ESOPHAGUS anatomy and physiology relevant for Mch Sge
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full MCh Surgery-level answer.
Esophagus: Anatomy and Physiology - MCh Surgery Level
1. Overview and Extent
The esophagus is a muscular conduit extending from the cricoid cartilage (C6 vertebral level) to the cardia of the stomach (T10 vertebral level).
| Landmark | Distance from upper incisors |
|---|---|
| Upper incisors to cricopharyngeus | ~16 cm |
| Upper incisors to aortic arch | ~23 cm |
| Upper incisors to left main bronchus | ~27 cm |
| Upper incisors to diaphragmatic hiatus | ~38 cm |
| Upper incisors to cardia (LES) | ~40 cm |
- Resting lumen diameter: ~20 mm (can distend to 2 cm AP, 3 cm lateral)
- Total length (resting): 18-26 cm
- No serosa - this is a key surgical fact (contributes to anastomotic leak risk and early local tumor spread)
2. Segments and Anatomical Relations
Cervical Esophagus (C6 - Suprasternal notch, ~4-5 cm)
- Anterior: Trachea (left recurrent laryngeal nerve runs in tracheoesophageal groove - at surgical risk during cervical dissection)
- Posterior: Prevertebral fascia and vertebral column
- Lateral: Carotid sheaths and thyroid gland
Thoracic Esophagus (Suprasternal notch - Diaphragm)
- Divided into upper, middle, and lower thirds
- Upper thoracic: passes posterior to trachea, posterior to the left main bronchus
- At T4: crosses posterior to aortic arch
- At T5: crosses posterior to tracheal bifurcation and left main bronchus
- At T8: turns left and crosses anterior to the descending aorta
- At T10: passes through the diaphragmatic hiatus (through the right crus)
Surgical note: The esophagus lies directly on the aorta in its lower thoracic portion - critical in esophagectomy and planning aortic exposure.
Abdominal Esophagus (0.5 - 2.5 cm)
- Anterior: Left lobe of liver
- Right: Caudate lobe of liver
