Leucopoiesis and it's regulation and it's clinical correlations
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
leukopoiesis regulation hematopoietic growth factors
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, detailed response.
Leukopoiesis: Formation, Regulation, and Clinical Correlations
1. Definition and Overview
Leukopoiesis (also spelled leucopoiesis) is the process of white blood cell (leukocyte) formation from hematopoietic stem cells (HSCs). It is one of three components of hematopoiesis, alongside erythropoiesis and thrombopoiesis. In adults, leukopoiesis occurs primarily in the red bone marrow of the axial skeleton (skull, vertebral bodies, pelvis, proximal long bones), with lymphopoiesis additionally occurring in the thymus, spleen, and lymph nodes.
The bone marrow produces more than 400 billion blood cells per day, and leukocyte production can increase dramatically in response to infection.
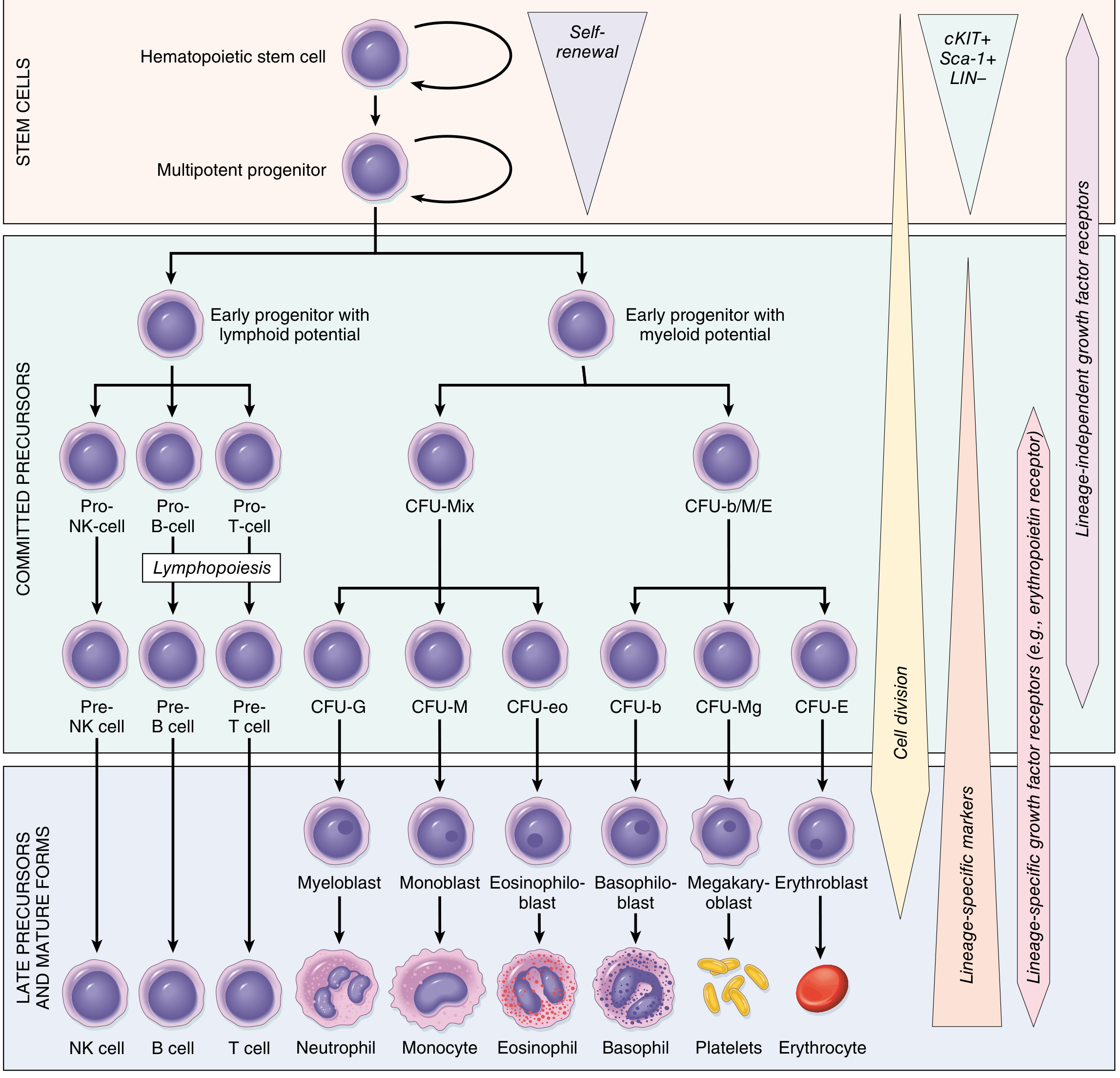
2. Stem Cell Hierarchy
All leukocytes originate from pluripotent HSCs, which have two cardinal properties:
- Pluripotency - ability to generate all mature blood cells
- Self-renewal - at least one daughter cell must self-renew to prevent stem cell depletion
HSCs reside in a specialized marrow niche maintained by stromal cells and secreted factors. They express surface markers cKIT+, Sca-1+, LIN-.
