Tell me angina in all detail with proper understanding with photos medicine mbbs
Reading File
Finding Sources
Finding Sources
Searching PubMed
angina pectoris management guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
I now have comprehensive content from Harrison's, Robbins, Goldman-Cecil, and Katzung. Let me compile the definitive MBBS-level angina answer.
Angina Pectoris - Complete MBBS Guide
Sources: Harrison's Principles of Internal Medicine 22E | Robbins & Cotran Pathologic Basis of Disease | Goldman-Cecil Medicine | Katzung's Basic & Clinical Pharmacology 16E
1. Definition
Angina pectoris is paroxysmal, recurrent chest discomfort caused by transient, reversible myocardial ischemia that is insufficient to cause myocyte necrosis. The ischemia triggers release of adenosine, bradykinin, and other metabolites that stimulate sympathetic and vagal afferent nerves, producing the characteristic pain.
- The word "angina" means choking/strangling; "pectoris" means chest.
- It is the most common clinical expression of myocardial ischemia.
- Males make up ~70% of all patients; in those <50 years, the proportion is even greater.
2. Pathophysiology - The Core Concept
The fundamental mechanism is an imbalance between myocardial oxygen demand and supply.
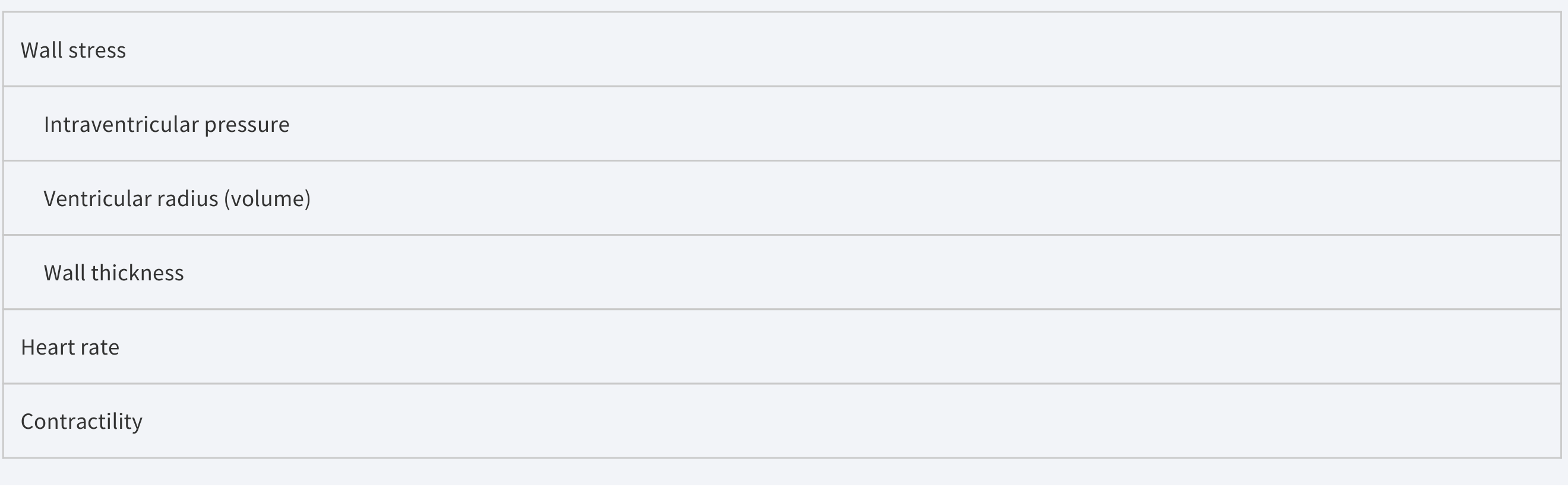
Determinants of Myocardial Oxygen DEMAND
| Factor | Effect |
|---|---|
| Wall stress | Increased by ↑ intraventricular pressure, ↑ ventricular radius (volume), ↓ wall thickness |
| Heart rate | ↑ HR → ↑ O₂ demand |
| Contractility | ↑ Contractility → ↑ O₂ consumption |
Determinants of Myocardial Oxygen SUPPLY
- Coronary blood flow is near zero during systole; perfusion occurs mainly in diastole.
- Flow = Aortic diastolic pressure / Coronary vascular resistance.
- At tachycardia, diastole shortens - this limits perfusion.
- Atherosclerotic plaques reduce luminal area and increase resistance.
