence
Two relevant recent systematic reviews (2025):
- A Cochrane review on perioperative interventions in POP surgery (Shahid et al., Cochrane 2025, PMID 40693510) addresses perioperative care optimization.
- A meta-analysis on hysterectomy and pelvic floor disorders (Chang et al., AJOG 2025, PMID 40120730) shows associations between hysterectomy and subsequent prolapse risk - relevant when counselling patients about uterus-preserving vs. hysterectomy-based repairs.
This is a shared conversation. Sign in to Orris to start your own chat.