The HSC differentiates into two major progenitor branches:
| Progenitor | Gives rise to |
|---|---|
| Common Myeloid Progenitor (CMP) | Granulocytes (neutrophils, eosinophils, basophils), monocytes, megakaryocytes, erythrocytes |
| Common Lymphoid Progenitor (CLP) | T cells, B cells, NK cells |
From CMP, a Granulocyte-Monocyte Progenitor (GMP) is formed, which differentiates further under cytokine influence into distinct granulocyte lineages.
3. Granulopoiesis (Myeloid Leukopoiesis)
3.1 Six Morphological Stages of Neutrophil Maturation
The GMP differentiates into neutrophil progenitor (NoP) cells that undergo six sequential, morphologically identifiable stages:
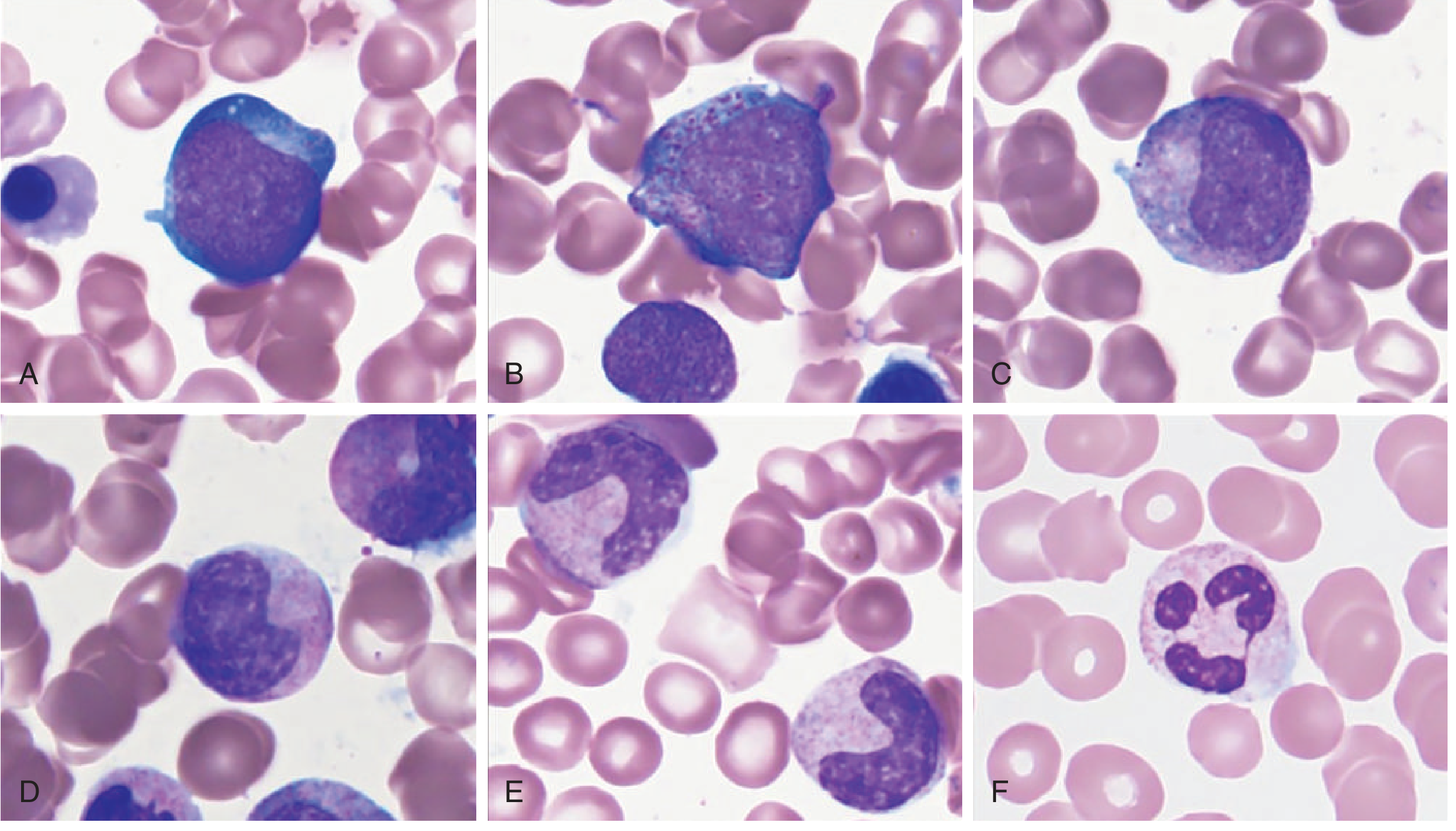
| Stage | Size | Nucleus | Cytoplasm / Key Feature |
|---|---|---|---|
| Myeloblast | 15-20 µm | Large, round, euchromatic; 3-5 nucleoli | Scant, deeply basophilic; agranular (first recognizable cell) |
| Promyelocyte | 12-24 µm (largest) | Round/ovoid; nucleoli still visible | Primary (azurophilic) granules appear; ONLY stage producing them |
| Myelocyte | 16-24 µm | More condensed; no nucleolus | Specific (secondary) granules appear - first stage where neutrophil/eosinophil/basophil lines can be distinguished; last mitotic stage |
| Metamyelocyte | 10-18 µm | Kidney-shaped (indented <half of width) | Abundant secondary granules; few azurophilic; postmitotic |
| Band (stab) cell | 9-15 µm | Horseshoe-shaped (indented >half of width); U/S/G-shaped | Pale cytoplasm with pink-tan secondary granules |
| Segmented neutrophil | 10-15 µm | 2-5 lobes joined by thin chromatin strands | Mature; enters circulation |
Key rule: In normal states, only mature neutrophils (segmented + occasional band forms up to 10%) circulate in peripheral blood. All stages are present in the bone marrow.
3.2 Eosinophil and Basophil Development
- Follow the same six morphological stages as neutrophils
- Cannot be distinguished from neutrophilic precursors until the myelocyte stage, when lineage-specific granules appear
- Eosinophilic myelocyte: large, eosin-pink secondary granules
- Basophilic myelocyte: dark blue-black metachromatic granules
- Basophil precursors are extremely difficult to identify in marrow smears due to their low numbers
3.3 Monocyte Development
- GMP cells can also give rise to monoblasts → promonocytes → monocytes under M-CSF influence
- Monocytes exit the marrow and become tissue macrophages (Kupffer cells, microglia, alveolar macrophages, Langerhans cells)
4. Lymphopoiesis
The CLP gives rise to T, B, and NK cells. Commitment depends on transcription factor expression:
| Lymphocyte | Transcription Factor | Site of Maturation |
|---|---|---|