- Endothelial damage impairs vasodilation (reduced NO synthesis).
Key Rule: Ischemia develops when demand exceeds supply, or when supply falls below the threshold of demand. - Goldman-Cecil Medicine
3. Types of Angina Pectoris
A. Stable (Typical) Angina - Most Common
- Caused by chronic fixed atherosclerotic stenosis of coronary arteries
- Occurs predictably with exertion, emotional stress, cold, meals, or tachycardia
- Does NOT occur at rest in a given patient
- Relieved within 2-5 minutes by rest or nitrates
- The plaque is stable; no thrombosis occurs
B. Unstable Angina (ACS)
- Increasingly frequent chest pain, precipitated by progressively less exertion or occurring at rest
- Pain lasts >20 minutes
- Caused by plaque disruption + superimposed thrombosis + vasospasm + distal embolization
- A medical emergency - harbinger of MI
- Most cases show evidence of myocyte injury (troponin may be mildly elevated)
- Distinguished from NSTEMI by negative troponin
C. Prinzmetal (Variant) Angina
- Uncommon; caused by coronary artery spasm (vasospasm)
- Occurs at rest, unrelated to physical activity, heart rate, or blood pressure
- Can affect normal or atherosclerotic vessels
- ECG shows ST-segment elevation (transient) during attack - opposite of stable angina
- Responds promptly to nitrates and calcium channel blockers
"Prinzmetal angina responds promptly to vasodilators such as nitroglycerin and calcium channel blockers." - Robbins & Kumar Basic Pathology
D. Silent Ischemia
- Ischemia without pain - particularly common in diabetic neuropathy and the elderly
- May manifest as dyspnea, nausea, palpitations, diaphoresis, or fatigue - or no symptoms at all
4. CCS Grading of Angina (Canadian Cardiovascular Society)
| Class | Description |
|---|---|
| I | Angina only with strenuous or prolonged physical activity; ordinary activity does not cause angina |
| II | Slight limitation of ordinary activity (walking >2 blocks, climbing >1 flight of stairs) |
| III | Marked limitation; angina with walking 1-2 blocks or climbing 1 flight of stairs |
| IV | Inability to carry on any activity without angina; angina at rest |
- Classes I-II = stable (chronic ischemic heart disease)
- Classes III-IV = severe/unstable
Source: Goldman-Cecil Medicine
5. Clinical Features (History)
Typical patient: Man >50 years or woman >60 years
Character of pain:
- Heaviness, pressure, squeezing, smothering, or choking - rarely described as "sharp"
- Located substernal or precordial
- Patient places a clenched fist over the sternum = Levine's sign
- Crescendo-decrescendo pattern - not most severe at onset
- Duration: 2-5 minutes (if >20 min, consider NSTEMI/STEMI)
Radiation:
- Left shoulder, down both arms (especially ulnar aspects)
- Jaw, teeth, neck, back, interscapular region, epigastrium
- Rarely radiates below the umbilicus or above the mandible
- Does NOT radiate to the trapezius (that pattern = pericarditis)
Precipitants (increase O₂ demand):
- Exercise, hurrying, sexual activity
- Emotional stress, anger, fright, frustration
- Cold weather (causes coronary vasoconstriction + ↑ afterload)
- Heavy meals
- Tachyarrhythmias
Relief:
- Rest (reduces demand)
- Sublingual nitroglycerin within 1-3 minutes
Associated symptoms:
- Dyspnea (LV dysfunction during ischemia)
- Diaphoresis, nausea (autonomic response)
- Nocturnal angina (angina decubitus) - patient awakened at night
6. Risk Factors
Modifiable:
- Hypertension, dyslipidemia (high LDL), diabetes mellitus
- Smoking, obesity, sedentary lifestyle
- Metabolic syndrome
Non-modifiable:
- Age (men >45, women >55)
- Male sex (women protected during reproductive years by estrogen)
- Family history of premature CAD (<55 in male relative, <65 in female)
Additional risk markers: Elevated CRP, coronary artery calcification on CT, increased carotid intimal thickness
7. Investigations
ECG (Electrocardiogram)
| Situation | ECG Finding |
|---|---|
| Resting ECG (stable angina, between episodes) | May be normal OR show Q waves (prior MI), T-wave changes |
| During angina episode (stable angina) | ST-segment depression (subendocardial ischemia) |
| During Prinzmetal angina attack | ST-segment elevation (transmural ischemia from spasm) |
| Exercise stress test | ST depression ≥1 mm at 60-80 ms after J-point = positive |
A positive exercise test: 2.5 mm ST depression at 5 METs is highly significant.