- Left: Fundus of stomach
- Posterior: Right crus of diaphragm and aorta
- Compressed by intraabdominal positive pressure - contributes to LES function
3. Wall Layers (No Serosa - Surgical Significance)
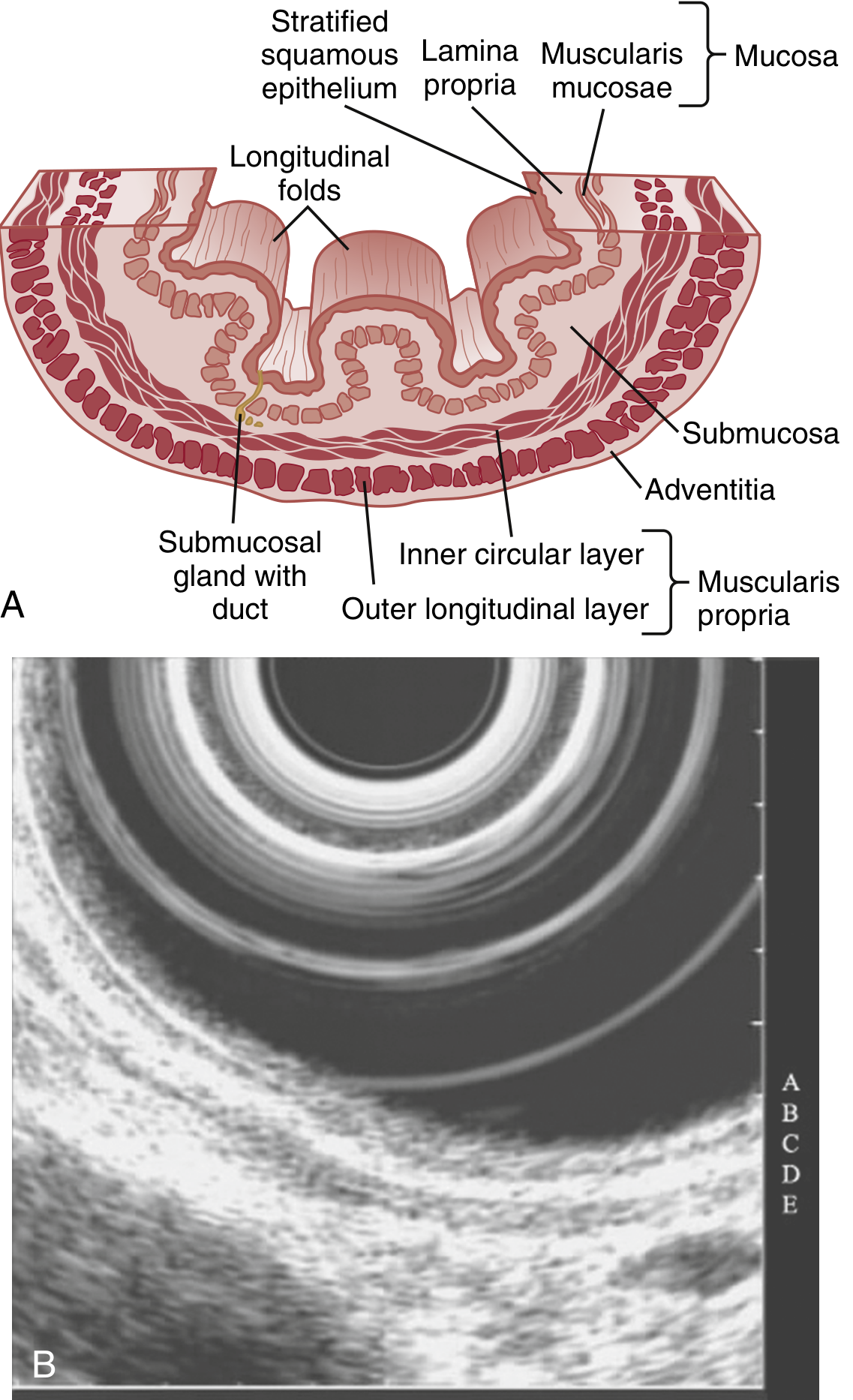
| Layer | Contents | Notes |
|---|---|---|
| Mucosa | Non-keratinized stratified squamous epithelium + lamina propria + muscularis mucosae | 3 sublayers: stratum corneum (permeability barrier), stratum spinosum (metabolically active), stratum germinativum (proliferating basal cells) |
| Submucosa | Dense connective tissue, blood vessels, lymphatics, Meissner plexus, esophageal glands | Most mechanically strong layer - the layer sutured in anastomosis |
| Muscularis propria | Inner circular + Auerbach (myenteric) plexus + outer longitudinal | Striated (upper 1/3), mixed (middle), smooth (lower 2/3) |
| Adventitia | Loose connective tissue only - NO serosa | Allows direct mediastinal spread of cancer |
EUS layers: On EUS, the 5 layers alternate as hyperechoic (A: lumen-mucosa interface, C: submucosa, E: adventitia) and hypoechoic (B: mucosa, D: muscularis propria).
Absence of Serosa - Surgical Implications
- Anastomotic leak rates higher than bowel anastomoses
- Tumor invades mediastinum earlier (T3 = adventitia involvement)
- No natural barrier to prevent local spread
- Requires extra care in anastomotic technique (submucosa is the holding layer)
4. Musculature
| Segment | Muscle type | Innervation |
|---|---|---|
| Upper 1/3 (cervical) | Striated voluntary | Nucleus ambiguus via RLN/vagus |
| Middle 1/3 | Transition zone - striated + smooth | Both nuclei |
| Lower 2/3 | Smooth involuntary | Dorsal motor nucleus of vagus |
- Cricopharyngeus is C-shaped (no posterior midline raphe), attaches to lateral cricoid - this makes the posterior midline the natural weak point (Killian's dehiscence / Zenker's diverticulum).
