GCS scale for nursing foundation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete nursing foundation guide to the Glasgow Coma Scale (GCS):
Glasgow Coma Scale (GCS) - Nursing Foundation
The GCS was originally developed in 1974 and is the most widely used scale to quickly assess level of consciousness, particularly after possible traumatic brain injury (TBI). It is a repetitive, reproducible scale that allows for ongoing neurologic monitoring by nurses.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
- Sabiston Textbook of Surgery, 11th Ed.
The Three Components
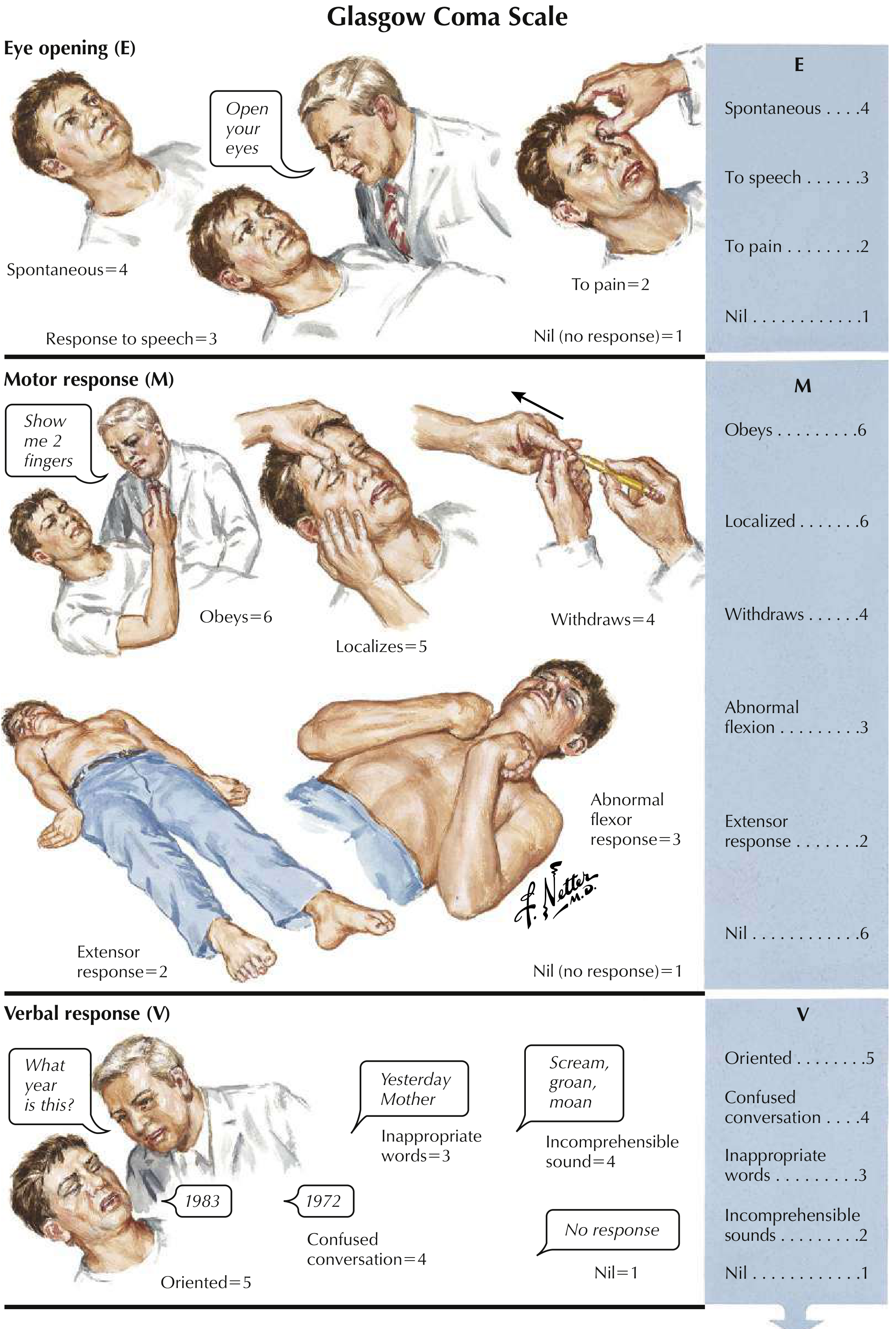
1. Eye Opening (E) - Maximum 4 points
| Score | Response |
|---|---|
| 4 | Eyes open spontaneously (without any stimulation) |
| 3 | Eyes open to verbal command (speech) |
| 2 | Eyes open to pain (e.g., sternal rub, nail bed pressure) |
| 1 | No eye opening (nil) |
2. Motor Response (M) - Maximum 6 points
| Score | Response |
|---|---|
| 6 | Obeys commands (e.g., "show me 2 fingers") |
| 5 | Localizes pain (purposeful movement toward painful stimulus) |
| 4 | Withdrawal from pain (pulls away from stimulus) |
| 3 | Abnormal flexion (decorticate posturing - arms flex inward) |
| 2 | Extension response (decerebrate posturing - arms extend outward) |
| 1 | No motor response (nil) |
3. Verbal Response (V) - Maximum 5 points
| Score | Response |
|---|---|
| 5 | Oriented (knows person, place, time - e.g., answers "What year is this?" correctly) |
| 4 | Confused conversation (responds but disoriented) |
| 3 | Inappropriate words (random words, no coherent conversation) |
| 2 | Incomprehensible sounds (moaning, groaning, no words) |
| 1 | No verbal response (nil) |
Total GCS Score (3-15)
| Total Score | Interpretation |
|---|---|
| 13-15 | Mild brain injury / normal consciousness |
| 9-12 | Moderate brain injury |
| 8 or less | Severe brain injury (GCS ≤8 = coma, consider intubation) |
| 3 | Lowest possible score (deep coma/death) |
Key nursing rule: GCS score ≤8 indicates loss of protective airway reflexes - the patient may need intubation and mechanical ventilation.
How to Record GCS
Always record each component separately, not just the total:
Example: E3 V4 M5 = GCS 12 (moderate brain injury)
The mnemonic "EMV" helps remember the order:
- E - Eye opening
- M - Motor response
- V - Verbal response
Nursing Tips for Assessment
- Start with verbal stimulation before painful stimuli
- Use standardized painful stimuli: central pain (supraorbital pressure, sternal rub) or peripheral (nail bed pressure)
- Document each component (E, M, V) individually - do not just write the total
- Reassess regularly and compare trends - deterioration is more important than a single reading
- Modifiers: Use "T" (e.g., VT) if the patient is intubated and cannot speak; use "C" if eyes are closed due to swelling
Comparison with Related Scales (Quick Reference)
| Scale | Use |
|---|---|
| GCS | Standard consciousness assessment (E+M+V, 3-15) |
| AVPU | Simpler bedside screen: Alert / Voice / Pain / Unresponsive |
| FOUR Score | Used in ICU; can assess brainstem reflexes even in intubated patients |
The AVPU scale is a simplified alternative often used in initial nursing triage:
- A - Alert and oriented
- V - Responds to Voice
- P - Responds to Pain
- U - Unresponsive
Sources: Plum and Posner's Diagnosis and Treatment of Stupor and Coma | Sabiston Textbook of Surgery, 11th Ed. | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.