Echocardiography
- Assesses LV function, wall motion abnormalities (regional hypokinesis during ischemia)
- Rules out valvular causes (aortic stenosis can mimic angina)
Stress Testing
- Exercise ECG (treadmill) - Bruce protocol
- Stress echo or nuclear scintigraphy (Tc-99m sestamibi) - for higher sensitivity/specificity
- If unable to exercise: pharmacological stress (adenosine, dobutamine)
Coronary CT Angiography (CTA) / Calcium Scoring
- Coronary artery calcification (CAC) score correlates with atherosclerotic burden
- CTA: noninvasive anatomical assessment of stenosis severity
- Used as adjunctive information but not sole basis for decisions
Cardiac Biomarkers
- Troponin I/T: NORMAL in stable angina (ischemia but no necrosis)
- Troponin elevation distinguishes NSTEMI from unstable angina
Coronary Angiography (Catheterization) - Gold Standard
- Direct visualization of coronary anatomy
- Fractional flow reserve (FFR) assesses hemodynamic significance of stenosis
- Mandatory before revascularization
8. Pharmacology of Anti-Anginal Drugs
The three classic drug groups work by reducing the oxygen demand/supply mismatch:
A. Organic Nitrates (Nitroglycerin, Isosorbide dinitrate/mononitrate)
Mechanism of Action:
Nitrates are converted to nitric oxide (NO) intracellularly (via mitochondrial aldehyde dehydrogenase-2). NO activates guanylyl cyclase → ↑ cGMP → dephosphorylation of myosin light chains → vascular smooth muscle relaxation.
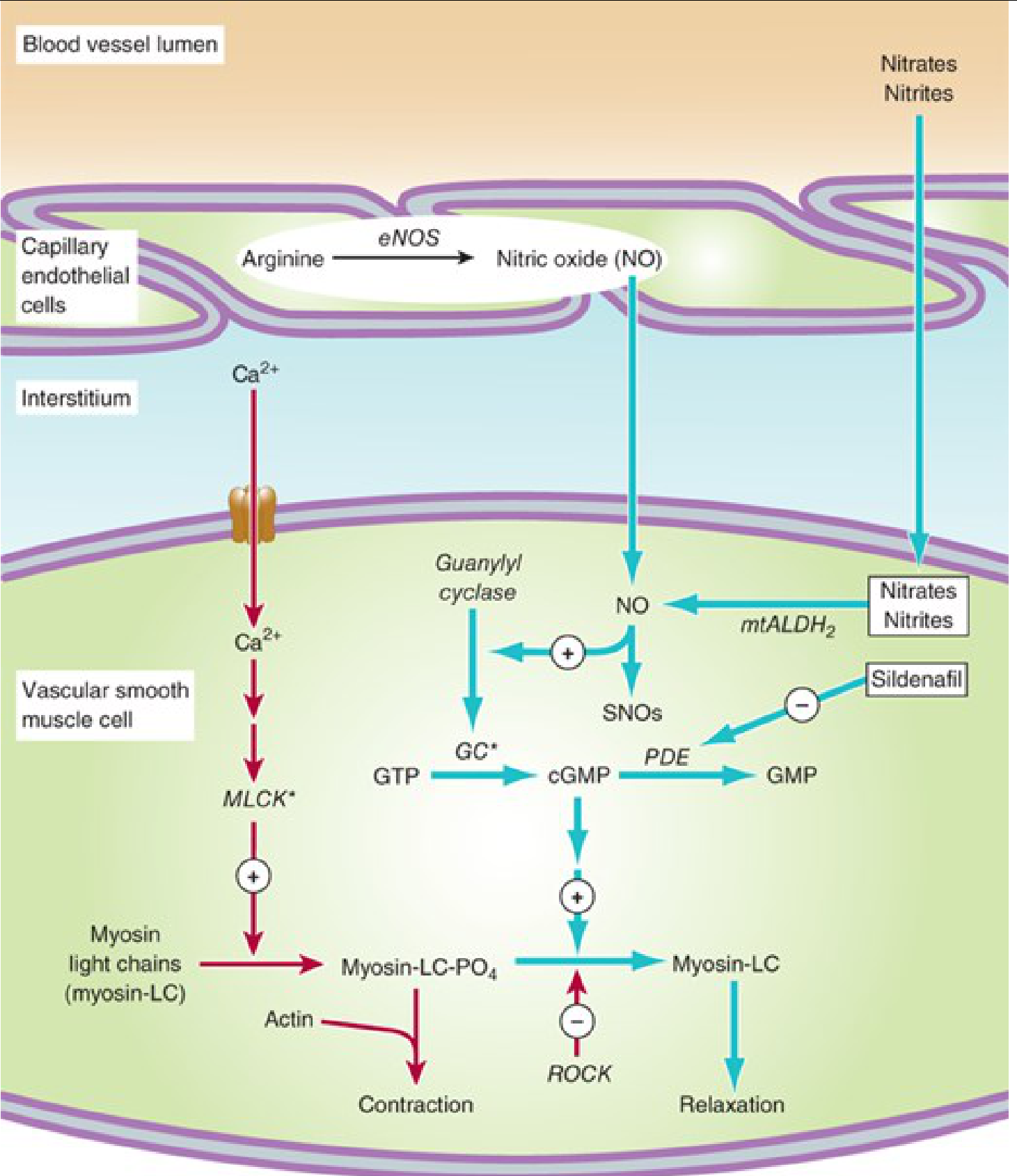
Effects:
- Venodilatation (dominant) → ↓ preload → ↓ ventricular volume → ↓ wall stress → ↓ O₂ demand
- Arterial dilatation → ↓ afterload
- Coronary vasodilation → ↑ supply (especially in variant angina)
Pharmacokinetics:
- Sublingual GTN: onset in minutes, duration 15-30 min; avoids first-pass metabolism
- Oral bioavailability <10-20% due to heavy hepatic first-pass
- Transdermal patches: sustained effect but tolerance develops
- Half-life: 2-8 minutes (active metabolites longer)
Tolerance: Develops with continuous use; requires a nitrate-free interval of 8-12 hours daily
ADRs: Headache (vasodilation), reflex tachycardia, hypotension, flushing