| T lymphocytes | GATA-3 | Leave bone marrow as pre-T cells → mature in thymus → enter circulation as long-lived small T lymphocytes |
| B lymphocytes | Pax5 (activates B-cell-specific genes) | Develop in bone marrow, gut-associated lymphoid tissue, spleen ("bursa-equivalent organs") |
| NK cells | Unclear | Bone marrow (primary); also lymph nodes and fetal thymus |
Lymphocytes constitute up to 30% of all nucleated cells in the bone marrow. The Ikaros family of transcription factors plays a master role in HSC → CLP differentiation.
5. Bone Marrow Microenvironment
The marrow contains specialized sinusoids (thin-walled, lined by a single endothelial layer) separating the hematopoietic compartment from the peripheral circulation. Key features:
- Hematopoietic cells lie in "cords" between sinusoids
- Differentiated cells enter circulation by transcellular migration through endothelial cells
- Megakaryocytes lie adjacent to sinusoids and extend cytoplasmic processes to shed platelets
- Red cell precursors surround erythroblastic island macrophages that dispose of extruded nuclei
Red vs. Yellow marrow:
- Red marrow: hematopoietically active (children: throughout skeleton; adults: axial skeleton only)
- Yellow marrow: predominantly adipose cells, inactive (replaced in states of high demand)
6. Regulation of Leukopoiesis
6.1 Colony-Stimulating Factors (CSFs) and Cytokines
Regulation is achieved by hematopoietic growth factors - glycoproteins active at very low concentrations that interact synergistically (a process called "networking"):
| Growth Factor | Produced by | Primary Action |
|---|---|---|
| GM-CSF (Granulocyte-Macrophage CSF) | Endothelial cells, T cells, macrophages, mast cells, fibroblasts | Stimulates GMP cells to produce all granulocytes (neutrophils, eosinophils, basophils) AND monocytes |
| G-CSF (Granulocyte CSF) | Multiple sources | Specifically drives neutrophil differentiation, proliferation, and function; mobilizes HSCs from marrow |
| M-CSF (Monocyte/Macrophage CSF) | Multiple sources | Drives monocyte/macrophage differentiation |
| IL-3 | T cells | Broad multipotent growth factor; acts on early progenitors |
| IL-5 | T cells | Drives eosinophil differentiation from GMP; lack of IL-5 shifts toward basophil lineage |
| IL-2 + IL-15 | Stromal cells, T cells | NK cell differentiation |
| SCF (Stem Cell Factor / c-KIT ligand) | Stromal cells | Supports HSC survival and early progenitor expansion |
| Thrombopoietin | Liver, kidney | Megakaryocyte/platelet production |
Important principle: Lineage-committed growth factors (CSFs) act primarily at the CFU stage (mature progenitor level), amplifying cell output by up to 30-fold at that stage and a further 30-fold during maturation - generating >1000 mature cells per committed stem cell.