5. Blood Supply (Segmental, Surgically Critical)
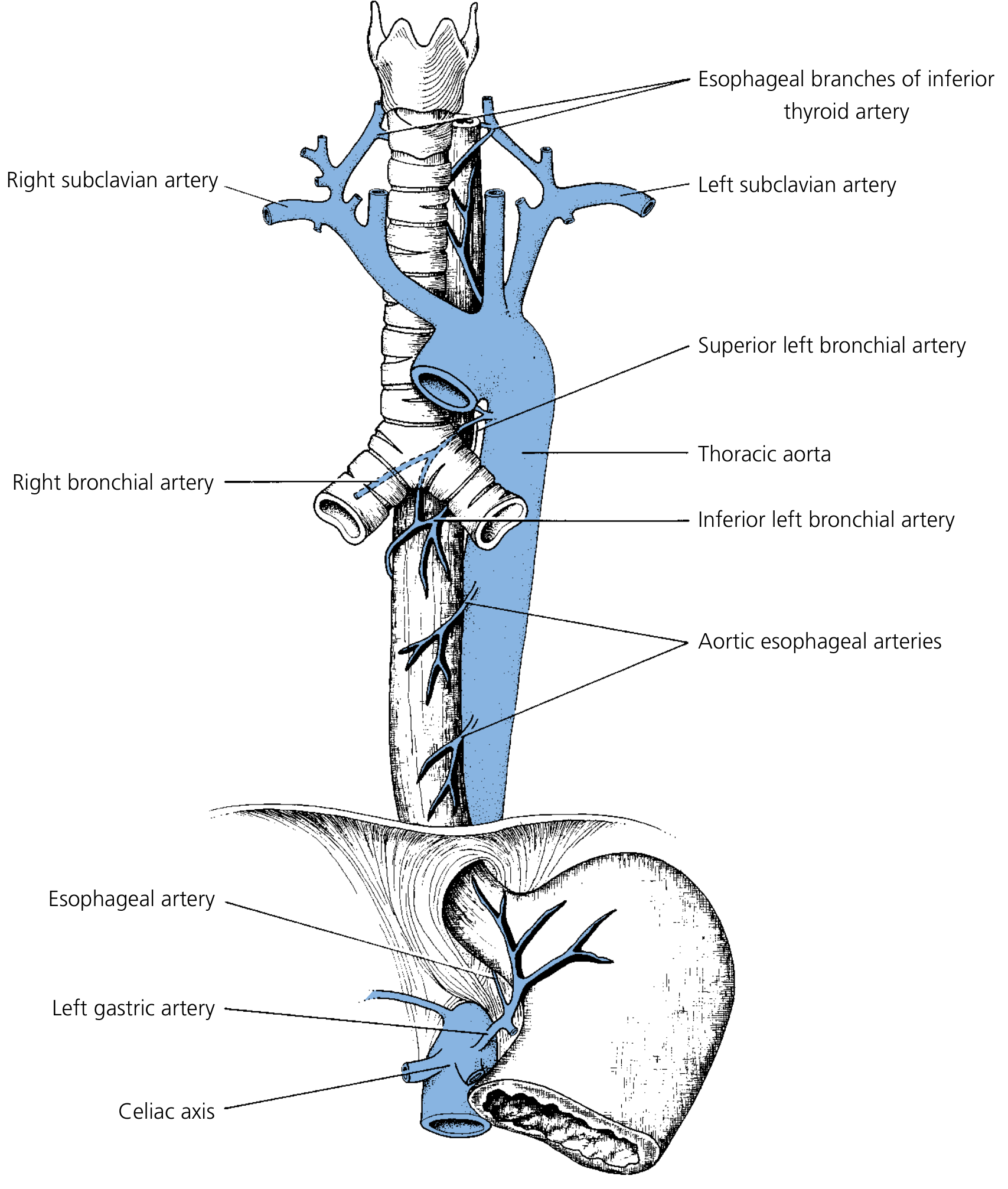
| Segment | Arterial Supply |
|---|---|
| Cervical | Inferior thyroid artery (branches) + contributions from common carotid, subclavian, vertebral, ascending pharyngeal |
| Upper thoracic | Bronchial arteries (right + left), right intercostal arteries |
| Mid/lower thoracic | Direct aortic esophageal arteries (segmental) |
| Abdominal | Left gastric artery (main), left inferior phrenic artery, short gastric arteries |
Surgical significance:
- Blood supply is segmental with limited overlap - esophageal infarction is rare due to submucosal anastomotic network, but devascularization during extensive mobilization risks ischemic anastomotic leak
- The left gastric artery (branch of celiac axis) is the dominant supply to the GEJ - must be preserved when doing Heller myotomy or sacrificed deliberately in esophageal cancer resection with gastric pull-up
6. Venous Drainage
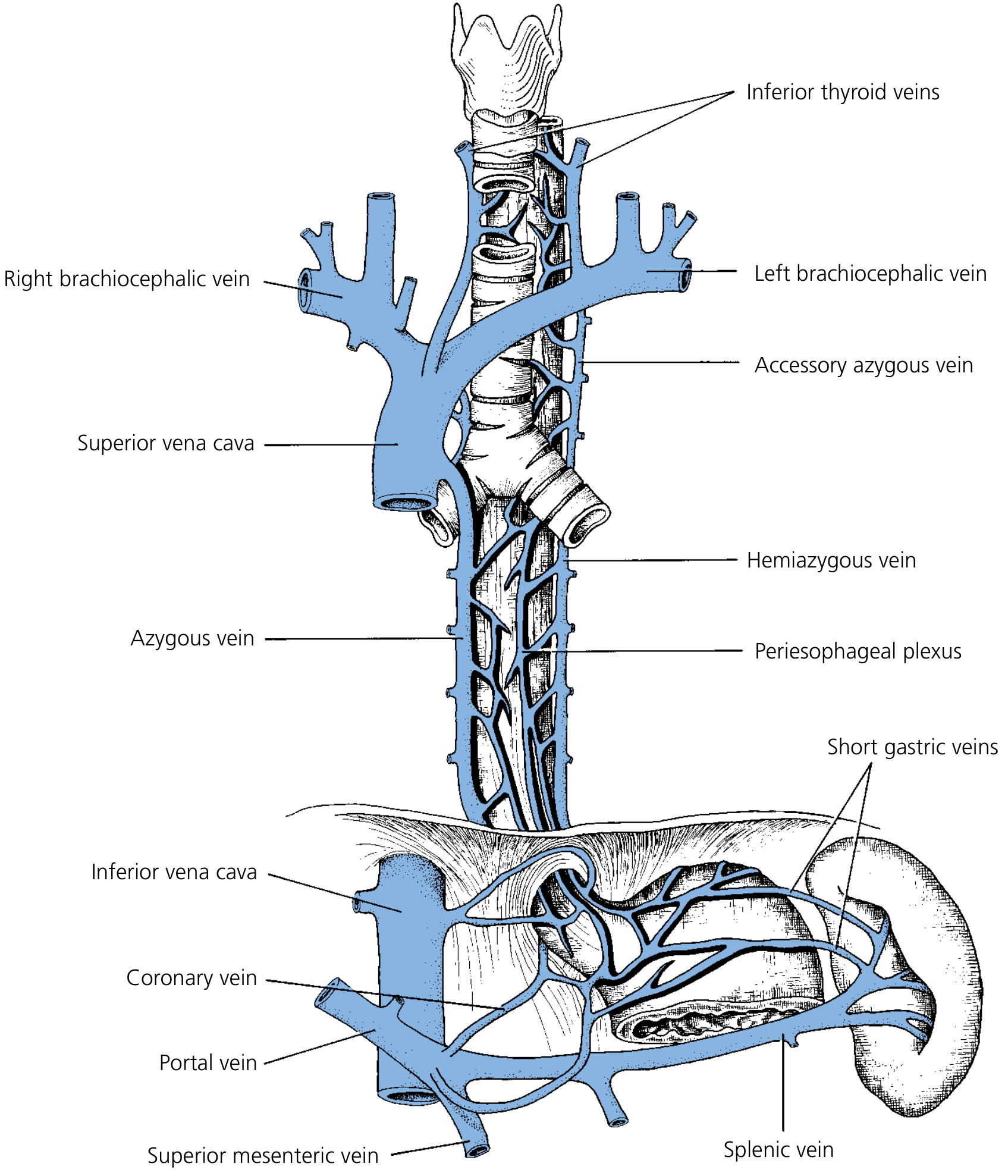
| Segment | Venous Drainage |
|---|---|
| Cervical | Inferior thyroid veins → brachiocephalic veins (systemic) |
| Thoracic (mid) | Azygos vein (right), hemiazygos (left) → SVC (systemic) |