Contraindication: Concurrent PDE-5 inhibitors (sildenafil, tadalafil) - severe hypotension
Preparations:
| Drug | Route | Duration |
|---|---|---|
| Nitroglycerin (GTN) | Sublingual, transdermal, IV | 15-30 min (SL) |
| Isosorbide dinitrate | Oral | 4-6 hours |
| Isosorbide mononitrate | Oral | 6-10 hours |
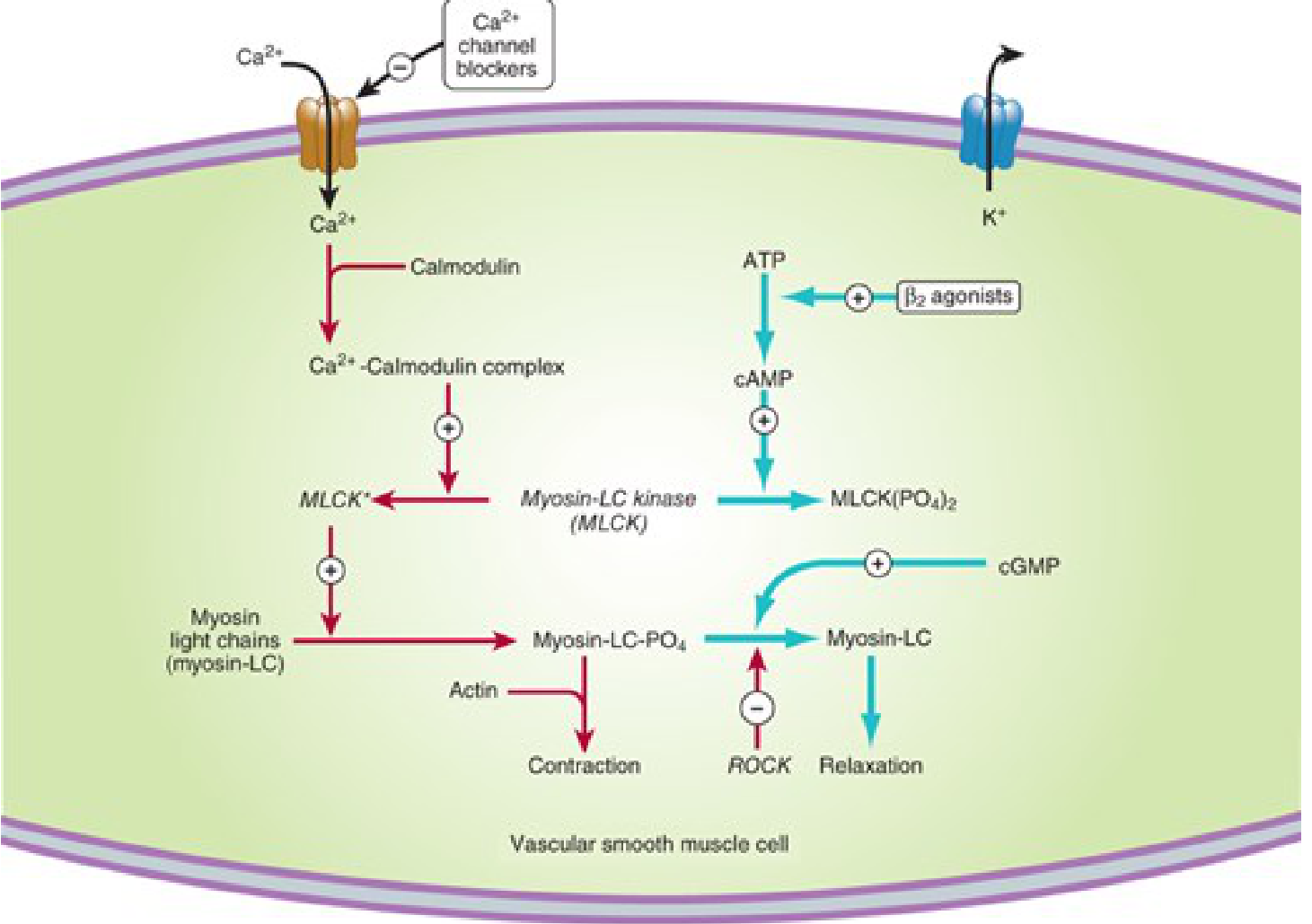
B. Beta-Adrenoceptor Blockers
Mechanism:
Block β₁ receptors → ↓ heart rate, ↓ contractility, ↓ blood pressure → ↓ myocardial O₂ demand.
Slowing HR also prolongs diastole → improves coronary filling time.
Drugs: Metoprolol (cardioselective), Atenolol, Bisoprolol, Propranolol (non-selective)
Benefits:
- Reduce frequency of anginal episodes
- Improve exercise tolerance
- Reduce mortality after MI (primary prevention of reinfarction)
- Cardioselective agents preferred (less bronchoconstriction)
Contraindications: Severe bradycardia, AV block, decompensated heart failure, asthma, Prinzmetal angina (may worsen vasospasm due to unopposed alpha stimulation)
C. Calcium Channel Blockers (CCBs)
Mechanism:
Block L-type Ca²⁺ channels → reduce intracellular Ca²⁺ → reduced smooth muscle and cardiac muscle contraction.
Types:
| Drug | Class | Selectivity | HR effect |
|---|---|---|---|
| Nifedipine | Dihydropyridine | Vascular > cardiac | ↑ HR (reflex) |
| Amlodipine | Dihydropyridine | Vascular > cardiac | Minimal |
| Verapamil | Phenylalkylamine | Cardiac > vascular | ↓↓ HR |
| Diltiazem | Benzothiazepine | Balanced | ↓ HR |
Benefits in Angina:
- Coronary vasodilation → ↑ supply
- Reduce afterload → ↓ demand
- Drug of choice in Prinzmetal angina (stop vasospasm)
- Verapamil/diltiazem also reduce HR
ADRs: Peripheral edema (dihydropyridines), bradycardia/heart block (verapamil/diltiazem), constipation (verapamil)
D. Ranolazine (Newer agent)
- Blocks the late inward sodium current (late I_Na)
- ↓ Na⁺ → ↓ Ca²⁺ overload via Na⁺/Ca²⁺ exchanger → less ischemic contracture
- Reduces angina without significantly affecting heart rate or BP
- Used as add-on therapy when standard agents insufficient
- Does NOT reduce mortality
E. Ivabradine
- Blocks the HCN (funny current, I_f) channel in the SA node