6.2 Transcription Factors
- C/EBPα - master regulator of granulopoiesis; mutated or silenced in many AML cases
- PU.1 - drives myeloid and monocyte lineage commitment
- Ikaros - master regulator of lymphopoiesis
- GATA-3 - T cell commitment
- Pax5 - B cell commitment
6.3 Marrow Storage and Peripheral Pools
Mature neutrophils are stored in a marrow reserve pool that can be rapidly mobilized. In the peripheral blood, neutrophils exist in two pools:
- Circulating pool (~50%) - those counted in the CBC
- Marginating pool (~50%) - adherent to vascular endothelium (not counted in CBC)
Demargination (e.g., from epinephrine or corticosteroids) shifts neutrophils from marginating to circulating pool, causing a pseudoneutrophilia without true increased production.
6.4 Myeloid:Erythroid (M:E) Ratio
Normal M:E ratio in bone marrow = 2:1 to 3:1 (some sources say 1.2:1 to 5:1 depending on method). A decreased M:E ratio (<1.2:1) may indicate depression of leukopoiesis or normoblastic hyperplasia. - Henry's Clinical Diagnosis and Management by Laboratory Methods
7. Normal Reference Ranges for Leukocytes (Adults)
(Robbins, Cotran & Kumar - Table 13.1)
| Cell Type | Normal Range |
|---|---|
| Total WBC | 4.8 - 10.8 × 10³/µL |
| Granulocytes | 40 - 70% |
| Neutrophils | 1.4 - 6.5 × 10³/µL |
| Lymphocytes | 1.2 - 3.4 × 10³/µL |
| Monocytes | 0.1 - 0.6 × 10³/µL |
| Eosinophils | 0 - 0.5 × 10³/µL |
| Basophils | 0 - 0.2 × 10³/µL |
8. Clinical Correlations
8.1 Quantitative Disorders
| Condition | Definition | Key Causes |
|---|---|---|
| Leukocytosis | WBC > 10.8 × 10³/µL | Infection, inflammation, malignancy, corticosteroids, stress |
| Neutrophilia | Neutrophils > 7 × 10³/µL | Bacterial infection, burns, AMI, myeloproliferative neoplasms, lithium therapy |
| Neutropenia | Neutrophils < 1.5 × 10³/µL | Chemotherapy, aplastic anemia, viral infections, autoimmune, drug-induced |
| Agranulocytosis | Neutrophils < 0.5 × 10³/µL | Severe drug toxicity (clozapine, methimazole, carbimazole), risk of life-threatening infection |
| Eosinophilia | Eosinophils > 0.5 × 10³/µL | Parasitic infection, allergy, asthma, drug reactions, lymphoma |
| Basophilia | Basophils > 0.1 × 10³/µL | CML (pathognomonic), hypothyroidism, allergic states |
| Leukopenia | WBC < 4.8 × 10³/µL | Viral infections, SLE, drug toxicity, aplastic anemia, B12/folate deficiency |
| Lymphocytosis | Lymphocytes > 3.4 × 10³/µL | Viral infections (EBV, CMV), CLL, pertussis |
Lithium causes leukocytosis by a direct effect on leukopoiesis (not just demargination) - this effect has been exploited therapeutically in neutropenia. - Katzung's Basic and Clinical Pharmacology
8.2 Neoplastic Disorders of Leukopoiesis
| Disorder | Key Pathology |
|---|---|
| Acute Myeloid Leukemia (AML) | Maturation arrest at blast stage (>20% blasts); mutations block C/EBPα or activate proliferative signaling. Auer rods are pathognomonic - crystalline aggregates of azurophilic granules seen in myeloblasts |
| Acute Promyelocytic Leukemia (APL / AML-M3) | t(15;17) - PML-RARα fusion; block at promyelocyte stage; risk of DIC; responsive to ATRA |
| Chronic Myeloid Leukemia (CML) | BCR-ABL1 (t(9;22), Philadelphia chromosome); unregulated granulopoiesis; all stages present in blood; characteristic basophilia |
| Acute Lymphoblastic Leukemia (ALL) | Lymphoid blast proliferation; most common childhood cancer |
| Chronic Lymphocytic Leukemia (CLL) | Monoclonal B cell accumulation; most common adult leukemia |
| Myelodysplastic Syndromes (MDS) | Clonal HSC disorders; ineffective hematopoiesis; cytopenias despite hypercellular marrow |
Pathogenesis shared principle (Robbins): Hematopoietic tumors arise from mutations that either block progenitor cell maturation or abrogate growth factor dependence, leading to unregulated clonal expansion replacing normal marrow progenitors.