| Distal esophagus / GEJ | Left and short gastric veins → portal vein |
Porto-systemic anastomosis at GEJ - the submucosal venous plexus is a watershed where portal and systemic (azygos) systems communicate. In portal hypertension, back-pressure dilates these submucosal veins → esophageal varices (most common site: 2-5 cm above GEJ). Varices above the level of the aortic arch are called "downhill" varices (from superior vena caval obstruction).
7. Lymphatic Drainage (Non-Segmental - Surgical Significance)
| Segment | Primary lymph nodes |
|---|---|
| Cervical esophagus | Deep cervical (jugular chain) nodes |
| Upper thoracic | Paratracheal, tracheobronchial nodes |
| Mid thoracic | Posterior mediastinal, paraesophageal nodes |
| Lower thoracic / GEJ | Celiac, left gastric (paracardial) nodes |
Critical surgical point: Unlike arterial supply, lymphatic drainage is NOT segmental - there are extensive longitudinal submucosal lymphatic channels running the full length of the esophagus. This explains:
- "Skip lesions" - tumors can spread to nodes far from the primary site
- Most esophageal cancers have lymph node spread beyond the primary region at time of diagnosis
- Need for extended lymphadenectomy (2-field or 3-field) in esophageal cancer resection
8. Nerve Supply
Motor (Vagus - Parasympathetic)
- Nucleus ambiguus (NA): innervates UES and upper esophageal striated muscle via recurrent laryngeal nerves
- Dorsal motor nucleus (DMN): innervates smooth muscle of lower esophagus and LES via esophageal plexus
- At the level of the diaphragm, the esophageal plexus condenses into:
- Anterior vagal trunk (predominantly left vagus) → anterior gastric branches + hepatic branch
- Posterior vagal trunk (predominantly right vagus) → posterior gastric branches + celiac plexus branch
- Vagal rotation: During gut rotation, the left vagus moves anteriorly and the right moves posteriorly (rotate clockwise when viewed from above)
Sympathetic
- Superior cervical ganglion, thoracic sympathetic chain, major splanchnic nerve, celiac ganglion
- Mediates nociception (pain) from the esophagus
Enteric Nervous System
- Meissner plexus (submucosal): parasympathetic ganglia - secretomotor
- Auerbach (myenteric) plexus (between inner circular and outer longitudinal): coordinates peristalsis
Clinical note: Destruction of Auerbach's plexus → achalasia. The RLN (recurrent laryngeal nerve) runs in the tracheoesophageal groove on both sides - at risk during cervical/thoracic esophageal surgery.