- Pure heart rate reduction without affecting contractility
- Used in patients intolerant to beta-blockers
9. Treatment Algorithm
Non-pharmacological (lifestyle modifications)
- Smoking cessation
- Weight loss, regular aerobic exercise (supervised cardiac rehab)
- Dietary modification (Mediterranean diet)
- Treatment of diabetes, hypertension, dyslipidemia
Pharmacological - Anti-ischemic
Step 1 (all patients):
- Sublingual GTN for acute relief
- Beta-blocker (first line for stable angina) - reduces events
Step 2 (if beta-blocker insufficient or contraindicated):
- Add long-acting nitrate or CCB
- Or switch to CCB (particularly dihydropyridine)
Step 3:
- Combination: beta-blocker + long-acting nitrate + CCB
- Ranolazine or ivabradine as add-on
Pharmacological - Secondary Prevention (MANDATORY)
| Drug | Rationale |
|---|---|
| Aspirin 75-100 mg daily | Antiplatelet - reduces MI risk |
| Statin (atorvastatin, rosuvastatin) | Plaque stabilization, LDL ↓, anti-inflammatory |
| ACE inhibitor/ARB | Reduces cardiac remodeling, beneficial in DM + HTN |
| Beta-blocker | Post-MI mortality reduction |
Revascularization
When to refer:
- CCS Class III-IV despite optimal medical therapy
- High-risk stress test findings (large territory of ischemia, EF <35%)
- Left main disease, 3-vessel disease (CABG preferred)
Options:
- PCI (Percutaneous Coronary Intervention): Angioplasty ± stent - for single/double vessel disease
- CABG (Coronary Artery Bypass Grafting): For left main, 3-vessel disease, diabetics with multi-vessel disease
2026 Evidence Update: A recent meta-analysis (PMID: 41130952) comparing medical management vs. PCI in stable angina confirms that for symptom relief PCI provides benefit, but for mortality outcomes optimal medical therapy remains competitive - patient selection is key.
10. Differential Diagnosis of Chest Pain
| Condition | Key Distinguishing Feature |
|---|---|
| Angina | Substernal, exertional, relieved by GTN |
| MI | Angina >20 min, not relieved by GTN, ↑ troponin |
| GERD/esophageal spasm | Relieved by antacids, postprandial, heartburn |
| Pericarditis | Sharp, positional, worse lying down, radiates to trapezius, friction rub |