8.3 Bone Marrow Failure
- Aplastic anemia: destruction or suppression of HSC pool → pancytopenia (all lineages reduced including WBCs)
- Infiltrative processes: metastatic cancer, granulomatous disease, myelofibrosis → displace normal hematopoietic cells
- Nutritional deficiencies: B12/folate deficiency causes megaloblastic changes affecting all lineages; B12 replacement normalizes leukopoiesis within 12-14 days and leukocyte counts return to normal within 1 week
8.4 Paraneoplastic Leukopoiesis
Tumors can ectopically secrete CSFs, causing paraneoplastic granulocytosis (approximately 30% of solid tumors). - Harrison's Principles of Internal Medicine
| Syndrome | Mediator | Associated Cancers |
|---|---|---|
| Granulocytosis | G-CSF, GM-CSF, IL-6 | Lung, GI, ovarian, genitourinary, Hodgkin's |
| Eosinophilia | IL-5 | Lymphoma, leukemia, lung cancer |
8.5 Pharmacological Applications
| Drug/Agent | Mechanism | Clinical Use |
|---|---|---|
| Filgrastim (recombinant G-CSF) | Stimulates neutrophil production and release | Chemotherapy-induced neutropenia, stem cell mobilization for transplant, severe congenital neutropenia |
| Sargramostim (GM-CSF) | Stimulates myeloid and monocyte production | Post-BMT engraftment, AML recovery, graft failure |
| Lithium | Directly stimulates leukopoiesis | Investigational use in neutropenia |
| Clozapine | Suppresses leukopoiesis | Requires mandatory WBC monitoring; risk of agranulocytosis |
| Dopamine receptor antagonists | Transient depression of leukopoiesis | Monitor WBC in patients on antipsychotics |
| Chemotherapy | Kills rapidly dividing cells (including myeloid progenitors) | Dose-limiting toxicity is neutropenia; G-CSF used to mitigate |
8.6 "Left Shift" (Bandemia)
When leukopoiesis is pushed to maximum output (severe infection, physiologic stress), immature neutrophil precursors appear in peripheral blood - a "left shift":
- Band cells (up to 10% in normal states)
- Metamyelocytes
- Occasionally myelocytes in severe cases
- Hypersegmented neutrophils (>5 lobes) = "right shift" seen in B12/folate deficiency (ineffective nuclear maturation)
Summary Diagram
Pluripotent HSC
│
├─── CMP ─── GMP ─── NoP ─── Myeloblast → Promyelocyte → Myelocyte → Metamyelocyte → Band → Neutrophil
│ │ (first specific granules; last mitosis)
│ ├───────────────────────────────────────────────────────────────────────────── Eosinophil
│ ├───────────────────────────────────────────────────────────────────────────── Basophil
│ └─── Monoblast → Promonocyte → Monocyte → Tissue Macrophage
│
└─── CLP ─── Pro-B cell → Pre-B cell → B lymphocyte (Pax5)
├─ Pro-T cell → Pre-T cell → Thymus → T lymphocyte (GATA-3)
└─ Pre-NK cell → NK cell (IL-2, IL-15)
Regulation: G-CSF (neutrophils), GM-CSF (all myeloid), M-CSF (monocytes), IL-5 (eosinophils),
IL-3 (multipotent), SCF (stem cells), Ikaros/Pax5/GATA-3 (lymphoid)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Histology: A Text and Atlas (Ross & Pawlina); Tietz Textbook of Laboratory Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's Principles of Internal Medicine 22E; Katzung's Basic and Clinical Pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.