9. Sphincters
Upper Esophageal Sphincter (UES)
- Anatomic structures: Cricopharyngeus muscle (primary) + inferior pharyngeal constrictor + thyropharyngeus
- Located at C5-C6 level
- Manometrically: 2-3 cm zone of high pressure
- Resting tone: tonic contraction at ~100 mmHg (prevents air entry during respiration)
- Relaxation: during swallowing - passive by laryngeal elevation opening the sphincter actively
- Cricopharyngeus is a C-shaped muscle (no dorsal raphe) - Killian's triangle (posterior midline weakness) predisposes to Zenker's diverticulum
Lower Esophageal Sphincter (LES)
-
NOT a true anatomic sphincter - it is a 3-4 cm zone of high pressure (15-25 mmHg resting) at the GEJ, extending 1-2 cm above and below the diaphragm
-
A functional/physiological sphincter created by:
- Intrinsic smooth muscle tone (dominant mechanism)
- Angle of His (oblique angle of esophagogastric junction)
- Diaphragmatic crura acting as an external squeeze during inspiration
- Phrenoesophageal ligament (Laimer's membrane)
- Intraabdominal positive pressure on abdominal esophageal segment
-
Factors increasing LES tone (prevent reflux): gastrin, motilin, substance P, alpha-adrenergic agonists, metoclopramide, acetylcholine
-
Factors decreasing LES tone (cause reflux): secretin, CCK, VIP, nitric oxide, beta-agonists, nitrates, calcium channel blockers, alcohol, fat
-
In hiatal hernia, the crural support and angle of His are disrupted → LES incompetence → GERD
10. Physiology of Swallowing
Three Phases
Oral phase (voluntary):
- Mastication, bolus formation, mixing with saliva
- Bolus pressed against faucial arches triggers pharyngeal phase
- CN IX and X afferents to brainstem swallowing center
Pharyngeal phase (involuntary, <1 second):
- Soft palate elevation (seals nasopharynx)
- Laryngeal elevation + epiglottic tilt (airway protection)
- Pharyngeal constrictor peristalsis
- UES relaxation (active dilation by laryngeal elevation)
Esophageal phase:
- Primary peristalsis: physiologic sequential constriction propagating at 2-4 cm/sec - propels bolus to stomach
- Secondary peristalsis: triggered by esophageal distension (not by swallowing) - clears residual food/acid
- Tertiary contractions: non-peristaltic, non-propulsive simultaneous contractions - abnormal (seen in presbyesophagus, DES)
Upper 1/3 (striated muscle): fastest transit (<1 second), voluntary
Lower 2/3 (smooth muscle): ~3 second transit, involuntary, under ENS + vagal control
Gravity plays only a minor role - peristalsis is the primary driver (swallowing in any position works).
11. Key Surgical Points Summary (MCh relevance)
| Feature | Surgical Relevance |
|---|---|
| No serosa | Higher anastomotic leak, early mediastinal tumor spread |
| Segmental blood supply | Devascularization risk in mobilization; anastomotic ischemia |
| Non-segmental lymphatics | Skip metastases; need extensive lymphadenectomy |
| No posterior raphe in cricopharyngeus | Killian's dehiscence → Zenker's diverticulum |
| LES is physiological, not anatomical | Disrupted by hiatal hernia; cannot be "tightened" anatomically without fundoplication |
| Angle of His | Absent in infants → infantile reflux; disrupted in hiatal hernia |
| RLN in TE groove | At risk in cervical esophageal surgery; right RLN more oblique - at risk in upper thoracic dissection |
| Vagal rotation | Anterior vagus = left; posterior = right; both trunks preserved in selective vagotomy |
| Porto-systemic anastomosis at GEJ | Esophageal varices in portal hypertension |
| EUS layers | T staging of esophageal cancer; planning EMR vs surgical resection |
Sources: Yamada's Textbook of Gastroenterology 7th ed.; K.J. Lee's Essential Otolaryngology; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Schwartz's Principles of Surgery 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.