| Aortic dissection | Tearing, radiates to back, BP difference between arms |
| Pulmonary embolism | Pleuritic pain, dyspnea, risk factors for DVT |
| MSK (costochondritis) | Reproducible on palpation, Tietze syndrome |
| Anxiety/panic | Atypical, young, + psychiatric history |
11. Complications of Untreated Angina
- Acute MI (plaque rupture + complete occlusion)
- Sudden cardiac death (ventricular fibrillation from ischemia)
- Heart failure (ischemic cardiomyopathy)
- Arrhythmias (PVCs, VT)
- Progression to unstable angina / ACS
12. Prognosis
Prognostic determinants (Harrison's 22E):
-
LV function (EF) - most important single predictor
-
Extent of coronary artery disease (number of vessels involved)
-
Severity of ischemia on stress testing
-
Age, additional risk factors (DM, HTN, dyslipidemia)
-
Evidence of prior MI
-
3-vessel disease + LV dysfunction: best treated with CABG
-
Left main disease: CABG preferred over PCI
Quick Summary Table
| Feature | Stable Angina | Unstable Angina | Prinzmetal Angina |
|---|---|---|---|
| Cause | Fixed atherosclerosis | Plaque rupture + thrombus | Coronary vasospasm |
| Trigger | Exertion | Rest or minimal exertion | Rest (often nocturnal) |
| Duration | 2-5 min | >20 min | Variable |
| ECG | ST depression | ST depression/T-wave changes | ST elevation |
| Troponin | Normal | Borderline/elevated (NSTEMI) | Normal |
| Treatment | GTN + BB + statin | ACS protocol (anticoagulation, PCI) | Nitrates + CCBs |
| GTN response | Yes | Partial/none | Yes |
References:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw-Hill - Chapter on Stable Angina Pectoris
- Robbins & Cotran Pathologic Basis of Disease - Chapter on Ischemic Heart Disease
- Robbins & Kumar Basic Pathology - Angina Pectoris
- Goldman-Cecil Medicine - Angina Pectoris and Chronic Ischemic Heart Disease; CCS Grading
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - Chapter 12: Vasodilators & Treatment of Angina Pectoris
- Upreti P et al. (2026) - Medical Management vs PCI in Stable Angina [PMID: 41130952]
This is a shared conversation. Sign in to Orris to start your own chat.